Vous aimerez peut-être aussi
- Dr. Dan Siegel - Resources - Healthy Mind PlatterDocument4 pagesDr. Dan Siegel - Resources - Healthy Mind PlatterInês Novais100% (4)
- RISK ASSESSMENT REPORT - George Municipality - Tender ENG0042016 Installation of Perimeter Concrete Palisade FeDocument10 pagesRISK ASSESSMENT REPORT - George Municipality - Tender ENG0042016 Installation of Perimeter Concrete Palisade FeemmyPas encore d'évaluation
- Lippincott ProceduresDocument3 pagesLippincott ProceduresYmon TuallaPas encore d'évaluation
- Decontamination and SterilizationDocument7 pagesDecontamination and SterilizationStanley SibandaPas encore d'évaluation
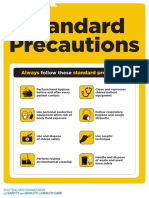
- Approach 4 Standard Precautions Icon PDF 672KBDocument1 pageApproach 4 Standard Precautions Icon PDF 672KBElaine MacalandaPas encore d'évaluation
- Philippine Constitution - Civil Service Exam ReviewerDocument41 pagesPhilippine Constitution - Civil Service Exam ReviewerYzza Veah Esquivel50% (2)
- Different Committees in The HospitalDocument8 pagesDifferent Committees in The HospitalShehnaz SheikhPas encore d'évaluation
- Elc590 Informative Speech About InsomniaDocument5 pagesElc590 Informative Speech About InsomniaANGJELLY ALLYA NGAUHPas encore d'évaluation
- INFECTION CONTROL 2nd YearDocument12 pagesINFECTION CONTROL 2nd YearAmy LalringhluaniPas encore d'évaluation
- TÉCNICAS DEL AUXILIAR DE ENFERMERÍA EN EL ÁREA DE QUIRÓFANOD'EverandTÉCNICAS DEL AUXILIAR DE ENFERMERÍA EN EL ÁREA DE QUIRÓFANOPas encore d'évaluation
- MAN-EMPOWERMENT - Strategies For Enhancing Autonomy and Control Over Nursing Practice PDFDocument10 pagesMAN-EMPOWERMENT - Strategies For Enhancing Autonomy and Control Over Nursing Practice PDFfriolan_cacliniPas encore d'évaluation
- Role of Nursing Staff in Patient Centric Care, Patient Safety and Hospital Infection ControlDocument31 pagesRole of Nursing Staff in Patient Centric Care, Patient Safety and Hospital Infection ControlVincy MacwanPas encore d'évaluation
- Surveillance Prevention and Control of Infection PlanDocument11 pagesSurveillance Prevention and Control of Infection Plansony kurniawanPas encore d'évaluation
- Vital Signs and Early Warning ScoresDocument47 pagesVital Signs and Early Warning Scoresdr_nadheem100% (1)
- Admitting A Patient .: Prepared by Ayugi Winnyfred Patience Bsc. Midwifery StudentDocument10 pagesAdmitting A Patient .: Prepared by Ayugi Winnyfred Patience Bsc. Midwifery StudentAYO NELSONPas encore d'évaluation
- Patient SafetyDocument22 pagesPatient SafetyRensy Sabi100% (1)
- The Management and Control of Hospital Acquired InfectionDocument21 pagesThe Management and Control of Hospital Acquired InfectionHarrison TravisPas encore d'évaluation
- File 571Document65 pagesFile 571RazaCreciaLastrillaMenesesPas encore d'évaluation
- Needle RecappingDocument4 pagesNeedle RecappingAyesha Calmerin PenuelaPas encore d'évaluation
- Surgical Site Marking PolicyDocument11 pagesSurgical Site Marking PolicymiraPas encore d'évaluation
- Infection Control Practices in WorkplaceDocument28 pagesInfection Control Practices in WorkplaceJames Patrick Dizon100% (1)
- Contrast and Special Radiographic Procedures: Topic - Aseptic TechniquesDocument15 pagesContrast and Special Radiographic Procedures: Topic - Aseptic TechniquesPOOJA MPas encore d'évaluation
- Cauti Prevention - UpdatedDocument25 pagesCauti Prevention - Updatedapi-340518242Pas encore d'évaluation
- CPG Management of Post-Operative Infectious EndophthalmitisDocument41 pagesCPG Management of Post-Operative Infectious EndophthalmitisnrajentranPas encore d'évaluation
- Annex G - Infection Control Annual Plan 2012-13Document7 pagesAnnex G - Infection Control Annual Plan 2012-13Tianti PuadiPas encore d'évaluation
- Aseptic TechniqueDocument9 pagesAseptic Techniquebethh_6Pas encore d'évaluation
- Infection Control NHS PolicyDocument12 pagesInfection Control NHS PolicyYahya Salem100% (1)
- Errors in NursingDocument59 pagesErrors in NursingCzerwin JualesPas encore d'évaluation
- Module 12: Infection Control in Health Care Settings: Image Courtesy Of: World Lung FoundationDocument37 pagesModule 12: Infection Control in Health Care Settings: Image Courtesy Of: World Lung FoundationAniruddhaPas encore d'évaluation
- Ipsg # 2017 PDFDocument30 pagesIpsg # 2017 PDFDARRYLARANHA100% (1)
- 14 Infection ControlDocument27 pages14 Infection ControlMichelle Joy M. VicentePas encore d'évaluation
- Prevention and Control of InfectionsDocument21 pagesPrevention and Control of InfectionsSunil ThomasPas encore d'évaluation
- Restraint Soctrative With AnswersDocument5 pagesRestraint Soctrative With AnswersKarren FernandezPas encore d'évaluation
- Iv Drug Preperation: Gina S. Cuenca, RN, MNDocument49 pagesIv Drug Preperation: Gina S. Cuenca, RN, MNJainah Rose Ferrer GubacPas encore d'évaluation
- Hemodialysis Central Venous Catheter STH ProtocolDocument2 pagesHemodialysis Central Venous Catheter STH ProtocolNor HilaliahPas encore d'évaluation
- Annual Infection Control Report Für 2021Document26 pagesAnnual Infection Control Report Für 2021Ruby Joyce AguilarPas encore d'évaluation
- Operating TheatreDocument26 pagesOperating TheatreStephen Pilar PortilloPas encore d'évaluation
- Universal Precaution by FithriDocument62 pagesUniversal Precaution by FithriFithriKurniatiPas encore d'évaluation
- Outbreak Control POLICYDocument11 pagesOutbreak Control POLICYAdrian SavastitaPas encore d'évaluation
- Chapter 2 HandwashingDocument18 pagesChapter 2 HandwashingMylene Valdez50% (2)
- 5.infection Control & Standard PrecautionsDocument33 pages5.infection Control & Standard PrecautionsGilbert JohnPas encore d'évaluation
- Infection Control Bundles For HospitalDocument12 pagesInfection Control Bundles For HospitalumeshbhartiPas encore d'évaluation
- IV Therapy ChecklistDocument3 pagesIV Therapy ChecklistJestoni SalvadorPas encore d'évaluation
- INFECTION CONTROL by Sandra WilsonDocument24 pagesINFECTION CONTROL by Sandra WilsonsandraPas encore d'évaluation
- Surgical Handwashing Resource Material 2023-2024Document9 pagesSurgical Handwashing Resource Material 2023-2024Cherry Louise O. SanvictoresPas encore d'évaluation
- Western Australian Patient Identification Policy PDFDocument14 pagesWestern Australian Patient Identification Policy PDFpuspadiniaPas encore d'évaluation
- Infection Control in ORDocument10 pagesInfection Control in ORaaminah tariqPas encore d'évaluation
- Infection Control ActivitiesDocument3 pagesInfection Control ActivitiesAileen A. MonaresPas encore d'évaluation
- Infection Control Program Flow ChartDocument1 pageInfection Control Program Flow ChartAnonymous ORleRrPas encore d'évaluation
- IPSGDocument16 pagesIPSGNyimas Milka Ayu NabilaPas encore d'évaluation
- Autoclave GuideDocument48 pagesAutoclave GuideIman 111Pas encore d'évaluation
- British Journal of Nursing Volume 14 Issue 10 2005 (Doi 10.12968/bjon.2005.14.10.18102) Preston, Rosemary M - Aseptic Technique - Evidence-Based Approach For Patient SafetyDocument6 pagesBritish Journal of Nursing Volume 14 Issue 10 2005 (Doi 10.12968/bjon.2005.14.10.18102) Preston, Rosemary M - Aseptic Technique - Evidence-Based Approach For Patient SafetyPriscilla CarmiolPas encore d'évaluation
- Theatre Infection Control Policy 2005Document15 pagesTheatre Infection Control Policy 2005parthotissPas encore d'évaluation
- Location at Time of Fall (Ward, Clinic, Service, Etc.) : - Inpatient Outpatient Date of Fall: Time of Fall (Military)Document5 pagesLocation at Time of Fall (Ward, Clinic, Service, Etc.) : - Inpatient Outpatient Date of Fall: Time of Fall (Military)Eduard RiparipPas encore d'évaluation
- Etiquette and PrinciplesDocument3 pagesEtiquette and PrinciplesHoney Bee S. PlatolonPas encore d'évaluation
- Image Courtesy Of: World Lung FoundationDocument37 pagesImage Courtesy Of: World Lung Foundationines syadzaPas encore d'évaluation
- COP 3 & PFR 1.5 - Care of Vulnerable PatientsDocument4 pagesCOP 3 & PFR 1.5 - Care of Vulnerable Patientsn_robinPas encore d'évaluation
- Central Sterile Supply Department: Mallikarjuna MHADocument25 pagesCentral Sterile Supply Department: Mallikarjuna MHAsandhyakrishnanPas encore d'évaluation
- Rating Scale: 0 Omitted 1 Poorly Done 2 Fairly Done 3 Well Done Indicates Critical Step Omission or Poor Performance Equates To FailureDocument3 pagesRating Scale: 0 Omitted 1 Poorly Done 2 Fairly Done 3 Well Done Indicates Critical Step Omission or Poor Performance Equates To FailureTemahlungwane100% (1)
- CSSD Performance Quality Analysis at A Super Speciality HospitalDocument29 pagesCSSD Performance Quality Analysis at A Super Speciality HospitalD. GandhirajPas encore d'évaluation
- Aceptic Techniques 1Document20 pagesAceptic Techniques 1RimaPas encore d'évaluation
- Ic-01-047 Infection Control in Operating RoomDocument13 pagesIc-01-047 Infection Control in Operating RoomDerick RanaPas encore d'évaluation
- Concepts of Infection ControlDocument61 pagesConcepts of Infection Controltummalapalli venkateswara rao100% (1)
- Handbook for Cssd Technicians: Understanding the Basics - Second EditionD'EverandHandbook for Cssd Technicians: Understanding the Basics - Second EditionPas encore d'évaluation
- Healthcare Environmental Services A Complete Guide - 2020 EditionD'EverandHealthcare Environmental Services A Complete Guide - 2020 EditionPas encore d'évaluation
- HepatitisDocument1 pageHepatitisAlma Moiselle LastimosaPas encore d'évaluation
- HepatitisDocument1 pageHepatitisAlma Moiselle LastimosaPas encore d'évaluation
- PRS-Team Leadership NursingDocument1 pagePRS-Team Leadership NursingAlma Moiselle LastimosaPas encore d'évaluation
- PRS Head NursingDocument1 pagePRS Head NursingAlma Moiselle LastimosaPas encore d'évaluation
- AnthraxDocument2 pagesAnthraxAlma Moiselle LastimosaPas encore d'évaluation
- Higher Algebra - Hall & KnightDocument593 pagesHigher Algebra - Hall & KnightRam Gollamudi100% (2)
- Handouts IMCIDocument5 pagesHandouts IMCIseigelystic100% (20)
- Handouts IMCIDocument5 pagesHandouts IMCIseigelystic100% (20)
- TEACHER Healthy Diet American English Upper Intermediate Advanced GroupDocument4 pagesTEACHER Healthy Diet American English Upper Intermediate Advanced GroupMarcus SabiniPas encore d'évaluation
- Fragility of MarriageDocument10 pagesFragility of MarriageMichellePas encore d'évaluation
- Domestic Violence Cycle of Violence Types of Families-2Document22 pagesDomestic Violence Cycle of Violence Types of Families-2api-340420872Pas encore d'évaluation
- Presentation 1Document16 pagesPresentation 1Azhari AhmadPas encore d'évaluation
- Pag-Unawa Sa Mga Panganib NG Sobrang Dosis NG Alkohol: Ano Ang Isang Pamantayang Tagay?Document5 pagesPag-Unawa Sa Mga Panganib NG Sobrang Dosis NG Alkohol: Ano Ang Isang Pamantayang Tagay?Rochelle Bartocillo BasquezPas encore d'évaluation
- The Influence of Music in Horror Games (Final Draft)Document7 pagesThe Influence of Music in Horror Games (Final Draft)Panther LenoXPas encore d'évaluation
- Covid-19 and Attitudes of Ground-Level Public Health Staff in Sri LankaDocument6 pagesCovid-19 and Attitudes of Ground-Level Public Health Staff in Sri LankaIJAR JOURNALPas encore d'évaluation
- Synthesis PaperDocument7 pagesSynthesis Paperapi-379148533Pas encore d'évaluation
- GENDER Reseach 100%3Document46 pagesGENDER Reseach 100%3Mesud GemechuPas encore d'évaluation
- Response To States 4.2 Motion in Limine Character of VictimDocument10 pagesResponse To States 4.2 Motion in Limine Character of VictimLaw of Self DefensePas encore d'évaluation
- NIH Public Access: Author ManuscriptDocument17 pagesNIH Public Access: Author ManuscriptJoyBoyXPas encore d'évaluation
- Nursing - Burn InjuryDocument39 pagesNursing - Burn Injuryamaracha2003Pas encore d'évaluation
- Handbook: Master of Social Work StudiesDocument26 pagesHandbook: Master of Social Work StudiesSukhman ChahalPas encore d'évaluation
- Fatima's CommissionDocument7 pagesFatima's CommissionSachie Daniela CheungPas encore d'évaluation
- Recreational Water Quality Guidelines and Aesthetics - IntroductionDocument3 pagesRecreational Water Quality Guidelines and Aesthetics - IntroductionLenin Jorge Villanueva DuranPas encore d'évaluation
- Hospital Pharmacy Communication - NewsletterDocument5 pagesHospital Pharmacy Communication - Newsletterjuveria nausheenPas encore d'évaluation
- 1120161049855Document16 pages1120161049855Ruchi SharmaPas encore d'évaluation
- CWU Psy 3Document8 pagesCWU Psy 3Codillia CheongPas encore d'évaluation
- Stress Management WorkbookDocument19 pagesStress Management WorkbookKATHYPas encore d'évaluation
- Tea and Industrial RevolutionDocument4 pagesTea and Industrial RevolutionPhuong NguyenPas encore d'évaluation
- J Villanueva Group 2Document22 pagesJ Villanueva Group 2Caryl Jole PaligsaPas encore d'évaluation
- Therapeutic Relationship Is Between Therapist and Patient and Has Always Been Viewed As SacredDocument3 pagesTherapeutic Relationship Is Between Therapist and Patient and Has Always Been Viewed As Sacredcbargrad100% (1)
- Burnout Among Secondary School Teachers in Malaysia Sabah: Dr. Balan RathakrishnanDocument8 pagesBurnout Among Secondary School Teachers in Malaysia Sabah: Dr. Balan Rathakrishnanxll21Pas encore d'évaluation
- Sq20-030 - Fact Sheet - Informed Consent - Nsqhs-8.9aDocument4 pagesSq20-030 - Fact Sheet - Informed Consent - Nsqhs-8.9aPedro Medeiros JrPas encore d'évaluation
- Example of A NHS Risk Rating MatrixDocument2 pagesExample of A NHS Risk Rating MatrixRochady SetiantoPas encore d'évaluation
- Smart and Sustainable Built Environment: Article InformationDocument14 pagesSmart and Sustainable Built Environment: Article Informationmikky jayPas encore d'évaluation