Vous aimerez peut-être aussi
- Unit - XI-Role of Nurse in Nutrition ProgrammeDocument82 pagesUnit - XI-Role of Nurse in Nutrition ProgrammeEllen AngelPas encore d'évaluation
- Chronic DiarrhoeaDocument9 pagesChronic DiarrhoeaDennis CobbPas encore d'évaluation
- Talk To Me Johnnie - John WelbournDocument993 pagesTalk To Me Johnnie - John WelbournYodarionPas encore d'évaluation
- Ultimate Soccer Fitness GuideDocument51 pagesUltimate Soccer Fitness GuideJerricJeevaPas encore d'évaluation
- Discharge Planning and NCP SDocument8 pagesDischarge Planning and NCP SRainier RamosPas encore d'évaluation
- A2 English Exam ReviewDocument4 pagesA2 English Exam ReviewJoshua CardenasPas encore d'évaluation
- The Vitamin Cure for Digestive DiseaseD'EverandThe Vitamin Cure for Digestive DiseaseÉvaluation : 5 sur 5 étoiles5/5 (4)
- Community Nutrition Teaching PlanDocument23 pagesCommunity Nutrition Teaching PlanBaljinder kaur91% (11)
- Maintaining Healthy LifestyleDocument6 pagesMaintaining Healthy LifestyleNoel Kl0% (1)
- Brightwok Kitchen MenuDocument1 pageBrightwok Kitchen MenuAshok SelvamPas encore d'évaluation
- Comprehensive 22-32 EngDocument160 pagesComprehensive 22-32 EngIsna AzizahPas encore d'évaluation
- El Efecto Del Kiwi en La Función de La Salud IntestinalDocument11 pagesEl Efecto Del Kiwi en La Función de La Salud IntestinalCatiuscia BarrilliPas encore d'évaluation
- Review: Treatment of Constipation in Older PeopleDocument8 pagesReview: Treatment of Constipation in Older PeopleMohd ZulAmirulPas encore d'évaluation
- Intractable Constipation in Elderly: Treatment OptionsDocument19 pagesIntractable Constipation in Elderly: Treatment OptionsLalito Manuel Cabellos AcuñaPas encore d'évaluation
- New Articles in This Journal Are Licensed Under A Creative Commons Attribution 4.0 United States LicenseDocument16 pagesNew Articles in This Journal Are Licensed Under A Creative Commons Attribution 4.0 United States Licenseandi hajrahPas encore d'évaluation
- Linakis2016 Article ChallengesAssociatedWithRouteO PDFDocument12 pagesLinakis2016 Article ChallengesAssociatedWithRouteO PDFEmilio Emmanué Escobar CruzPas encore d'évaluation
- Geriatric Constipation ManagementDocument7 pagesGeriatric Constipation ManagementAdy Adha NorsaniePas encore d'évaluation
- Admin,+6 +nisa +prevalence+of+constipation+and+lifestyleDocument9 pagesAdmin,+6 +nisa +prevalence+of+constipation+and+lifestylesalsabila JacobPas encore d'évaluation
- Konsensus Konstipasi 2010Document8 pagesKonsensus Konstipasi 2010Lidya Ayu LestariPas encore d'évaluation
- Gastroesophageal Reflux DiseaseDocument8 pagesGastroesophageal Reflux DiseaseGOURINANDHAPas encore d'évaluation
- Dietary Fiber and Its Effect On ObesityDocument13 pagesDietary Fiber and Its Effect On ObesitySusan FPas encore d'évaluation
- Diet in Benign Colonic Disorders: A Narrative ReviewDocument14 pagesDiet in Benign Colonic Disorders: A Narrative ReviewHouda LaatabiPas encore d'évaluation
- p2277 PDFDocument8 pagesp2277 PDFGoran TomićPas encore d'évaluation
- Askeb Kehamilan Fisiologis: Universitas Abulyatama Fakultas Kedokteran Prodi D4 Kebidanan Aceh Besar 2021/2022Document17 pagesAskeb Kehamilan Fisiologis: Universitas Abulyatama Fakultas Kedokteran Prodi D4 Kebidanan Aceh Besar 2021/2022Maulida TunsyifaPas encore d'évaluation
- 05 ConstipationDocument13 pages05 ConstipationNatanael NababanPas encore d'évaluation
- Diagnosis and Treatment of Chronic Constipation - A European PerspectiveDocument14 pagesDiagnosis and Treatment of Chronic Constipation - A European Perspectiveadinny julmizaPas encore d'évaluation
- Food and Drug InteractionDocument4 pagesFood and Drug InteractionRafaela SernagiottoPas encore d'évaluation
- Prescribing Medicines To Older People - How To Consider The Impact of Ageing On Human Organ and Body FunctionsDocument10 pagesPrescribing Medicines To Older People - How To Consider The Impact of Ageing On Human Organ and Body FunctionsEnzo VasquezPas encore d'évaluation
- Nutrients 14 00122 v2Document18 pagesNutrients 14 00122 v2Chon ChiPas encore d'évaluation
- Constipation ArticleDocument6 pagesConstipation ArticleDivyang BhaiPas encore d'évaluation
- Jurnal Smecta Khediri Et Al. 2011, Efficacy of Diosmectite (Smecta) in The Treatment of Acute Watery Diarrhoea in AdultsDocument8 pagesJurnal Smecta Khediri Et Al. 2011, Efficacy of Diosmectite (Smecta) in The Treatment of Acute Watery Diarrhoea in Adultsryan ardianPas encore d'évaluation
- The Effect of Zinc Supplementation in Adult Patients With Acute DiarrheaDocument5 pagesThe Effect of Zinc Supplementation in Adult Patients With Acute DiarrheaRizky AfriansyahPas encore d'évaluation
- Dysphagia, Dementia and Frailty: EditorialDocument5 pagesDysphagia, Dementia and Frailty: EditorialAlba FernándezPas encore d'évaluation
- Pediatric Bowel Management Program Improves Fecal IncontinenceDocument16 pagesPediatric Bowel Management Program Improves Fecal IncontinenceRhiza EchaPas encore d'évaluation
- Review: Epidemiology, Mechanisms, and Management of Diabetic GastroparesisDocument8 pagesReview: Epidemiology, Mechanisms, and Management of Diabetic GastroparesisIrma KurniawatiPas encore d'évaluation
- Pathophysiology of gastric acid in GI disordersDocument7 pagesPathophysiology of gastric acid in GI disordersCustom Essay WriterPas encore d'évaluation
- Cox 2020Document9 pagesCox 2020Mauricio LorcaPas encore d'évaluation
- New Horizons in Appetite and The Anorexia of AgeingDocument9 pagesNew Horizons in Appetite and The Anorexia of Ageingdevin mahendikaPas encore d'évaluation
- s11938-019-00231-8Document13 pagess11938-019-00231-8Nejc KovačPas encore d'évaluation
- A Guide To Fasting For MenopauseDocument12 pagesA Guide To Fasting For MenopauseConce RamirezPas encore d'évaluation
- Clinical Review: DyspepsiaDocument5 pagesClinical Review: Dyspepsiajenny puentesPas encore d'évaluation
- Kidneydial 02 00023Document13 pagesKidneydial 02 00023Lee Foo WengPas encore d'évaluation
- Preventing Opioid-Induced ConstipationDocument2 pagesPreventing Opioid-Induced Constipationaib reisPas encore d'évaluation
- Evaluation of ConstipationDocument8 pagesEvaluation of ConstipationAndrea GallegoPas encore d'évaluation
- Managing Gastrointestinal Complications of Diabetes: Joseph Sellin EditorDocument133 pagesManaging Gastrointestinal Complications of Diabetes: Joseph Sellin EditorRuth Desiyana GultomPas encore d'évaluation
- Probiotics and Constipation Mechanisms of Action Evidence For Effectiveness and Utilisation by Patients and Healthcare ProfessionalsDocument11 pagesProbiotics and Constipation Mechanisms of Action Evidence For Effectiveness and Utilisation by Patients and Healthcare ProfessionalsnganhaPas encore d'évaluation
- White Paper AGA: POWER - Practice Guide On Obesity and Weight Management, Education, and ResourcesDocument29 pagesWhite Paper AGA: POWER - Practice Guide On Obesity and Weight Management, Education, and ResourcesCin Gzlz PsicoPas encore d'évaluation
- Functional Gastrointestinal Disorders 3: SeriesDocument14 pagesFunctional Gastrointestinal Disorders 3: SeriesDimas RizkyPas encore d'évaluation
- Dyspepsia Risk Factors in IPB StudentsDocument18 pagesDyspepsia Risk Factors in IPB StudentsGalih Ayu PratiwiPas encore d'évaluation
- 01Document12 pages01whackjack_696977Pas encore d'évaluation
- A Time To FastDocument7 pagesA Time To Fastubiktrash1492Pas encore d'évaluation
- A Review On Colon Targeted Drug Delivery System: IJPSR (2019), Volume 10, Issue 1 (Review Article)Document10 pagesA Review On Colon Targeted Drug Delivery System: IJPSR (2019), Volume 10, Issue 1 (Review Article)VinayPas encore d'évaluation
- 77-File Utama Naskah-111-1-10-20181102Document6 pages77-File Utama Naskah-111-1-10-20181102Resti JayaPas encore d'évaluation
- Ferrara 2017Document5 pagesFerrara 2017nurharyanti darmaningtyasPas encore d'évaluation
- Review of The Treatment Options For Chronic ConstipationDocument21 pagesReview of The Treatment Options For Chronic Constipationcc verePas encore d'évaluation
- 03 KinightDocument4 pages03 Kinightcristina ArraisPas encore d'évaluation
- Evaluacion Disfagia Esofagica Adulto MayorDocument24 pagesEvaluacion Disfagia Esofagica Adulto MayorPaulina Culebro EspinozaPas encore d'évaluation
- A Time To FastDocument7 pagesA Time To Fastangela pavaPas encore d'évaluation
- Dehghan 2020Document15 pagesDehghan 2020showat nur chaninPas encore d'évaluation
- Jurnal Konstipasi KronikDocument10 pagesJurnal Konstipasi KronikIntan OctavianiPas encore d'évaluation
- Association Between Ultra-Processed Foods and Recurrence of Depressive Symptoms The Whitehall II Cohort StudyDocument14 pagesAssociation Between Ultra-Processed Foods and Recurrence of Depressive Symptoms The Whitehall II Cohort Studyangela.e.sanchezPas encore d'évaluation
- Dysphagia in The Elderly Management and Nutritional ConsiderationsDocument13 pagesDysphagia in The Elderly Management and Nutritional ConsiderationsGeraldo PaivaPas encore d'évaluation
- GastroparesisDocument10 pagesGastroparesisapi-437831510Pas encore d'évaluation
- Lifestyle Genetics-Based Reports in The Treatment of ObesityDocument13 pagesLifestyle Genetics-Based Reports in The Treatment of ObesityPavan MujawdiyaPas encore d'évaluation
- Evidence Supports Nutritional Support: EditorialDocument3 pagesEvidence Supports Nutritional Support: EditorialVitoria SilvaPas encore d'évaluation
- Malnutrition in the ElderlyD'EverandMalnutrition in the ElderlyW.O. SeilerPas encore d'évaluation
- Constipation: How To Treat Constipation: How To Prevent Constipation: Along With Nutrition, Diet, And Exercise For ConstipationD'EverandConstipation: How To Treat Constipation: How To Prevent Constipation: Along With Nutrition, Diet, And Exercise For ConstipationPas encore d'évaluation
- IDSA Releases Guidance On Antibiotic Selection For Gram-Negative Antimicrobial-Resistant Bacterial Infections - ACP Internist Weekly - ACP InternistDocument3 pagesIDSA Releases Guidance On Antibiotic Selection For Gram-Negative Antimicrobial-Resistant Bacterial Infections - ACP Internist Weekly - ACP InternistStacey WoodsPas encore d'évaluation
- Switching Ace-Inhibitors: Change To Change From Enalapril Quinapril RamiprilDocument2 pagesSwitching Ace-Inhibitors: Change To Change From Enalapril Quinapril RamiprilGlory Claudia KarundengPas encore d'évaluation
- Management of Bacterial and Fungal Infections in Cirrhosis JOH 2021Document17 pagesManagement of Bacterial and Fungal Infections in Cirrhosis JOH 2021Francisco Javier Gonzalez NomePas encore d'évaluation
- Id 397 TeicoplaninDocument2 pagesId 397 TeicoplaninStacey WoodsPas encore d'évaluation
- J Jacadv 2023 100389Document12 pagesJ Jacadv 2023 100389Edward ElBuenoPas encore d'évaluation
- Splenectomy Guideline Final 2012Document6 pagesSplenectomy Guideline Final 2012Stacey WoodsPas encore d'évaluation
- Antithrombotic Therapy For VTE DiseaseDocument13 pagesAntithrombotic Therapy For VTE DiseaseStacey WoodsPas encore d'évaluation
- 2023 ESPEN Practical and Partially Revised Guideline - Clinical Nutrition in The Intensive Care UnitDocument19 pages2023 ESPEN Practical and Partially Revised Guideline - Clinical Nutrition in The Intensive Care UnitStacey WoodsPas encore d'évaluation
- Antibiotik WhoDocument49 pagesAntibiotik WhodjebrutPas encore d'évaluation
- Palliative2 Nausea MedtableDocument2 pagesPalliative2 Nausea MedtableStacey WoodsPas encore d'évaluation
- Therapeutic Drug Monitoring in Adults at NUH2011 FinalDocument2 pagesTherapeutic Drug Monitoring in Adults at NUH2011 FinalStacey WoodsPas encore d'évaluation
- Critical CareDocument8 pagesCritical CareDzikrul Haq KarimullahPas encore d'évaluation
- Drug Information Center/KAUH: Selecting Gluten-Free Antibiotics in Celiac DiseaseDocument6 pagesDrug Information Center/KAUH: Selecting Gluten-Free Antibiotics in Celiac DiseaseStacey WoodsPas encore d'évaluation
- Multimorbidity Clinical Assessment and Management 1837516654789Document22 pagesMultimorbidity Clinical Assessment and Management 1837516654789Stacey WoodsPas encore d'évaluation
- Antibiotic Selection - The Clinical AdvisorDocument6 pagesAntibiotic Selection - The Clinical AdvisorStacey WoodsPas encore d'évaluation
- Antimicrobials at The End of LifeDocument2 pagesAntimicrobials at The End of LifeStacey WoodsPas encore d'évaluation
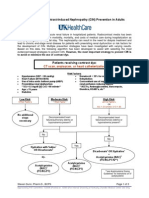
- Contrast NephRopathy GuidelinesDocument3 pagesContrast NephRopathy GuidelinesStacey WoodsPas encore d'évaluation
- Tamiflu PrescribingDocument26 pagesTamiflu PrescribingStacey WoodsPas encore d'évaluation
- Biomarkers of SepsisDocument8 pagesBiomarkers of SepsisStacey WoodsPas encore d'évaluation
- Potasio. 2014.Document19 pagesPotasio. 2014.Nestor Enrique Aguilar SotoPas encore d'évaluation
- Procoagulant GuidelineDocument30 pagesProcoagulant GuidelineStacey WoodsPas encore d'évaluation
- Fluid Choices Impact Outcome in Septic ShockDocument7 pagesFluid Choices Impact Outcome in Septic ShockStacey WoodsPas encore d'évaluation
- Elderly Patients Making Wise ChoicesDocument6 pagesElderly Patients Making Wise ChoicesStacey WoodsPas encore d'évaluation
- C.a.U.S.E. - Cardiac Arrest Ultra-Sound Exam - A Better Approach To Managing Patients in Primary Non-Arrhythmogenic Cardiac ArrestDocument2 pagesC.a.U.S.E. - Cardiac Arrest Ultra-Sound Exam - A Better Approach To Managing Patients in Primary Non-Arrhythmogenic Cardiac ArrestStacey WoodsPas encore d'évaluation
- Stimulant May Speed Antidepressant Response Time in ElderlyDocument3 pagesStimulant May Speed Antidepressant Response Time in ElderlyStacey WoodsPas encore d'évaluation
- StrokeDocument2 pagesStrokeStacey WoodsPas encore d'évaluation
- Preoperative Insulin 2013Document3 pagesPreoperative Insulin 2013Stacey WoodsPas encore d'évaluation
- Airway Clearance in The Intensive Care UnitDocument5 pagesAirway Clearance in The Intensive Care UnitStacey WoodsPas encore d'évaluation
- The ABC of Weaning Failure - A Structured ApproachDocument9 pagesThe ABC of Weaning Failure - A Structured ApproachArul ShanmugamPas encore d'évaluation
- 2nd G11 HOPE Module 2Document10 pages2nd G11 HOPE Module 2Sheryl FaelnarPas encore d'évaluation
- College of Nursing Case Study on Gestational DiabetesDocument32 pagesCollege of Nursing Case Study on Gestational DiabetesRich-Anne LagarasPas encore d'évaluation
- Anabolic Steroids HandoutDocument4 pagesAnabolic Steroids HandoutDiana AstriaPas encore d'évaluation
- Nutrition Needs: Daily Pre-Workout During Workout Post-WorkoutDocument1 pageNutrition Needs: Daily Pre-Workout During Workout Post-WorkoutS.odysseyPas encore d'évaluation
- Digestibility Determination in Fish Using Chromic Oxide Marking and Analysis of Contents From Different Segments of The Gastrointestinal TractDocument8 pagesDigestibility Determination in Fish Using Chromic Oxide Marking and Analysis of Contents From Different Segments of The Gastrointestinal TractRafael Hamakawa ViannaPas encore d'évaluation
- Nutrition LectureDocument2 pagesNutrition LectureIrwan M. IskoberPas encore d'évaluation
- ADULT Nutrition Screening Questionnaire 2Document1 pageADULT Nutrition Screening Questionnaire 2Alejandra López SalasPas encore d'évaluation
- Factors Affecting Food SelectionDocument1 pageFactors Affecting Food Selectioneunicebaldovino23Pas encore d'évaluation
- Journal 3 Personal Nutrition AssessmentDocument2 pagesJournal 3 Personal Nutrition Assessmentapi-456566589Pas encore d'évaluation
- Food Habits of India U-KDocument65 pagesFood Habits of India U-KTennety MrutyumjayaPas encore d'évaluation
- CHN LawsDocument4 pagesCHN LawsMarion JaoPas encore d'évaluation
- 16Document19 pages16phanisai100% (2)
- 150 FactsDocument13 pages150 Factsapi-256471149Pas encore d'évaluation
- Pancretic Cancer Case Study - BurkeDocument52 pagesPancretic Cancer Case Study - Burkeapi-282999254Pas encore d'évaluation
- LipidsDocument49 pagesLipidsAnumeha MittalPas encore d'évaluation
- Nutrition FSMDocument45 pagesNutrition FSMHema DeepikaPas encore d'évaluation
- Geriatric Constipation ManagementDocument7 pagesGeriatric Constipation ManagementAdy Adha NorsaniePas encore d'évaluation
- 3 PoshaDocument20 pages3 Poshav_vijayakanth7656Pas encore d'évaluation
- Physiological Psychology Study GuideDocument4 pagesPhysiological Psychology Study Guidemdelreal_22Pas encore d'évaluation
- The Effect of Indoor Rock Climbing On Strength, Endurance, and Flexibility Characteristics in Novice ClimbersDocument13 pagesThe Effect of Indoor Rock Climbing On Strength, Endurance, and Flexibility Characteristics in Novice ClimbersJournal of Theories and Application The International EditionPas encore d'évaluation
- Ebook Ebook PDF Introductory Foods 14Th Edition All Chapter PDF Docx KindleDocument41 pagesEbook Ebook PDF Introductory Foods 14Th Edition All Chapter PDF Docx Kindlevicki.lusk103100% (19)
- Lecture 9 - Resistance Training Program Design Part 2 Training CycleDocument22 pagesLecture 9 - Resistance Training Program Design Part 2 Training CycleRon Budnar100% (1)