Vous aimerez peut-être aussi
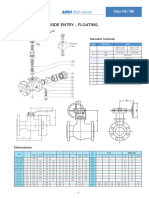
- Ball Valve DimensionDocument1 pageBall Valve DimensionridwanPas encore d'évaluation
- Appendix E - DisplacementDocument13 pagesAppendix E - DisplacementridwanPas encore d'évaluation
- Appendix B - Input ListingDocument11 pagesAppendix B - Input ListingridwanPas encore d'évaluation
- Appendix A - Caesar II ModelDocument1 pageAppendix A - Caesar II ModelridwanPas encore d'évaluation
- Spooling 2Document1 pageSpooling 2ridwanPas encore d'évaluation
- Appendix C - Stress SummaryDocument5 pagesAppendix C - Stress SummaryridwanPas encore d'évaluation
- Spooling 1Document1 pageSpooling 1ridwanPas encore d'évaluation
- Kirim Ke Pak SulthanDocument4 pagesKirim Ke Pak SulthanridwanPas encore d'évaluation
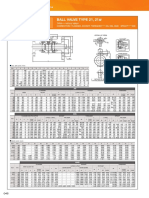
- Ball Valve Type 21, 21: ManualDocument1 pageBall Valve Type 21, 21: ManualridwanPas encore d'évaluation
- The Yellow House: A Memoir (2019 National Book Award Winner)D'EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Évaluation : 4 sur 5 étoiles4/5 (98)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceD'EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceÉvaluation : 4 sur 5 étoiles4/5 (895)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeD'EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeÉvaluation : 4 sur 5 étoiles4/5 (5794)
- The Little Book of Hygge: Danish Secrets to Happy LivingD'EverandThe Little Book of Hygge: Danish Secrets to Happy LivingÉvaluation : 3.5 sur 5 étoiles3.5/5 (399)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaD'EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaÉvaluation : 4.5 sur 5 étoiles4.5/5 (266)
- Shoe Dog: A Memoir by the Creator of NikeD'EverandShoe Dog: A Memoir by the Creator of NikeÉvaluation : 4.5 sur 5 étoiles4.5/5 (537)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureD'EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureÉvaluation : 4.5 sur 5 étoiles4.5/5 (474)
- Never Split the Difference: Negotiating As If Your Life Depended On ItD'EverandNever Split the Difference: Negotiating As If Your Life Depended On ItÉvaluation : 4.5 sur 5 étoiles4.5/5 (838)
- Grit: The Power of Passion and PerseveranceD'EverandGrit: The Power of Passion and PerseveranceÉvaluation : 4 sur 5 étoiles4/5 (588)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryD'EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryÉvaluation : 3.5 sur 5 étoiles3.5/5 (231)
- The Emperor of All Maladies: A Biography of CancerD'EverandThe Emperor of All Maladies: A Biography of CancerÉvaluation : 4.5 sur 5 étoiles4.5/5 (271)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyD'EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyÉvaluation : 3.5 sur 5 étoiles3.5/5 (2259)
- On Fire: The (Burning) Case for a Green New DealD'EverandOn Fire: The (Burning) Case for a Green New DealÉvaluation : 4 sur 5 étoiles4/5 (73)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersD'EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersÉvaluation : 4.5 sur 5 étoiles4.5/5 (344)
- Team of Rivals: The Political Genius of Abraham LincolnD'EverandTeam of Rivals: The Political Genius of Abraham LincolnÉvaluation : 4.5 sur 5 étoiles4.5/5 (234)
- The Unwinding: An Inner History of the New AmericaD'EverandThe Unwinding: An Inner History of the New AmericaÉvaluation : 4 sur 5 étoiles4/5 (45)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreD'EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreÉvaluation : 4 sur 5 étoiles4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)D'EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Évaluation : 4.5 sur 5 étoiles4.5/5 (121)
- Her Body and Other Parties: StoriesD'EverandHer Body and Other Parties: StoriesÉvaluation : 4 sur 5 étoiles4/5 (821)
- DM No. 2022-0511 Reporting of ZOD - 03oct2022Document9 pagesDM No. 2022-0511 Reporting of ZOD - 03oct2022Catherine LargaPas encore d'évaluation
- Health Care Economics CourseworkDocument3 pagesHealth Care Economics CourseworkcusoscylusPas encore d'évaluation
- Primary Health CareDocument41 pagesPrimary Health CareKailash NagarPas encore d'évaluation
- Medicare Objection and Rebuttals 2022Document4 pagesMedicare Objection and Rebuttals 2022Sam Jebasingh KirubhakaranPas encore d'évaluation
- Medical Insurance Guide - QLM - 2021Document12 pagesMedical Insurance Guide - QLM - 2021Murthy VvnPas encore d'évaluation
- Dovercourt Surgery: 3 Skye Edge Avenue Sheffield S2 5FXDocument4 pagesDovercourt Surgery: 3 Skye Edge Avenue Sheffield S2 5FXsafasayedPas encore d'évaluation
- Encyclopedia of Medical Decision MakingDocument1 266 pagesEncyclopedia of Medical Decision MakingAgam Reddy M100% (3)
- DR Tarek Tawfik Amin: Professor of Epidemiology Faculty of Medicine, Cairo University, EgyptDocument33 pagesDR Tarek Tawfik Amin: Professor of Epidemiology Faculty of Medicine, Cairo University, Egyptchipta lestariPas encore d'évaluation
- Methods: ResultsDocument8 pagesMethods: ResultsPrem Shankar GuptaPas encore d'évaluation
- Nursing Amendment Act 2018 Second Reading BriefDocument6 pagesNursing Amendment Act 2018 Second Reading BriefBernewsAdminPas encore d'évaluation
- Integrating Comprehensive Medication Management To Optimize Patient OutcomesDocument24 pagesIntegrating Comprehensive Medication Management To Optimize Patient OutcomesPatient-Centered Primary Care CollaborativePas encore d'évaluation
- Analisa Keselamatan Dan Kesehatan Kerja Pada Pembangunan Proyek Silktown Alexandria Tower ApartemenDocument7 pagesAnalisa Keselamatan Dan Kesehatan Kerja Pada Pembangunan Proyek Silktown Alexandria Tower ApartemenadeliaazmiPas encore d'évaluation
- Evidence Based PracticeDocument14 pagesEvidence Based PracticeAli RazaPas encore d'évaluation
- Sheet: Protecting Workers During A PandemicDocument3 pagesSheet: Protecting Workers During A Pandemicdhoo_babyPas encore d'évaluation
- Healthcare Domain TrainingDocument19 pagesHealthcare Domain TrainingShashank Raj50% (2)
- BCPC Accomplishment Report 2018Document2 pagesBCPC Accomplishment Report 2018pia97% (34)
- Innovation in Health Care Delivery: Jonathan Wilt AVP, Center For Innovation Ochsner Health SystemDocument47 pagesInnovation in Health Care Delivery: Jonathan Wilt AVP, Center For Innovation Ochsner Health SystemMedika UtamaPas encore d'évaluation
- Medicare: Part B Reopening Request FormDocument1 pageMedicare: Part B Reopening Request FormLukaPas encore d'évaluation
- Staffing Industry Analysts Recognizes Shari Dingle Costantini As A Leader in The Global 150 - Women in Staffing 2018Document2 pagesStaffing Industry Analysts Recognizes Shari Dingle Costantini As A Leader in The Global 150 - Women in Staffing 2018PR.comPas encore d'évaluation
- DPA Fact Sheet - Supervised Injection Facilities (Feb. 2016) PDFDocument2 pagesDPA Fact Sheet - Supervised Injection Facilities (Feb. 2016) PDFwebmaster@drugpolicy.orgPas encore d'évaluation
- Report Employee Training IPCDocument11 pagesReport Employee Training IPCDandi RawhidePas encore d'évaluation
- Bedside BrochureDocument2 pagesBedside Brochureapi-438607141100% (1)
- ICOHAP 2 - 1006 - CompressedDocument1 pageICOHAP 2 - 1006 - CompressederinaPas encore d'évaluation
- OHW NarrativeDocument5 pagesOHW NarrativeJESSICA ARNADOPas encore d'évaluation
- Disease ControlDocument20 pagesDisease Controlbibi bennyPas encore d'évaluation
- 10.daftar Pustaka PDFDocument3 pages10.daftar Pustaka PDFrosyadPas encore d'évaluation
- CHN Finals ExamDocument10 pagesCHN Finals ExamJhaynePas encore d'évaluation
- Women and BirthDocument13 pagesWomen and BirthRobithoh AlamsyahPas encore d'évaluation
- REPATRIATED OFW Final June 2, 2020Document24 pagesREPATRIATED OFW Final June 2, 2020Masinloc PS Zambales PpoPas encore d'évaluation
- 01 Soal LatihanDocument1 page01 Soal LatihanMuhammad Khairuna SyahPutraPas encore d'évaluation