Vous aimerez peut-être aussi
- Abdul Hakeem Hady.: Done byDocument29 pagesAbdul Hakeem Hady.: Done byعمر احمد شاكرPas encore d'évaluation
- Maternal Problems With PowerDocument2 pagesMaternal Problems With PowerAlex CvgPas encore d'évaluation
- Human Reproduction PDFDocument35 pagesHuman Reproduction PDFsqhaa100% (4)
- Abnormal Uterine ActionDocument110 pagesAbnormal Uterine ActionAnnapurna DangetiPas encore d'évaluation
- Chapter 24: Nursing Care of A Family During A Surgical Intervention For BirthDocument22 pagesChapter 24: Nursing Care of A Family During A Surgical Intervention For BirthAlyssaGrandeMontimorPas encore d'évaluation
- Absolute Obstetric Anesthesia Review: The Complete Study Guide for Certification and RecertificationD'EverandAbsolute Obstetric Anesthesia Review: The Complete Study Guide for Certification and RecertificationPas encore d'évaluation
- Paternity Leave LawDocument15 pagesPaternity Leave LawJohnny Castillo SerapionPas encore d'évaluation
- Difficult Airway in Obstetric AnesthesiaDocument3 pagesDifficult Airway in Obstetric AnesthesiaRoman AureliaPas encore d'évaluation
- Management of Normal LabourDocument37 pagesManagement of Normal LabourGlucose DRglucosePas encore d'évaluation
- Physiology of 1st Stage of LaborDocument134 pagesPhysiology of 1st Stage of LaborVijith.V.kumar50% (2)
- EpisiotomyDocument6 pagesEpisiotomyNishaThakuri100% (1)
- Subinvolution: Unit: IXDocument12 pagesSubinvolution: Unit: IXmikegrace0250% (2)
- Legal Medicine Set of Cases Part 1Document2 pagesLegal Medicine Set of Cases Part 1lalynPas encore d'évaluation
- Cephalopelvic DisproportionDocument7 pagesCephalopelvic DisproportionEli Ayase100% (1)
- Gynec and Obs. Topic Fetal DistressDocument45 pagesGynec and Obs. Topic Fetal DistressRajdeep ParmarPas encore d'évaluation
- Managament of The 2nd Stage of LabourDocument59 pagesManagament of The 2nd Stage of LabourJSeasharkPas encore d'évaluation
- History of RH Law in The PhilippinesDocument9 pagesHistory of RH Law in The PhilippinesAnonymous nYvtSgoQPas encore d'évaluation
- Induction of LaborDocument5 pagesInduction of LaborSimran SimzPas encore d'évaluation
- Dental Management of the Pregnant PatientD'EverandDental Management of the Pregnant PatientChristos A. SkouterisPas encore d'évaluation
- Rle FinalsDocument9 pagesRle FinalsMary Florence VelardePas encore d'évaluation
- Dysfunctional LaborDocument25 pagesDysfunctional Laborelleas24thPas encore d'évaluation
- 45-Fetal & Neonatal AsphyxiaDocument35 pages45-Fetal & Neonatal Asphyxiadr_asaleh100% (2)
- DystociaDocument31 pagesDystociamarsan120% (1)
- Module 4 Assignment SantiagoSibal NU 201Document4 pagesModule 4 Assignment SantiagoSibal NU 201Francisco Sibal IIIPas encore d'évaluation
- 365 Labour-Epidural-BasicsDocument5 pages365 Labour-Epidural-BasicsBilly AsifPas encore d'évaluation
- LASMARIAS IndivAct5Document25 pagesLASMARIAS IndivAct5AngelicaJaneA.SuanPas encore d'évaluation
- Abnormal LaborDocument20 pagesAbnormal Laborأ.م.د. إنعام فيصل محمدPas encore d'évaluation
- Prolonged Labour - Print DR AdilDocument2 pagesProlonged Labour - Print DR AdilAri Puji AstutiPas encore d'évaluation
- Prolonged LaborDocument23 pagesProlonged Laborsapana shahPas encore d'évaluation
- Precipitous LaborDocument15 pagesPrecipitous Laborelleas24thPas encore d'évaluation
- Cesarean DeliveryDocument6 pagesCesarean DeliveryShella Marie UsquisaPas encore d'évaluation
- C-Obs 16 Instrumental Vaginal Delivery Review Nov 12Document5 pagesC-Obs 16 Instrumental Vaginal Delivery Review Nov 12Yashdevil AtriPas encore d'évaluation
- Operative Vaginal Delivery (Ovd)Document35 pagesOperative Vaginal Delivery (Ovd)api-3705046Pas encore d'évaluation
- Course+Unit+Week+11 2Document9 pagesCourse+Unit+Week+11 2Kate RoquePas encore d'évaluation
- School of Health and Allied Health Sciences Nursing Department Self-Directed Learning (Nur 146 - Clinical Area)Document4 pagesSchool of Health and Allied Health Sciences Nursing Department Self-Directed Learning (Nur 146 - Clinical Area)Milagros FloritaPas encore d'évaluation
- ANESTHESIA in OBSTETRICSDocument159 pagesANESTHESIA in OBSTETRICSemma rose lutellaPas encore d'évaluation
- Week 7 NCM 109 LectureDocument25 pagesWeek 7 NCM 109 LecturePolicarpio AprilPas encore d'évaluation
- WEEK 7 NCM 109 LECTURE PPTX With Recorded DiscussionDocument26 pagesWEEK 7 NCM 109 LECTURE PPTX With Recorded DiscussionMa. Isabel A. EnriquezPas encore d'évaluation
- CHest Physio For NeonatesDocument7 pagesCHest Physio For Neonateschri23Pas encore d'évaluation
- Prolonged LabourDocument3 pagesProlonged Labourgeorgeloto12Pas encore d'évaluation
- DystociaDocument9 pagesDystociaRod Reynon BorcePas encore d'évaluation
- NRDS国教班Document39 pagesNRDS国教班raj patelPas encore d'évaluation
- Cesarean SectionDocument14 pagesCesarean Sectionمؤمن شطناويPas encore d'évaluation
- Maternity Exam 2 Self Made Study GuideDocument8 pagesMaternity Exam 2 Self Made Study GuidecheniahmPas encore d'évaluation
- PDF 075Document74 pagesPDF 075crystal_rc9Pas encore d'évaluation
- WEEK 5-NCM-109-LECTURE-PPTX With Recorded DiscussionDocument74 pagesWEEK 5-NCM-109-LECTURE-PPTX With Recorded DiscussionMa. Isabel A. EnriquezPas encore d'évaluation
- 6management of Labor (Updated)Document16 pages6management of Labor (Updated)uouoPas encore d'évaluation
- Module 4 Assignment Cortez and Salalila PDFDocument7 pagesModule 4 Assignment Cortez and Salalila PDFjennielunay00Pas encore d'évaluation
- Nursing Care PlansDocument4 pagesNursing Care PlansRITIK KUMARPas encore d'évaluation
- M PostpartumDocument23 pagesM PostpartumDonaJeanPas encore d'évaluation
- Intrapartum: Delivery Room Technique PurposeDocument7 pagesIntrapartum: Delivery Room Technique Purposesharmena harunPas encore d'évaluation
- Cord Presentation ProlapseDocument10 pagesCord Presentation ProlapseJHONESSA LAYOSPas encore d'évaluation
- Intrapartum DR TechniqueDocument10 pagesIntrapartum DR TechniqueAl-waleed JulkanainPas encore d'évaluation
- Intrapartum DR TechniqueDocument10 pagesIntrapartum DR TechniqueAl-waleed JulkanainPas encore d'évaluation
- Lesson 8 Pediatric NursingDocument21 pagesLesson 8 Pediatric NursingKristine Joy ManzanoPas encore d'évaluation
- Intrapartal Complications: Problems With The PowerDocument10 pagesIntrapartal Complications: Problems With The PowerkeinwayPas encore d'évaluation
- Pathophysiological Interpretation of Fetal Heart Rate Tracings in Clinical Practice AJOGDocument23 pagesPathophysiological Interpretation of Fetal Heart Rate Tracings in Clinical Practice AJOGMitsury Jacqueline Flores C.Pas encore d'évaluation
- NCM 109 L - Cesarean DeliveryDocument74 pagesNCM 109 L - Cesarean DeliveryRon Ar IcaPas encore d'évaluation
- Cord Clamping - Physiologic ApproachDocument13 pagesCord Clamping - Physiologic ApproachravyryPas encore d'évaluation
- JINGCO - BSN 2-D - Module-6-Storified-Case-ScenarioDocument13 pagesJINGCO - BSN 2-D - Module-6-Storified-Case-ScenarioJashtine JingcoPas encore d'évaluation
- DR Technique ChecklistDocument8 pagesDR Technique ChecklistChristine Joy MolinaPas encore d'évaluation
- Intrapartum: Delivery Room Technique PurposeDocument8 pagesIntrapartum: Delivery Room Technique PurposeRoshin TejeroPas encore d'évaluation
- DR Technique Checklist101Document8 pagesDR Technique Checklist101Christine Joy MolinaPas encore d'évaluation
- Intrapartum: Delivery Room Technique PurposeDocument8 pagesIntrapartum: Delivery Room Technique PurposeChristine Joy MolinaPas encore d'évaluation
- Care of Mother and Child at Risk or With Problems (Acute and Chronic)Document14 pagesCare of Mother and Child at Risk or With Problems (Acute and Chronic)Nicole Mendonis LunarPas encore d'évaluation
- MATERNALDocument14 pagesMATERNALjhenwilliamsPas encore d'évaluation
- FamilyDocument3 pagesFamilySyed Tanvir AhmedPas encore d'évaluation
- FCM 3 - 3A Group 8 - National AIDS STI Prevention and Control ProgramDocument184 pagesFCM 3 - 3A Group 8 - National AIDS STI Prevention and Control ProgramRenz Francis SasaPas encore d'évaluation
- Displacement of The UterusDocument32 pagesDisplacement of The UterusRaja100% (1)
- WGST Week 10 Quiz - Queer TheoryDocument7 pagesWGST Week 10 Quiz - Queer TheoryLiu Iwtsukun50% (2)
- Placental AbruptionDocument34 pagesPlacental Abruptionrosekatekate929Pas encore d'évaluation
- Debate Pro AbortionDocument5 pagesDebate Pro AbortionFirman Dwi CahyoPas encore d'évaluation
- THBT Woman Older Than 40 Should Not Have ChildrenDocument2 pagesTHBT Woman Older Than 40 Should Not Have ChildrenElma Nur HafizahPas encore d'évaluation
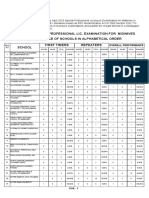
- April 2023 Special Professional Lic. Examination For MidwivesDocument2 pagesApril 2023 Special Professional Lic. Examination For MidwivesRapplerPas encore d'évaluation
- Family PlanningDocument18 pagesFamily PlanningPanchal JenishPas encore d'évaluation
- Ethical Issues in Maternal and Child Health NursingDocument11 pagesEthical Issues in Maternal and Child Health NursingIndah Dwi Jayanti0% (1)
- What Is Low Birth WeightDocument3 pagesWhat Is Low Birth WeightPrincess BartolomePas encore d'évaluation
- Ob Ward Timeline of ActivitiesDocument2 pagesOb Ward Timeline of Activitiesjohncarlo ramosPas encore d'évaluation
- KIK KI-1 PREGNANCY RELATED DEATH NOTIFICATION FORM Revised 2020Document1 pageKIK KI-1 PREGNANCY RELATED DEATH NOTIFICATION FORM Revised 2020syamimi amalinaPas encore d'évaluation
- Share Anatomy and Physiology CASE STUDY (Edited)Document3 pagesShare Anatomy and Physiology CASE STUDY (Edited)Glyndee Marr JagonobPas encore d'évaluation
- Bioethics and Its Application in Various Health Care SituationDocument8 pagesBioethics and Its Application in Various Health Care SituationDianne ObedozaPas encore d'évaluation
- Antepartum Fetal Surveillance ACOG Bulletin 2014 PDFDocument11 pagesAntepartum Fetal Surveillance ACOG Bulletin 2014 PDFDanPas encore d'évaluation
- Online Assignment 4Document15 pagesOnline Assignment 4Ab Staholic Boii100% (1)
- Menstrual Hygiene Industry in India October 2023Document36 pagesMenstrual Hygiene Industry in India October 2023Avinash GuptaPas encore d'évaluation
- 2018Andrology-Colpi-European Academy of Andrology Guideline Management of Oligo Astheno TeratozoospermiaDocument12 pages2018Andrology-Colpi-European Academy of Andrology Guideline Management of Oligo Astheno Teratozoospermiakong_666064846Pas encore d'évaluation
- Chapter 6 The Sexual Self e ModuleDocument25 pagesChapter 6 The Sexual Self e ModuleAl Francis DocilPas encore d'évaluation
- Sociology of Kinship - Assignment (PROCREATION)Document7 pagesSociology of Kinship - Assignment (PROCREATION)Mayank SinghPas encore d'évaluation
- Quarter II Health AshleyDocument46 pagesQuarter II Health AshleySarah Grace ManuelPas encore d'évaluation
- Physiology of Lactation: Prepared By: Fy MSC NursingDocument32 pagesPhysiology of Lactation: Prepared By: Fy MSC NursingSùjâl PätídàrPas encore d'évaluation
- Notes For HivDocument11 pagesNotes For HivEbenezar Paul Ratnaraj SPas encore d'évaluation