Vous aimerez peut-être aussi
- Healthcare Environmental Services A Complete Guide - 2020 EditionD'EverandHealthcare Environmental Services A Complete Guide - 2020 EditionPas encore d'évaluation
- IEHP Medi-Cal Members Rights and Responsibilities PDFDocument11 pagesIEHP Medi-Cal Members Rights and Responsibilities PDFminipower50Pas encore d'évaluation
- Neurodiagnostic TechnologyDocument3 pagesNeurodiagnostic TechnologyJeyarajasekar TtrPas encore d'évaluation
- Post Operative ComplicationsDocument18 pagesPost Operative ComplicationsamriezPas encore d'évaluation
- Medical Assitant ProjectDocument18 pagesMedical Assitant Projectapi-378167354100% (1)
- Patient Record MaintenanceDocument2 pagesPatient Record MaintenanceSai SridharPas encore d'évaluation
- @@assessment of Medical Documentation As Per Joint Commission InternationDocument6 pages@@assessment of Medical Documentation As Per Joint Commission InternationNahari ArifinPas encore d'évaluation
- Legal Implications Document A Schneider PDFDocument52 pagesLegal Implications Document A Schneider PDFAmrod Inglorion100% (2)
- Ahima Data Quality Management ModelDocument11 pagesAhima Data Quality Management Modelselinasimpson2301Pas encore d'évaluation
- Health Information TechnologyfinalDocument8 pagesHealth Information TechnologyfinalFranzia Izandra Alkuino Mojica100% (1)
- Nursing Home AdministratorDocument2 pagesNursing Home Administratorapi-78009605100% (1)
- NIH Adoption PolicyDocument4 pagesNIH Adoption PolicyABC7 WJLAPas encore d'évaluation
- Health Needs Assessment Maidstone Finalhealth Needs Assessment Maidstonefinal PDFDocument23 pagesHealth Needs Assessment Maidstone Finalhealth Needs Assessment Maidstonefinal PDFkoliosnf100% (1)
- Navigating Powerchart For Ed Ob orDocument2 pagesNavigating Powerchart For Ed Ob orapi-224958119Pas encore d'évaluation
- AMA Medical NecessityDocument3 pagesAMA Medical NecessityIrfan Gondal100% (1)
- A Comparative Analysis of The Philippine Nursing Curriculum From Other Countries.Document8 pagesA Comparative Analysis of The Philippine Nursing Curriculum From Other Countries.Alvin SantiagoPas encore d'évaluation
- Medical Office Management PDFDocument9 pagesMedical Office Management PDFAyessa Joy Tajale100% (1)
- Credential IngDocument13 pagesCredential Ingdr_rajatjainPas encore d'évaluation
- Timely Simple DischargeDocument52 pagesTimely Simple DischargeDesti Setyaningrum100% (1)
- EHT For Athletes For Brain HealthDocument2 pagesEHT For Athletes For Brain HealthTracey Jorg RollisonPas encore d'évaluation
- Hakim Seikh CaseDocument14 pagesHakim Seikh Caseronn13nPas encore d'évaluation
- JCAHO Medication Management Standards 2004Document10 pagesJCAHO Medication Management Standards 2004Afdhal MawardinPas encore d'évaluation
- Step 7 How - To - Conduct - A - Mock - Tracer PDFDocument10 pagesStep 7 How - To - Conduct - A - Mock - Tracer PDFRekhaPas encore d'évaluation
- Presentor-: Ruma Sen: MN (Previous) RakconDocument40 pagesPresentor-: Ruma Sen: MN (Previous) Rakconcy100% (1)
- Nationwide Health Information Network ExchangeDocument2 pagesNationwide Health Information Network ExchangeONC for Health Information TechnologyPas encore d'évaluation
- Medication Policy Sept 13Document3 pagesMedication Policy Sept 13parkadminPas encore d'évaluation
- The Model For ImprovementDocument17 pagesThe Model For Improvementapi-487551161100% (1)
- NHO Code of Practice For Healthcare Records Management Version 2 0Document370 pagesNHO Code of Practice For Healthcare Records Management Version 2 0Khirod SahuPas encore d'évaluation
- Front Office Staff Development 2007Document51 pagesFront Office Staff Development 2007Drishti DehradunPas encore d'évaluation
- Clinical Audit GuideDocument13 pagesClinical Audit Guidewassie gebiPas encore d'évaluation
- Standard of Care: Standard of Care Is That Care in Which A Reasonable Man Would Take inDocument10 pagesStandard of Care: Standard of Care Is That Care in Which A Reasonable Man Would Take invishakhaPas encore d'évaluation
- Medical Transcription Industry: Prepared byDocument27 pagesMedical Transcription Industry: Prepared byrohitpatel203100% (1)
- Bizmanualz Medical Office Policies and Procedures SampleDocument7 pagesBizmanualz Medical Office Policies and Procedures SampleallukazoldyckPas encore d'évaluation
- Sample of Job DescriptionsDocument48 pagesSample of Job DescriptionsLoresita Amoranto Rebong RNPas encore d'évaluation
- 3 Summary Guide Clinical Indicators 2012 (ACHS)Document48 pages3 Summary Guide Clinical Indicators 2012 (ACHS)Erniwati SilalahiPas encore d'évaluation
- Overview of Healthcare Interoperability Standards: Safer Better CareDocument38 pagesOverview of Healthcare Interoperability Standards: Safer Better CareAnis BEN JEMAA100% (1)
- Discharge Process SynopsisDocument7 pagesDischarge Process Synopsisdrbhavya250% (1)
- Chapter 3 Health Information TechnologyDocument66 pagesChapter 3 Health Information Technologygrasslovecow100% (1)
- 2010 SWOT Harrison - Chapter5 Health Administration Press, 2010Document7 pages2010 SWOT Harrison - Chapter5 Health Administration Press, 2010Fernando NingunoPas encore d'évaluation
- ACHS Clinical Indicator PDFDocument169 pagesACHS Clinical Indicator PDFTri Hastuti HendrayaniPas encore d'évaluation
- Meaningful Use Business Analyst in Atlanta GA Resume Margaret ChandlerDocument3 pagesMeaningful Use Business Analyst in Atlanta GA Resume Margaret ChandlerMargaretChandlerPas encore d'évaluation
- Documentation: Basic Nursing: Foundations of Skills & Concepts DocumentationDocument8 pagesDocumentation: Basic Nursing: Foundations of Skills & Concepts DocumentationJona GarzonPas encore d'évaluation
- Assg Codingcasestudies 20171109 Ah102 KPDocument1 pageAssg Codingcasestudies 20171109 Ah102 KPapi-427618755Pas encore d'évaluation
- Joint Commission TST Hand Hygiene Data Collection Tool PDFDocument5 pagesJoint Commission TST Hand Hygiene Data Collection Tool PDFJoel Guillen JulianPas encore d'évaluation
- Week 1Document73 pagesWeek 1Kimberly Jane TogñoPas encore d'évaluation
- Facts of Medical Record KeepingDocument4 pagesFacts of Medical Record KeepingSuraj SrivatsavPas encore d'évaluation
- The Therapy Place Informed Consent and Therapy Contract: Statement of FaithDocument5 pagesThe Therapy Place Informed Consent and Therapy Contract: Statement of FaithMax ElamPas encore d'évaluation
- Chapter 26Document46 pagesChapter 26meeeenonPas encore d'évaluation
- Handbook CredentialingDocument14 pagesHandbook CredentialingSugiarto SuwardiPas encore d'évaluation
- NABH Assessment - Institutional Ethics CommitteesDocument4 pagesNABH Assessment - Institutional Ethics CommitteesAmitKumarPas encore d'évaluation
- Prelim To Finals RT 203 1Document71 pagesPrelim To Finals RT 203 1Leopardas, Lynn Clemard C.100% (1)
- Collaborative CareDocument16 pagesCollaborative CareArdhani IrfanPas encore d'évaluation
- Scenario 12 - Ethics Committee Serves As GuardianDocument5 pagesScenario 12 - Ethics Committee Serves As GuardianVictoria100% (1)
- HASTING CENTER The Privacy Rule That's NotDocument11 pagesHASTING CENTER The Privacy Rule That's NotIon Arrieta ValeroPas encore d'évaluation
- Dictionary of Acronyms in HealthcareDocument1 353 pagesDictionary of Acronyms in HealthcaremeaningfulhealthitPas encore d'évaluation
- Essential Safety Requirements - Nursing Standards Accomplishment ReportDocument10 pagesEssential Safety Requirements - Nursing Standards Accomplishment ReportMARITES MACAPAGAL100% (1)
- Ch.8 Telephone Techniques WorkbookDocument4 pagesCh.8 Telephone Techniques WorkbookAndre AyalaPas encore d'évaluation
- Utilization Review Coordinator: Passbooks Study GuideD'EverandUtilization Review Coordinator: Passbooks Study GuidePas encore d'évaluation
- Patient Safety Organization A Complete Guide - 2020 EditionD'EverandPatient Safety Organization A Complete Guide - 2020 EditionPas encore d'évaluation
- ED Doc PolicyDocument4 pagesED Doc PolicyAlyssa AzucenaPas encore d'évaluation
- Documentation and NursingDocument52 pagesDocumentation and NursingAlyssa Azucena100% (1)
- Directing and Controlling Nursing ServiceDocument13 pagesDirecting and Controlling Nursing ServiceAlyssa AzucenaPas encore d'évaluation
- GMO Case Study (Half)Document10 pagesGMO Case Study (Half)Alyssa AzucenaPas encore d'évaluation
- The Electricity Act - 2003Document84 pagesThe Electricity Act - 2003Anshul PandeyPas encore d'évaluation
- Basic Vibration Analysis Training-1Document193 pagesBasic Vibration Analysis Training-1Sanjeevi Kumar SpPas encore d'évaluation
- Avalon LF GB CTP MachineDocument2 pagesAvalon LF GB CTP Machinekojo0% (1)
- Hip NormDocument35 pagesHip NormAiman ArifinPas encore d'évaluation
- Escario Vs NLRCDocument10 pagesEscario Vs NLRCnat_wmsu2010Pas encore d'évaluation
- Abu Hamza Al Masri Wolf Notice of Compliance With SAMs AffirmationDocument27 pagesAbu Hamza Al Masri Wolf Notice of Compliance With SAMs AffirmationPaulWolfPas encore d'évaluation
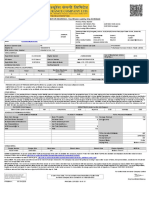
- MOTOR INSURANCE - Two Wheeler Liability Only SCHEDULEDocument1 pageMOTOR INSURANCE - Two Wheeler Liability Only SCHEDULESuhail V VPas encore d'évaluation
- Use of EnglishDocument4 pagesUse of EnglishBelén SalituriPas encore d'évaluation
- 199437-Unit 4Document36 pages199437-Unit 4Yeswanth rajaPas encore d'évaluation
- QA/QC Checklist - Installation of MDB Panel BoardsDocument6 pagesQA/QC Checklist - Installation of MDB Panel Boardsehtesham100% (1)
- Jerome4 Sample Chap08Document58 pagesJerome4 Sample Chap08Basil Babym100% (7)
- Lab Session 7: Load Flow Analysis Ofa Power System Using Gauss Seidel Method in MatlabDocument7 pagesLab Session 7: Load Flow Analysis Ofa Power System Using Gauss Seidel Method in MatlabHayat AnsariPas encore d'évaluation
- Doas - MotorcycleDocument2 pagesDoas - MotorcycleNaojPas encore d'évaluation
- Cs8792 Cns Unit 1Document35 pagesCs8792 Cns Unit 1Manikandan JPas encore d'évaluation
- 450i User ManualDocument54 pages450i User ManualThượng Lê Văn0% (2)
- Social Media Marketing Advice To Get You StartedmhogmDocument2 pagesSocial Media Marketing Advice To Get You StartedmhogmSanchezCowan8Pas encore d'évaluation
- 3125 Vitalogic 4000 PDFDocument444 pages3125 Vitalogic 4000 PDFvlaimirPas encore d'évaluation
- Subqueries-and-JOINs-ExercisesDocument7 pagesSubqueries-and-JOINs-ExerciseserlanPas encore d'évaluation
- Manufacturing StrategyDocument31 pagesManufacturing Strategyrajendra1pansare0% (1)
- 4109 CPC For ExamDocument380 pages4109 CPC For ExamMMM-2012Pas encore d'évaluation
- Hager Pricelist May 2014Document64 pagesHager Pricelist May 2014rajinipre-1Pas encore d'évaluation
- General Diesel Engine Diagnostic Guide PDFDocument3 pagesGeneral Diesel Engine Diagnostic Guide PDFan0th3r_0n3Pas encore d'évaluation
- EXTENDED PROJECT-Shoe - SalesDocument28 pagesEXTENDED PROJECT-Shoe - Salesrhea100% (5)
- Activity Description Predecessor Time (Days) Activity Description Predecessor ADocument4 pagesActivity Description Predecessor Time (Days) Activity Description Predecessor AAlvin LuisaPas encore d'évaluation
- Doterra Enrollment Kits 2016 NewDocument3 pagesDoterra Enrollment Kits 2016 Newapi-261515449Pas encore d'évaluation
- HSBC in A Nut ShellDocument190 pagesHSBC in A Nut Shelllanpham19842003Pas encore d'évaluation
- Seminar On Despute Resolution & IPR Protection in PRCDocument4 pagesSeminar On Despute Resolution & IPR Protection in PRCrishi000071985100% (2)
- Sample Annual BudgetDocument4 pagesSample Annual BudgetMary Ann B. GabucanPas encore d'évaluation
- CV Ovais MushtaqDocument4 pagesCV Ovais MushtaqiftiniaziPas encore d'évaluation
- Hotel ManagementDocument34 pagesHotel ManagementGurlagan Sher GillPas encore d'évaluation