Vous aimerez peut-être aussi
- FAQs - What Is An Egg Donor - Egg Donor in Mumbai India.Document6 pagesFAQs - What Is An Egg Donor - Egg Donor in Mumbai India.24x7emarketingPas encore d'évaluation
- IVF ART Laboratory Equipment - IVF Lab Design SetupDocument30 pagesIVF ART Laboratory Equipment - IVF Lab Design Setup24x7emarketing100% (3)
- IVF Treatment - IVF Treatments in Mumbai - IVF Doctors - IVF Clinics in Mumbai - Top IVF Hospital in MumbaiDocument4 pagesIVF Treatment - IVF Treatments in Mumbai - IVF Doctors - IVF Clinics in Mumbai - Top IVF Hospital in Mumbai24x7emarketingPas encore d'évaluation
- IVF Embryology WorkshopsDocument18 pagesIVF Embryology Workshops24x7emarketing100% (1)
- Canadian SurrogacyDocument4 pagesCanadian SurrogacyinstantdigitalprintPas encore d'évaluation
- Surrogacy India NewsDocument8 pagesSurrogacy India News24x7emarketingPas encore d'évaluation
- The New American FamilyDocument11 pagesThe New American Family24x7emarketingPas encore d'évaluation
- IVF TRAINING For EMBRYOLOGIST & GYNAECOLOGISTDocument3 pagesIVF TRAINING For EMBRYOLOGIST & GYNAECOLOGIST24x7emarketingPas encore d'évaluation
- IVF and Assisted HatchingDocument3 pagesIVF and Assisted Hatching24x7emarketingPas encore d'évaluation
- IVF Infertility Treatment IndiaDocument26 pagesIVF Infertility Treatment India24x7emarketing100% (1)
- Reproductive HealthDocument2 pagesReproductive Health24x7emarketingPas encore d'évaluation
- Law Commission On Surrogacy in India SurrogacyDocument10 pagesLaw Commission On Surrogacy in India Surrogacy24x7emarketing100% (1)
- Frequently Asked Questions About Fertility IVFDocument10 pagesFrequently Asked Questions About Fertility IVFinstantdigitalprintPas encore d'évaluation
- Blocked Fallopian Tubes - Treatment OptionsDocument4 pagesBlocked Fallopian Tubes - Treatment Options24x7emarketingPas encore d'évaluation
- Gay Dads Canada, Gay Dads USA, Gay Dads Australia, Gay Dads Ireland, Gay Dads France, Gay Dads UKDocument10 pagesGay Dads Canada, Gay Dads USA, Gay Dads Australia, Gay Dads Ireland, Gay Dads France, Gay Dads UK24x7emarketingPas encore d'évaluation
- Resources BollywoodDocument12 pagesResources Bollywood24x7emarketing67% (3)
- Top Indian ad agencies by billings and clientsDocument9 pagesTop Indian ad agencies by billings and clientsArun SachuPas encore d'évaluation
- Surrogacy Rotunda, Surrogacy Australia, Surrogacy Ireland, Surrogacy France, Surrogacy Uk, Surrogacy Usa, Surrogacy CanadaDocument6 pagesSurrogacy Rotunda, Surrogacy Australia, Surrogacy Ireland, Surrogacy France, Surrogacy Uk, Surrogacy Usa, Surrogacy Canada24x7emarketingPas encore d'évaluation
- World War II - European TheaterDocument8 pagesWorld War II - European TheaterElitePoa RsPas encore d'évaluation
- IVF Laboratory EquipmentDocument1 pageIVF Laboratory Equipment24x7emarketingPas encore d'évaluation
- Design and Set Up Ivf Lab FOR IVF CLINICDocument4 pagesDesign and Set Up Ivf Lab FOR IVF CLINIC24x7emarketing100% (2)
- The IVF Lab - The Heart of The IVF ClinicDocument1 pageThe IVF Lab - The Heart of The IVF Clinic24x7emarketingPas encore d'évaluation
- Workshop On IVF FertilityDocument2 pagesWorkshop On IVF Fertility24x7emarketingPas encore d'évaluation
- Obstetrics Fertility CME OB/GYN Conference Medical EducationDocument15 pagesObstetrics Fertility CME OB/GYN Conference Medical Education24x7emarketingPas encore d'évaluation
- Assisted Reproduction Technology Obstetrics Gynecology IVF IUi ART ICSI Fertility CME ConferenceDocument15 pagesAssisted Reproduction Technology Obstetrics Gynecology IVF IUi ART ICSI Fertility CME Conference24x7emarketingPas encore d'évaluation
- Obstetrics Fertility CME OB/GYN Conference Medical EducationDocument15 pagesObstetrics Fertility CME OB/GYN Conference Medical Education24x7emarketingPas encore d'évaluation
- Medical Conferences India: Gynaecologists Workshop / CME Gynaecology Obstetrics Infertility IVFDocument4 pagesMedical Conferences India: Gynaecologists Workshop / CME Gynaecology Obstetrics Infertility IVF24x7emarketingPas encore d'évaluation
- Obstetrics Fertility CME OB/GYN Conference Medical EducationDocument15 pagesObstetrics Fertility CME OB/GYN Conference Medical Education24x7emarketingPas encore d'évaluation
- Obstetrics Fertility CME OB/GYN Conference Medical EducationDocument15 pagesObstetrics Fertility CME OB/GYN Conference Medical Education24x7emarketingPas encore d'évaluation
- Shoe Dog: A Memoir by the Creator of NikeD'EverandShoe Dog: A Memoir by the Creator of NikeÉvaluation : 4.5 sur 5 étoiles4.5/5 (537)
- Never Split the Difference: Negotiating As If Your Life Depended On ItD'EverandNever Split the Difference: Negotiating As If Your Life Depended On ItÉvaluation : 4.5 sur 5 étoiles4.5/5 (838)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureD'EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureÉvaluation : 4.5 sur 5 étoiles4.5/5 (474)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeD'EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeÉvaluation : 4 sur 5 étoiles4/5 (5783)
- Grit: The Power of Passion and PerseveranceD'EverandGrit: The Power of Passion and PerseveranceÉvaluation : 4 sur 5 étoiles4/5 (587)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceD'EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceÉvaluation : 4 sur 5 étoiles4/5 (890)
- The Yellow House: A Memoir (2019 National Book Award Winner)D'EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Évaluation : 4 sur 5 étoiles4/5 (98)
- On Fire: The (Burning) Case for a Green New DealD'EverandOn Fire: The (Burning) Case for a Green New DealÉvaluation : 4 sur 5 étoiles4/5 (72)
- The Little Book of Hygge: Danish Secrets to Happy LivingD'EverandThe Little Book of Hygge: Danish Secrets to Happy LivingÉvaluation : 3.5 sur 5 étoiles3.5/5 (399)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryD'EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryÉvaluation : 3.5 sur 5 étoiles3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnD'EverandTeam of Rivals: The Political Genius of Abraham LincolnÉvaluation : 4.5 sur 5 étoiles4.5/5 (234)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaD'EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaÉvaluation : 4.5 sur 5 étoiles4.5/5 (265)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersD'EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersÉvaluation : 4.5 sur 5 étoiles4.5/5 (344)
- The Emperor of All Maladies: A Biography of CancerD'EverandThe Emperor of All Maladies: A Biography of CancerÉvaluation : 4.5 sur 5 étoiles4.5/5 (271)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyD'EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyÉvaluation : 3.5 sur 5 étoiles3.5/5 (2219)
- The Unwinding: An Inner History of the New AmericaD'EverandThe Unwinding: An Inner History of the New AmericaÉvaluation : 4 sur 5 étoiles4/5 (45)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreD'EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreÉvaluation : 4 sur 5 étoiles4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)D'EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Évaluation : 4.5 sur 5 étoiles4.5/5 (119)
- Her Body and Other Parties: StoriesD'EverandHer Body and Other Parties: StoriesÉvaluation : 4 sur 5 étoiles4/5 (821)
- Na Blog - CZ: ClozeDocument6 pagesNa Blog - CZ: ClozeUtari Septiana DewiPas encore d'évaluation
- NTA NEET Biology Syallabus 2021 2022Document6 pagesNTA NEET Biology Syallabus 2021 2022Shridansh TripathiPas encore d'évaluation
- Important Points GyeneDocument9 pagesImportant Points GyeneDr.G.Bhanu Prakash100% (3)
- Assessing Male Genitalia and InguinalDocument51 pagesAssessing Male Genitalia and InguinalJellaiza QuiozonPas encore d'évaluation
- Reproductive System Notes - 2014-15 DraftDocument62 pagesReproductive System Notes - 2014-15 DraftMiguel MenendezPas encore d'évaluation
- 3 Propagation Methods in PlantsDocument10 pages3 Propagation Methods in PlantsRaquel Husayan ParanPas encore d'évaluation
- Bio 1Document3 pagesBio 1James TolentinoPas encore d'évaluation
- Obstetrics and Gynaecology, 4th Edition - Impey, Lawrence, Child, TimDocument1 pageObstetrics and Gynaecology, 4th Edition - Impey, Lawrence, Child, TimalfredmansonPas encore d'évaluation
- Module 23Document18 pagesModule 23Jerico CastilloPas encore d'évaluation
- For Other Uses, See .: Seed (Disambiguation)Document65 pagesFor Other Uses, See .: Seed (Disambiguation)MADZPas encore d'évaluation
- Bangladesh School Muscat Yearly Syllabus ACADEMIC YEAR: 2020-2021 Class:XDocument19 pagesBangladesh School Muscat Yearly Syllabus ACADEMIC YEAR: 2020-2021 Class:XAbdul NoorPas encore d'évaluation
- DR - Shamim Rima MBBS, Dmu, FCGP M.Phil Radiology & ImagingDocument71 pagesDR - Shamim Rima MBBS, Dmu, FCGP M.Phil Radiology & Imagingdr_shamimrPas encore d'évaluation
- Penleigh and Essendon Grammar School YEAR 11 BIOLOGY, 2021 Semester 2 Exam 29 October, 2021Document25 pagesPenleigh and Essendon Grammar School YEAR 11 BIOLOGY, 2021 Semester 2 Exam 29 October, 2021testsubjectnumber500Pas encore d'évaluation
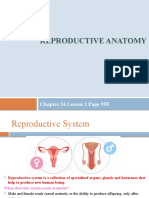
- Reproductive Anatomy: Chapter 34 Lesson 1 Page 958Document13 pagesReproductive Anatomy: Chapter 34 Lesson 1 Page 958JanaPas encore d'évaluation
- Reproduction in Algae 2Document7 pagesReproduction in Algae 2damanjeettiwana4Pas encore d'évaluation
- Instructional Planning on Puberty ChangesDocument12 pagesInstructional Planning on Puberty ChangesMerce Tojino ManigosPas encore d'évaluation
- SAQ EmbryologyDocument9 pagesSAQ EmbryologyShilpa DuttaPas encore d'évaluation
- Theories of EvolutionDocument5 pagesTheories of EvolutionMehar FathimaPas encore d'évaluation
- Organized KinematicsDocument56 pagesOrganized KinematicsBrad McFallPas encore d'évaluation
- Exercise A: Naming Plants and Using Keys Pre-Lab AssignmentDocument27 pagesExercise A: Naming Plants and Using Keys Pre-Lab AssignmentEssay NationPas encore d'évaluation
- Meiosis Pipe Cleaner LabDocument3 pagesMeiosis Pipe Cleaner Labmaeko nayuPas encore d'évaluation
- Cambridge Lower Secondary Checkpoint: Science 1113/02Document16 pagesCambridge Lower Secondary Checkpoint: Science 1113/02lol82% (17)
- Diagestive, Urinary and Reproductive SystemDocument39 pagesDiagestive, Urinary and Reproductive SystemCarolina Calle HerreraPas encore d'évaluation
- Perpetuation of LifeDocument1 pagePerpetuation of LifeDenise Antoneth Plangca100% (1)
- Lab Exercise19 Reproductive System PDFDocument3 pagesLab Exercise19 Reproductive System PDFcsolutionPas encore d'évaluation
- Text Test Bank 11Document11 pagesText Test Bank 11n1n2n3nPas encore d'évaluation
- Study of Life and Living OrganismsDocument5 pagesStudy of Life and Living OrganismsVidGe MasaquelPas encore d'évaluation
- Compare and Contrast Plant and Animal Reproduction and DevelopmentDocument145 pagesCompare and Contrast Plant and Animal Reproduction and DevelopmentAuxidyPas encore d'évaluation
- A Review: Brief Insight Into Polycystic Ovarian SyndromeDocument7 pagesA Review: Brief Insight Into Polycystic Ovarian SyndromeAnh Vũ Hồ NgọcPas encore d'évaluation
- Congenital Malformations of The Genital Tract andDocument19 pagesCongenital Malformations of The Genital Tract andabhinay_1712100% (1)