Vous aimerez peut-être aussi
- The Care Process: Assessment, planning, implementation and evaluation in healthcareD'EverandThe Care Process: Assessment, planning, implementation and evaluation in healthcarePas encore d'évaluation
- Collaborative Care Between Nurse Practitioners and Primary Care PhysiciansDocument11 pagesCollaborative Care Between Nurse Practitioners and Primary Care PhysiciansLeek AgoessPas encore d'évaluation
- Healthcare in Practice: Communicating Principles of Practice in Health and Social CareD'EverandHealthcare in Practice: Communicating Principles of Practice in Health and Social CarePas encore d'évaluation
- Quality of Care: Eze Chukwu NwoyeDocument22 pagesQuality of Care: Eze Chukwu Nwoyeeze NwoyePas encore d'évaluation
- Program Graduate Competency ReflectionDocument11 pagesProgram Graduate Competency Reflectionapi-458433381Pas encore d'évaluation
- Understanding Your Child's and Teen's Behavior: Simple Steps and Resources to Guide You Through the JourneyD'EverandUnderstanding Your Child's and Teen's Behavior: Simple Steps and Resources to Guide You Through the JourneyPas encore d'évaluation
- Health Promotion and Health Education - Nursing Students - Perspect PDFDocument120 pagesHealth Promotion and Health Education - Nursing Students - Perspect PDFAlex Olivar100% (1)
- Enabling Learning in Nursing and Midwifery Practice: A Guide for MentorsD'EverandEnabling Learning in Nursing and Midwifery Practice: A Guide for MentorsSue WestPas encore d'évaluation
- Multidisciplinary Team and Pharmacists Role in That TeamDocument5 pagesMultidisciplinary Team and Pharmacists Role in That TeamTimothy OgomaPas encore d'évaluation
- A Clinical Nurse Specialist-Led Interprofessional Quality Improvement Project To Reduce Hospital-Acquired Pressure Ulcers Clinical Nurse SpecialistDocument7 pagesA Clinical Nurse Specialist-Led Interprofessional Quality Improvement Project To Reduce Hospital-Acquired Pressure Ulcers Clinical Nurse SpecialistIhsan Nur MahmudiPas encore d'évaluation
- Roles and Responsibilities of A NurseDocument3 pagesRoles and Responsibilities of A NurseAubrey De Gracia0% (1)
- 2010 SWOT Harrison - Chapter5 Health Administration Press, 2010Document7 pages2010 SWOT Harrison - Chapter5 Health Administration Press, 2010Fernando NingunoPas encore d'évaluation
- BEFITBODY Wellness Menu of ServicesDocument46 pagesBEFITBODY Wellness Menu of ServicesPeri TharpPas encore d'évaluation
- 10 Qualities of A Great Nurse EducatorDocument53 pages10 Qualities of A Great Nurse EducatorAmy Roc100% (1)
- Professional Role Development Plan NewDocument8 pagesProfessional Role Development Plan Newapi-532226029Pas encore d'évaluation
- Op-Ed Part 2Document1 pageOp-Ed Part 2api-530416054Pas encore d'évaluation
- Nursing Dissertation, Nursing Essay, Nursing Project, Nursing Assignment, Nursing Homework, Nursing Writing, Nursing Outline, Nursing Abstract, Nursing DissertationDocument10 pagesNursing Dissertation, Nursing Essay, Nursing Project, Nursing Assignment, Nursing Homework, Nursing Writing, Nursing Outline, Nursing Abstract, Nursing DissertationiWanttutor.com100% (1)
- Medical Assistance in Dying NewDocument4 pagesMedical Assistance in Dying NewNarinder S.Pas encore d'évaluation
- Patient Centred CareDocument45 pagesPatient Centred CareAnjali Pant100% (1)
- Organizing Patient CareDocument16 pagesOrganizing Patient CareWalid Gee AbdulrahimPas encore d'évaluation
- Reflection PaperDocument9 pagesReflection Paperapi-302035669Pas encore d'évaluation
- A Syllabus For Fellowship Education in Palliative MedicineDocument12 pagesA Syllabus For Fellowship Education in Palliative Medicinebaixinha_Pas encore d'évaluation
- 1I02 Clinical Nursing Practice Notes Week 3 Reflection (3 Parts)Document39 pages1I02 Clinical Nursing Practice Notes Week 3 Reflection (3 Parts)NTRisforthinkersPas encore d'évaluation
- HLTH 300 Reflection - ReflectionDocument5 pagesHLTH 300 Reflection - Reflectionapi-479186899Pas encore d'évaluation
- The Constraints in Providing Primary Care To Elder Patients With Chronic Disease Causes A More Challenging Physical and Social EnvironmentDocument10 pagesThe Constraints in Providing Primary Care To Elder Patients With Chronic Disease Causes A More Challenging Physical and Social EnvironmentTony MuselaPas encore d'évaluation
- Hsci 360 Long Term Care PPT Revised 9Document23 pagesHsci 360 Long Term Care PPT Revised 9api-249502229Pas encore d'évaluation
- The DNP Project ToolboxDocument43 pagesThe DNP Project ToolboxGRooT tolOGYPas encore d'évaluation
- Psychological ChangesDocument36 pagesPsychological ChangesAndrei La MadridPas encore d'évaluation
- Panna Dhai Maa Subharti Nursing College: Amritanshu Chanchal M.SC Nursing 2 Year Bipolar DisorderDocument24 pagesPanna Dhai Maa Subharti Nursing College: Amritanshu Chanchal M.SC Nursing 2 Year Bipolar DisorderamritanshuPas encore d'évaluation
- AMA Guide To Alternative Payment Models PDFDocument26 pagesAMA Guide To Alternative Payment Models PDFiggybauPas encore d'évaluation
- Dementia Care. Part 2 Understanding and Managing Behavioural ChallengesDocument7 pagesDementia Care. Part 2 Understanding and Managing Behavioural Challengesdogstar23100% (2)
- Against All Odds Preventing Pressure Ulcers in High-Risk Cardiac Surgery PatientsDocument8 pagesAgainst All Odds Preventing Pressure Ulcers in High-Risk Cardiac Surgery PatientsjokoPas encore d'évaluation
- Inpatients Falls ProjectDocument10 pagesInpatients Falls ProjectAshraf Ali Smadi100% (3)
- Theory of Interpersonal RelationsDocument2 pagesTheory of Interpersonal RelationsAra Gayares Gallo100% (1)
- Dementia & Alzheimer's Care: Planning and Preparing For The Road AheadDocument14 pagesDementia & Alzheimer's Care: Planning and Preparing For The Road AheadblurrmiePas encore d'évaluation
- Care Planning ToolkitDocument47 pagesCare Planning ToolkitAjeet YadavPas encore d'évaluation
- Nursing Philosophy Apa PaperDocument7 pagesNursing Philosophy Apa Paperapi-449016836Pas encore d'évaluation
- Beyond Person Centred CareDocument11 pagesBeyond Person Centred CareJando Minggo SimonPas encore d'évaluation
- Child and Family Health Practice FrameworkDocument37 pagesChild and Family Health Practice Frameworkwildan yogaPas encore d'évaluation
- Care Coordination: - Case Management - Disease ManagementDocument27 pagesCare Coordination: - Case Management - Disease Managementamarneh1969Pas encore d'évaluation
- Diabetes Disease ManagementDocument7 pagesDiabetes Disease ManagementNashPas encore d'évaluation
- Nursing Philosophy QepDocument5 pagesNursing Philosophy Qepapi-534072530Pas encore d'évaluation
- Interdisciplinary Collaboration: Experience of Working in An Interdisciplinary Team in Healthcare at The MOI Teaching and Referral Hospital, Intensive Care UnitDocument3 pagesInterdisciplinary Collaboration: Experience of Working in An Interdisciplinary Team in Healthcare at The MOI Teaching and Referral Hospital, Intensive Care UnitInternational Journal of Innovative Science and Research TechnologyPas encore d'évaluation
- BSN Pgcs Reflection - KimDocument11 pagesBSN Pgcs Reflection - Kimapi-458308352Pas encore d'évaluation
- Hospital Discharge Education For CHFDocument18 pagesHospital Discharge Education For CHFarafathusein29Pas encore d'évaluation
- Competencies For Entry-Level Registered Nurse PracticeDocument16 pagesCompetencies For Entry-Level Registered Nurse PracticeAnooj FrancisPas encore d'évaluation
- INTRODUCTION TO GLOBAL HEALTH LessonsDocument39 pagesINTRODUCTION TO GLOBAL HEALTH LessonsDeidra Borus100% (1)
- What Is Person-Centred Care and Why Is It Important PDFDocument7 pagesWhat Is Person-Centred Care and Why Is It Important PDFZita VeszelakPas encore d'évaluation
- CCM DiabetesDocument21 pagesCCM DiabetesRobertPas encore d'évaluation
- Capstone Research PaperDocument22 pagesCapstone Research Paperapi-251333389Pas encore d'évaluation
- Wellness Program White PaperDocument16 pagesWellness Program White PaperJae SolPas encore d'évaluation
- Improving The Care of Older Adults Full ReportDocument74 pagesImproving The Care of Older Adults Full ReportKhoirun NisyakPas encore d'évaluation
- Liverpool Care Pathway PDFDocument63 pagesLiverpool Care Pathway PDFBryan DorosanPas encore d'évaluation
- Stigma and Discrimination-HIV and Aids Context: (A Case Study of University CommunityDocument9 pagesStigma and Discrimination-HIV and Aids Context: (A Case Study of University CommunityJASH MATHEWPas encore d'évaluation
- Population Health Core Concept PaperDocument12 pagesPopulation Health Core Concept Paperapi-312747585Pas encore d'évaluation
- Sample Nursing Interview Questions & TipsDocument2 pagesSample Nursing Interview Questions & TipssamdakaPas encore d'évaluation
- Intensive Care Unit - Docx 1Document12 pagesIntensive Care Unit - Docx 1Vaibhav MongaPas encore d'évaluation
- PROFESSIONALISM in The Community Health NurseDocument35 pagesPROFESSIONALISM in The Community Health NurseKristin Jones100% (1)
- Centr RecipesDocument20 pagesCentr RecipesAndrew WongPas encore d'évaluation
- Hand Injuries Guidelines 2020Document64 pagesHand Injuries Guidelines 2020Andrew WongPas encore d'évaluation
- Chapter 3 - Lower Extremity - 2020 - MLDocument71 pagesChapter 3 - Lower Extremity - 2020 - MLAndrew WongPas encore d'évaluation
- Cardiac Soc BWHDocument36 pagesCardiac Soc BWHAndrew WongPas encore d'évaluation
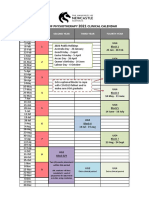
- UON Physiotherapy Calendar 2021 PDFDocument1 pageUON Physiotherapy Calendar 2021 PDFAndrew WongPas encore d'évaluation
- How To Develop A Program LogicDocument3 pagesHow To Develop A Program LogicAndrew WongPas encore d'évaluation
- Christmas SongsDocument24 pagesChristmas SongsAndrew WongPas encore d'évaluation
- NSLHD Policy Procedure Guideline Communique 14 Oct 2019Document3 pagesNSLHD Policy Procedure Guideline Communique 14 Oct 2019Andrew WongPas encore d'évaluation
- Module 1 SEM-C4DDocument19 pagesModule 1 SEM-C4DAndrew WongPas encore d'évaluation
- Program LogicDocument1 pageProgram LogicAndrew WongPas encore d'évaluation
- Overarching Logic Model: Reducing and Preventing Youth Tobacco UseDocument5 pagesOverarching Logic Model: Reducing and Preventing Youth Tobacco UseAndrew WongPas encore d'évaluation
- 3 Full Body Workouts For Cutting Body Fat!Document15 pages3 Full Body Workouts For Cutting Body Fat!Andrew WongPas encore d'évaluation
- Anselm L. Strauss, Shizuko Fagerhaugh, Barbara Suczek, Carolyn Wiener - Social Organization of Medical Work (1985, University of Chicago Press) PDFDocument323 pagesAnselm L. Strauss, Shizuko Fagerhaugh, Barbara Suczek, Carolyn Wiener - Social Organization of Medical Work (1985, University of Chicago Press) PDFDiogo Silva Correa100% (1)
- Chronic ModelDocument18 pagesChronic ModelDaisy SinduPas encore d'évaluation
- Sejarah Dan Definisi Psikologi PositifDocument11 pagesSejarah Dan Definisi Psikologi PositifHaryadi KurniawanPas encore d'évaluation
- Chronic Care Model GuideDocument2 pagesChronic Care Model GuideARHeiderPas encore d'évaluation
- Issues and Trends in Chronic CareDocument10 pagesIssues and Trends in Chronic CareElaine Dionisio TanPas encore d'évaluation
- Care For People With Chronic Conditions Guide For Community Health ProgramDocument42 pagesCare For People With Chronic Conditions Guide For Community Health ProgramAndrew Wong100% (1)
- Challenging Clinical Inertia and The Stepwise Diabetes Treatment Approach (With Insulin Therapy)Document33 pagesChallenging Clinical Inertia and The Stepwise Diabetes Treatment Approach (With Insulin Therapy)Eva GabrielPas encore d'évaluation
- Self ManagementDocument218 pagesSelf ManagementRiza Muhammad Nuur100% (1)
- Telehealth: Review and Perspectives For SingaporeDocument33 pagesTelehealth: Review and Perspectives For Singaporesuhangmydoc100% (1)
- Core Jail StandardsDocument57 pagesCore Jail StandardsDavid Epson MayerPas encore d'évaluation
- Chapter 21 Intrapartum Nursing AssessmentDocument27 pagesChapter 21 Intrapartum Nursing AssessmentNurse Utopia100% (1)
- ProposalDocument2 pagesProposalapi-252954099Pas encore d'évaluation
- Evaluation of Chronic Patient Nursing Care by The Patients - A University Hospital CaseDocument13 pagesEvaluation of Chronic Patient Nursing Care by The Patients - A University Hospital CaseGlobal Research and Development ServicesPas encore d'évaluation
- ChronicCareManagementDocument23 pagesChronicCareManagementRizki Yuliana100% (1)
- NURS FPX 6618 Assessment 1 Planning and Presenting A Care Coordination ProjectDocument5 pagesNURS FPX 6618 Assessment 1 Planning and Presenting A Care Coordination Projectjoohnsmith070Pas encore d'évaluation
- Applying The Chronic Care Model in Low-Resource Settings Ada Dec2013Document44 pagesApplying The Chronic Care Model in Low-Resource Settings Ada Dec2013Wawan JokoPas encore d'évaluation
- Reiss Sandborn 2015 Role of Psychosocial CareDocument6 pagesReiss Sandborn 2015 Role of Psychosocial CareAgata AgniPas encore d'évaluation
- Stephanie's CVDocument3 pagesStephanie's CVmadcat1425Pas encore d'évaluation
- NURS FPX 6618 Assessment 1 Planning and Presenting A Care Coordination ProjectDocument5 pagesNURS FPX 6618 Assessment 1 Planning and Presenting A Care Coordination ProjectEmma WatsonPas encore d'évaluation
- Do You Believe in Magic?: The Sense and Nonsense of Alternative MedicineD'EverandDo You Believe in Magic?: The Sense and Nonsense of Alternative MedicinePas encore d'évaluation
- Scaling Up: How a Few Companies Make It...and Why the Rest Don't, Rockefeller Habits 2.0D'EverandScaling Up: How a Few Companies Make It...and Why the Rest Don't, Rockefeller Habits 2.0Évaluation : 5 sur 5 étoiles5/5 (2)
- Uncontrolled Spread: Why COVID-19 Crushed Us and How We Can Defeat the Next PandemicD'EverandUncontrolled Spread: Why COVID-19 Crushed Us and How We Can Defeat the Next PandemicPas encore d'évaluation
- Summary: The Myth of Normal: Trauma, Illness, and Healing in a Toxic Culture By Gabor Maté MD & Daniel Maté: Key Takeaways, Summary & AnalysisD'EverandSummary: The Myth of Normal: Trauma, Illness, and Healing in a Toxic Culture By Gabor Maté MD & Daniel Maté: Key Takeaways, Summary & AnalysisÉvaluation : 4 sur 5 étoiles4/5 (9)
- The Power of People Skills: How to Eliminate 90% of Your HR Problems and Dramatically Increase Team and Company Morale and PerformanceD'EverandThe Power of People Skills: How to Eliminate 90% of Your HR Problems and Dramatically Increase Team and Company Morale and PerformanceÉvaluation : 5 sur 5 étoiles5/5 (22)
- Powerful Phrases for Dealing with Difficult People: Over 325 Ready-to-Use Words and Phrases for Working with Challenging PersonalitiesD'EverandPowerful Phrases for Dealing with Difficult People: Over 325 Ready-to-Use Words and Phrases for Working with Challenging PersonalitiesÉvaluation : 4 sur 5 étoiles4/5 (14)
- The Five Dysfunctions of a Team SummaryD'EverandThe Five Dysfunctions of a Team SummaryÉvaluation : 4.5 sur 5 étoiles4.5/5 (59)
- Getting Along: How to Work with Anyone (Even Difficult People)D'EverandGetting Along: How to Work with Anyone (Even Difficult People)Évaluation : 4.5 sur 5 étoiles4.5/5 (18)
- Summary: Who Moved My Cheese?: An A-Mazing Way to Deal with Change in Your Work and in Your Life by Spencer Johnson M.D. and Kenneth Blanchard: Key Takeaways, Summary & AnalysisD'EverandSummary: Who Moved My Cheese?: An A-Mazing Way to Deal with Change in Your Work and in Your Life by Spencer Johnson M.D. and Kenneth Blanchard: Key Takeaways, Summary & AnalysisÉvaluation : 3.5 sur 5 étoiles3.5/5 (3)
- Deaths of Despair and the Future of CapitalismD'EverandDeaths of Despair and the Future of CapitalismÉvaluation : 4.5 sur 5 étoiles4.5/5 (30)
- 50 Top Tools for Coaching, 3rd Edition: A Complete Toolkit for Developing and Empowering PeopleD'Everand50 Top Tools for Coaching, 3rd Edition: A Complete Toolkit for Developing and Empowering PeopleÉvaluation : 4.5 sur 5 étoiles4.5/5 (4)
- Finding the Next Steve Jobs: How to Find, Keep, and Nurture TalentD'EverandFinding the Next Steve Jobs: How to Find, Keep, and Nurture TalentÉvaluation : 4.5 sur 5 étoiles4.5/5 (18)
- Working with AI: Real Stories of Human-Machine Collaboration (Management on the Cutting Edge)D'EverandWorking with AI: Real Stories of Human-Machine Collaboration (Management on the Cutting Edge)Évaluation : 5 sur 5 étoiles5/5 (5)
- 12 Habits Of Valuable Employees: Your Roadmap to an Amazing CareerD'Everand12 Habits Of Valuable Employees: Your Roadmap to an Amazing CareerPas encore d'évaluation
- The Manager's Path: A Guide for Tech Leaders Navigating Growth and ChangeD'EverandThe Manager's Path: A Guide for Tech Leaders Navigating Growth and ChangeÉvaluation : 4.5 sur 5 étoiles4.5/5 (99)
- The 5 Languages of Appreciation in the Workplace: Empowering Organizations by Encouraging PeopleD'EverandThe 5 Languages of Appreciation in the Workplace: Empowering Organizations by Encouraging PeopleÉvaluation : 4.5 sur 5 étoiles4.5/5 (47)
- Developing Coaching Skills: A Concise IntroductionD'EverandDeveloping Coaching Skills: A Concise IntroductionÉvaluation : 4.5 sur 5 étoiles4.5/5 (5)
- Zconomy: How Gen Z Will Change the Future of Business—and What to Do About ItD'EverandZconomy: How Gen Z Will Change the Future of Business—and What to Do About ItPas encore d'évaluation
- Hire With Your Head: Using Performance-Based Hiring to Build Outstanding Diverse TeamsD'EverandHire With Your Head: Using Performance-Based Hiring to Build Outstanding Diverse TeamsÉvaluation : 4.5 sur 5 étoiles4.5/5 (5)
- The Wisdom of Plagues: Lessons from 25 Years of Covering PandemicsD'EverandThe Wisdom of Plagues: Lessons from 25 Years of Covering PandemicsÉvaluation : 4.5 sur 5 étoiles4.5/5 (6)
- How Performance Management Is Killing Performance—and What to Do About It: Rethink, Redesign, RebootD'EverandHow Performance Management Is Killing Performance—and What to Do About It: Rethink, Redesign, RebootPas encore d'évaluation
- The Fearless Organization: Creating Psychological Safety in the Workplace for Learning, Innovation, and GrowthD'EverandThe Fearless Organization: Creating Psychological Safety in the Workplace for Learning, Innovation, and GrowthÉvaluation : 4.5 sur 5 étoiles4.5/5 (101)
- HBR at 100: The Most Influential and Innovative Articles from Harvard Business Review's First CenturyD'EverandHBR at 100: The Most Influential and Innovative Articles from Harvard Business Review's First CenturyÉvaluation : 3.5 sur 5 étoiles3.5/5 (6)
- The Good Jobs Strategy: How the Smartest Companies Invest in Employees to Lower Costs and Boost ProfitsD'EverandThe Good Jobs Strategy: How the Smartest Companies Invest in Employees to Lower Costs and Boost ProfitsÉvaluation : 4.5 sur 5 étoiles4.5/5 (16)
- Scaling Up Compensation: 5 Design Principles for Turning Your Largest Expense into a Strategic AdvantageD'EverandScaling Up Compensation: 5 Design Principles for Turning Your Largest Expense into a Strategic AdvantageÉvaluation : 5 sur 5 étoiles5/5 (4)