Vous aimerez peut-être aussi
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryD'EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryÉvaluation : 3.5 sur 5 étoiles3.5/5 (231)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)D'EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Évaluation : 4.5 sur 5 étoiles4.5/5 (119)
- Never Split the Difference: Negotiating As If Your Life Depended On ItD'EverandNever Split the Difference: Negotiating As If Your Life Depended On ItÉvaluation : 4.5 sur 5 étoiles4.5/5 (838)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaD'EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaÉvaluation : 4.5 sur 5 étoiles4.5/5 (265)
- The Little Book of Hygge: Danish Secrets to Happy LivingD'EverandThe Little Book of Hygge: Danish Secrets to Happy LivingÉvaluation : 3.5 sur 5 étoiles3.5/5 (399)
- Grit: The Power of Passion and PerseveranceD'EverandGrit: The Power of Passion and PerseveranceÉvaluation : 4 sur 5 étoiles4/5 (587)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyD'EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyÉvaluation : 3.5 sur 5 étoiles3.5/5 (2219)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeD'EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeÉvaluation : 4 sur 5 étoiles4/5 (5794)
- Team of Rivals: The Political Genius of Abraham LincolnD'EverandTeam of Rivals: The Political Genius of Abraham LincolnÉvaluation : 4.5 sur 5 étoiles4.5/5 (234)
- Shoe Dog: A Memoir by the Creator of NikeD'EverandShoe Dog: A Memoir by the Creator of NikeÉvaluation : 4.5 sur 5 étoiles4.5/5 (537)
- The Emperor of All Maladies: A Biography of CancerD'EverandThe Emperor of All Maladies: A Biography of CancerÉvaluation : 4.5 sur 5 étoiles4.5/5 (271)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreD'EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreÉvaluation : 4 sur 5 étoiles4/5 (1090)
- Her Body and Other Parties: StoriesD'EverandHer Body and Other Parties: StoriesÉvaluation : 4 sur 5 étoiles4/5 (821)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersD'EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersÉvaluation : 4.5 sur 5 étoiles4.5/5 (344)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceD'EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceÉvaluation : 4 sur 5 étoiles4/5 (890)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureD'EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureÉvaluation : 4.5 sur 5 étoiles4.5/5 (474)
- The Unwinding: An Inner History of the New AmericaD'EverandThe Unwinding: An Inner History of the New AmericaÉvaluation : 4 sur 5 étoiles4/5 (45)
- The Yellow House: A Memoir (2019 National Book Award Winner)D'EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Évaluation : 4 sur 5 étoiles4/5 (98)
- On Fire: The (Burning) Case for a Green New DealD'EverandOn Fire: The (Burning) Case for a Green New DealÉvaluation : 4 sur 5 étoiles4/5 (73)
- APPLIED MECHANICAL ENGINEERING PROBLEM SOLVINGDocument4 pagesAPPLIED MECHANICAL ENGINEERING PROBLEM SOLVINGKyle LovePas encore d'évaluation
- Biology WS AnswersDocument17 pagesBiology WS AnswersKazePas encore d'évaluation
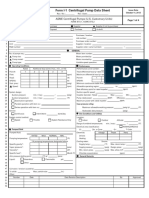
- Form I-1 Centrifugal Pump Data SheetDocument4 pagesForm I-1 Centrifugal Pump Data SheetJohnPas encore d'évaluation
- Blast Furnace Heat and Material Balance Using MS-Excel-Solver WBDocument42 pagesBlast Furnace Heat and Material Balance Using MS-Excel-Solver WBbabuxavier10Pas encore d'évaluation
- Ajit Vadakayil - BEEJ MANTRA - FrequencyDocument94 pagesAjit Vadakayil - BEEJ MANTRA - Frequencyjk.dasguptaPas encore d'évaluation
- Artículo Toxic JuiceDocument6 pagesArtículo Toxic JuiceSonia Fernández PradosPas encore d'évaluation
- Price 1998Document11 pagesPrice 1998LỢI NGUYỄN CÔNGPas encore d'évaluation
- Specialized lubricants maximize steel industry productivityDocument16 pagesSpecialized lubricants maximize steel industry productivitySioney MonteiroPas encore d'évaluation
- Resins Word DocumentDocument8 pagesResins Word DocumentHarish KakraniPas encore d'évaluation
- Sheet 1Document10 pagesSheet 1lawanPas encore d'évaluation
- Chemistry Notes For Class 12 Chapter 2 Solutions PDFDocument15 pagesChemistry Notes For Class 12 Chapter 2 Solutions PDFUmesh S Rathore100% (2)
- Current Events: Internet 1: An Optical Switch Based On A Single Nano-DiamondDocument3 pagesCurrent Events: Internet 1: An Optical Switch Based On A Single Nano-Diamondjennylee00182Pas encore d'évaluation
- Pen Type Visual Fault Locator: SpecificationsDocument1 pagePen Type Visual Fault Locator: SpecificationsHuy DuPas encore d'évaluation
- Banana Stem JuiceDocument8 pagesBanana Stem Juiceईन्द्रनील रायPas encore d'évaluation
- 9Document10 pages9Laurentiu Chilibaru-Cristina OpritescuPas encore d'évaluation
- What Are HerbicidesDocument14 pagesWhat Are HerbicidesBabatunde Alim OluwafẹmiPas encore d'évaluation
- Unit 7 MCQDocument5 pagesUnit 7 MCQWilliam XiePas encore d'évaluation
- 计量泵metering pump PDFDocument43 pages计量泵metering pump PDFAnonymous Tj3ApePIrPas encore d'évaluation
- What Is The Major Function of The Coating On An Arc Welding ElectrodeDocument7 pagesWhat Is The Major Function of The Coating On An Arc Welding ElectrodeElham Jaraine Garcia Lpt100% (4)
- Chemistry Assessment - Task 2 Report (Update 3)Document15 pagesChemistry Assessment - Task 2 Report (Update 3)kaylasadgrove4Pas encore d'évaluation
- A Finite Element Method Based Analysis of Casting Solidification Onpermanent Metallic ModelsDocument10 pagesA Finite Element Method Based Analysis of Casting Solidification Onpermanent Metallic ModelsseenisitPas encore d'évaluation
- Dwnload Full Visual Anatomy and Physiology 2nd Edition Martini Solutions Manual PDFDocument36 pagesDwnload Full Visual Anatomy and Physiology 2nd Edition Martini Solutions Manual PDFalluviumopuntialjvoh100% (9)
- Haldia Institute of Technology Engineering Chemistry Laboratory (CH 191 &CH 291)Document29 pagesHaldia Institute of Technology Engineering Chemistry Laboratory (CH 191 &CH 291)Shresth Sanskar100% (1)
- General Chemistry 1 Activity Sheet Quarter 2-MELC 12 Week 6Document9 pagesGeneral Chemistry 1 Activity Sheet Quarter 2-MELC 12 Week 6Joshua De La VegaPas encore d'évaluation
- Article1379594984 - Sivakumar and GomathiDocument7 pagesArticle1379594984 - Sivakumar and GomathiEdda GeregetanPas encore d'évaluation
- ABRASIVE JET MACHINING ModellingDocument3 pagesABRASIVE JET MACHINING ModellingAnkit OlaPas encore d'évaluation
- Silicone Materials Guide SnapDocument4 pagesSilicone Materials Guide SnapParagPas encore d'évaluation
- Aluminum Conditioner DX 503Document7 pagesAluminum Conditioner DX 503Mark Evan SalutinPas encore d'évaluation
- Experiment 1 and 2Document11 pagesExperiment 1 and 2Rohan MohantyPas encore d'évaluation
- TDS Energrease MP-MG 2 InfoDocument9 pagesTDS Energrease MP-MG 2 InfoLucian IftemiePas encore d'évaluation