Vous aimerez peut-être aussi
- PromDocument33 pagesPromkisPas encore d'évaluation
- Drug StudyyDocument3 pagesDrug StudyyShewit AbrahamPas encore d'évaluation
- Small Bowel Obstruction System - DisorderDocument1 pageSmall Bowel Obstruction System - DisorderMarina Wasem Netzlaff0% (1)
- College of Nursing: Cebu Normal UniversityDocument4 pagesCollege of Nursing: Cebu Normal UniversityFaye Andrea FranciscoPas encore d'évaluation
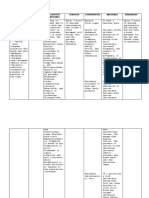
- Nursing Care Plan Drug Study: Assessment Nursing Diagnosis Nursing Goal Nursing Intervention Rationale EvaluationDocument2 pagesNursing Care Plan Drug Study: Assessment Nursing Diagnosis Nursing Goal Nursing Intervention Rationale Evaluationteejay andradaPas encore d'évaluation
- Khoory 2Document2 pagesKhoory 2Salamah KhooryPas encore d'évaluation
- NCM 112 MSN Prelim Topic 2 GastritisDocument1 pageNCM 112 MSN Prelim Topic 2 GastritisKim Erida QuezonPas encore d'évaluation
- MALABSORPTIONDocument3 pagesMALABSORPTIONZyra LagatPas encore d'évaluation
- NURSING CARE PLAN FOR DIARRHEADocument2 pagesNURSING CARE PLAN FOR DIARRHEAKrizha Angela NicolasPas encore d'évaluation
- Drug Study Nursing ResponsibilitiesDocument6 pagesDrug Study Nursing Responsibilitiesronnie023Pas encore d'évaluation
- NCP Nausea and VomitingDocument4 pagesNCP Nausea and VomitingKingJayson Pacman06Pas encore d'évaluation
- Gastroesophageal Reflux DiseaseDocument8 pagesGastroesophageal Reflux DiseaseEunice Ericka FloresPas encore d'évaluation
- DiareDocument5 pagesDiarefarisPas encore d'évaluation
- Pancreatitis Group 3 NCM 116Document21 pagesPancreatitis Group 3 NCM 116Diana Jane LauretaPas encore d'évaluation
- Breast Cancer Treatment PlanDocument2 pagesBreast Cancer Treatment PlanGilianne JimeneaPas encore d'évaluation
- Irritable Bowel Syndrome: Causes, Symptoms and ManagementDocument6 pagesIrritable Bowel Syndrome: Causes, Symptoms and ManagementmynamePas encore d'évaluation
- Nursing care plan for client experiencing nausea and vomitingDocument2 pagesNursing care plan for client experiencing nausea and vomitingHello KittyPas encore d'évaluation
- Acute PancreatitisDocument2 pagesAcute PancreatitisPrincess Aliha M. JIMENEZPas encore d'évaluation
- Hook Worm Infection: Republic of The Philippines City of Ilagan CampusDocument10 pagesHook Worm Infection: Republic of The Philippines City of Ilagan CampusCassey CuregPas encore d'évaluation
- Nursing Care Plan Diarrhea Assessment Diagnosis Planning Interventions Rationale EvaluationDocument8 pagesNursing Care Plan Diarrhea Assessment Diagnosis Planning Interventions Rationale EvaluationKrah100% (1)
- أروى حكميDocument16 pagesأروى حكميArwa HakamiPas encore d'évaluation
- DiarrheaDocument3 pagesDiarrheaBert GasalPas encore d'évaluation
- Case Study: Subjective: Objective: General Objective: Independent IndependentDocument10 pagesCase Study: Subjective: Objective: General Objective: Independent IndependentChristine EmanPas encore d'évaluation
- F. NCP PROPER CUES EXPLANATION GOALS INTERVENTIONS RATIONALE EVALUATIONDocument4 pagesF. NCP PROPER CUES EXPLANATION GOALS INTERVENTIONS RATIONALE EVALUATIONAle SandraPas encore d'évaluation
- HTP Uti (Artillo)Document2 pagesHTP Uti (Artillo)Al TheóPas encore d'évaluation
- 1 PPT Liver CirrhosisDocument65 pages1 PPT Liver CirrhosisDannaMae CastroPas encore d'évaluation
- Assessment Nursing Diagnosis Goals and Objective Nursing Interventions Rationale Evaluation SubjectiveDocument4 pagesAssessment Nursing Diagnosis Goals and Objective Nursing Interventions Rationale Evaluation SubjectiveDanica Kate GalleonPas encore d'évaluation
- Javier, Jomar A. BSN121 Group 83 Nursing Care Plan (Pediatric Patient)Document7 pagesJavier, Jomar A. BSN121 Group 83 Nursing Care Plan (Pediatric Patient)Julie AnnPas encore d'évaluation
- General Indications: BeforeDocument24 pagesGeneral Indications: Beforelouie john abilaPas encore d'évaluation
- LocalDocument5 pagesLocalybqbjpvtmrPas encore d'évaluation
- Abnormalities of Fecal Elimination SgmacDocument4 pagesAbnormalities of Fecal Elimination SgmacRachelle DelantarPas encore d'évaluation
- Nursing Care Plan for Diarrhea and Oral MucositisDocument7 pagesNursing Care Plan for Diarrhea and Oral MucositisJoshua MendozaPas encore d'évaluation
- DGJKHVDocument7 pagesDGJKHVGILIANNE MARIE JIMENEAPas encore d'évaluation
- MEDICATIONSDocument3 pagesMEDICATIONSchristyPas encore d'évaluation
- NCP FinalDocument18 pagesNCP FinalHelen GonzalesPas encore d'évaluation
- Case StudyDocument37 pagesCase StudyHecy CristoPas encore d'évaluation
- Managing Diverticulitis with Diet and RestDocument2 pagesManaging Diverticulitis with Diet and RestAhmad RizkiPas encore d'évaluation
- Diarrhea NCP Pedia WardDocument4 pagesDiarrhea NCP Pedia WardKyle DapulagPas encore d'évaluation
- Nursing Care Plan for Risk of Deficient Fluid VolumeDocument5 pagesNursing Care Plan for Risk of Deficient Fluid VolumeAmbrosio, Jasmin G.Pas encore d'évaluation
- Gonzaga Rlems - NCPDocument3 pagesGonzaga Rlems - NCPShaynne Wencille A. GONZAGAPas encore d'évaluation
- Resource Unit On Drugs and IVF's: College of NursingDocument7 pagesResource Unit On Drugs and IVF's: College of NursingJ Michael EscaraPas encore d'évaluation
- Assessment and Diagnostic ExamsDocument10 pagesAssessment and Diagnostic ExamsJan Mark SotoPas encore d'évaluation
- Cholecystitis Concept MapDocument4 pagesCholecystitis Concept Mapnursing concept maps100% (7)
- Drug Study: College of NursingDocument3 pagesDrug Study: College of NursingA.Pas encore d'évaluation
- Subjective: Nephrolithiasis Is STO: After 8 Diagnostics: STO: Fully MetDocument3 pagesSubjective: Nephrolithiasis Is STO: After 8 Diagnostics: STO: Fully MetSebastianPas encore d'évaluation
- Drug Study: College of NursingDocument3 pagesDrug Study: College of NursingA.Pas encore d'évaluation
- Nursing Care Plan for a Client with Intestinal ObstructionDocument4 pagesNursing Care Plan for a Client with Intestinal ObstructionRenea Joy ArruejoPas encore d'évaluation
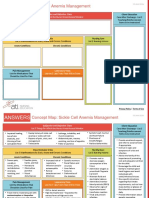
- NCC-SickleCellAnemiaManagement ConceptMap InteractivePDFDocument2 pagesNCC-SickleCellAnemiaManagement ConceptMap InteractivePDFLoggerz Arck100% (1)
- Diabetes Insipidus Nursing Care and TreatmentDocument2 pagesDiabetes Insipidus Nursing Care and TreatmentCharisse TaylanPas encore d'évaluation
- Planning Intervention Rationale Evaluation: Nursing Care Plan Problem DiagnosisDocument2 pagesPlanning Intervention Rationale Evaluation: Nursing Care Plan Problem DiagnosisRicardo Dela CruzPas encore d'évaluation
- B - Forcadilla, KiaraDocument10 pagesB - Forcadilla, KiaraKeir Mrls ForcadillaPas encore d'évaluation
- Nursing Care Plan: Diarrhea R/T Infectious Scientific: Goal: IndependentDocument4 pagesNursing Care Plan: Diarrhea R/T Infectious Scientific: Goal: IndependentKingJayson Pacman06Pas encore d'évaluation
- Diarrhea NCPDocument3 pagesDiarrhea NCPCharles Michael Azagra0% (1)
- Diarrhea NCPDocument3 pagesDiarrhea NCPCharles Michael AzagraPas encore d'évaluation
- Constipation: Patient Name: Shehzad Age: 45 Ward: Emergency BDocument2 pagesConstipation: Patient Name: Shehzad Age: 45 Ward: Emergency BShafiq Ur RahmanPas encore d'évaluation
- Case Scenario 3.editedDocument7 pagesCase Scenario 3.editedPoetic YatchyPas encore d'évaluation
- Rle Worksheet Nursing ProcessDocument6 pagesRle Worksheet Nursing ProcessMARVIE JOY BALUMA CABIOCPas encore d'évaluation
- Group 6 DiarheaDocument13 pagesGroup 6 DiarheaAkun NyampahPas encore d'évaluation
- Intestinal Failure: Diagnosis, Management and TransplantationD'EverandIntestinal Failure: Diagnosis, Management and TransplantationAlan LangnasPas encore d'évaluation
- Dictionary of Veterinary Terms: Vet-Speak Deciphered for the Non VeterinarianD'EverandDictionary of Veterinary Terms: Vet-Speak Deciphered for the Non VeterinarianPas encore d'évaluation
- Antibodies COVID 19Document6 pagesAntibodies COVID 19Ernesto SamamePas encore d'évaluation
- Test Bank For Roachs Introductory Clinical Pharmacology 10th North American Edition Susan M FordDocument9 pagesTest Bank For Roachs Introductory Clinical Pharmacology 10th North American Edition Susan M FordAnthonyRogersydtfp100% (61)
- USMLE Step 1 First Aid 2021-148-184Document37 pagesUSMLE Step 1 First Aid 2021-148-184mariana yllanesPas encore d'évaluation
- Acute Limb Ischemia SiteDocument23 pagesAcute Limb Ischemia Sitebenypermadi100% (1)
- Congenital Ichthyosis - Collodion Baby Case Report: KeywordsDocument2 pagesCongenital Ichthyosis - Collodion Baby Case Report: KeywordsLidia MdPas encore d'évaluation
- Neuromotor and Cognitive Functions in 4Document60 pagesNeuromotor and Cognitive Functions in 4ARICEL SALDIVIAPas encore d'évaluation
- MCQ Congenital Intestinal ObstructionDocument6 pagesMCQ Congenital Intestinal ObstructionAmrut LovesmusicPas encore d'évaluation
- Theories and Level of Disease Occurence FinalDocument108 pagesTheories and Level of Disease Occurence FinalruthPas encore d'évaluation
- Division Order/ Memorandum/Advisory: Division of City of San FernandoDocument9 pagesDivision Order/ Memorandum/Advisory: Division of City of San FernandogiansulakisosuPas encore d'évaluation
- Challenges in Health Care of Rural AreaDocument2 pagesChallenges in Health Care of Rural AreaKaran TrivediPas encore d'évaluation
- Veterinary EctoparasitesDocument8 pagesVeterinary Ectoparasitesc3891446100% (1)
- Surgery Question From AbeideDocument44 pagesSurgery Question From Abeide69xXALModr3EMXx69 McAnusPas encore d'évaluation
- Fungal Infections Explained: Types, Causes, Symptoms & TreatmentsDocument19 pagesFungal Infections Explained: Types, Causes, Symptoms & TreatmentsKasuganti koteshwar raoPas encore d'évaluation
- Managing Cramps During DialysisDocument7 pagesManaging Cramps During DialysisSavita HanamsagarPas encore d'évaluation
- Community Health Nursing: Arby James Abonalla, RN, MSN, PHDN (C)Document237 pagesCommunity Health Nursing: Arby James Abonalla, RN, MSN, PHDN (C)Roshie Kaye AbalorioPas encore d'évaluation
- Katzung LaxativesDocument6 pagesKatzung LaxativesLonnieAllenVirtudesPas encore d'évaluation
- What Are Koch's Postulates?Document3 pagesWhat Are Koch's Postulates?Cacamo Rexell-anPas encore d'évaluation
- Moh Exam Questions of Dr. EbiDocument11 pagesMoh Exam Questions of Dr. EbiHady SpinPas encore d'évaluation
- A39 Massage Chair Operation InstructionsDocument10 pagesA39 Massage Chair Operation InstructionsHelena MartinovićPas encore d'évaluation
- Doctors of Adventure-WorksheetDocument1 pageDoctors of Adventure-WorksheetJesus LizcanoPas encore d'évaluation
- 28 11 2019 8th Aitong Medical Camp ReportDocument26 pages28 11 2019 8th Aitong Medical Camp ReportStacy NeetPas encore d'évaluation
- 11.1 Diploma - in - Fitness - Complete - Master - Manual - FDocument67 pages11.1 Diploma - in - Fitness - Complete - Master - Manual - FAnil TalariPas encore d'évaluation
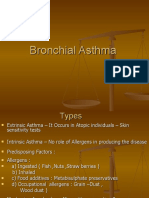
- Bronchial AsthmaDocument16 pagesBronchial AsthmaSHAIK SHABEENA100% (1)
- New Approaches To An Old Disease: GoutDocument27 pagesNew Approaches To An Old Disease: GoutDini HanifaPas encore d'évaluation
- OTC Drugs SeminarDocument42 pagesOTC Drugs SeminarSheena GagarinPas encore d'évaluation
- Dialysis MachineDocument1 pageDialysis MachineMarifer NazPas encore d'évaluation
- Dr. Jay Davidson - Lyme Disease EbookDocument35 pagesDr. Jay Davidson - Lyme Disease EbookFlo BorsPas encore d'évaluation
- 6BI04 01 Que 20130111Document24 pages6BI04 01 Que 20130111Fathmath MohamedPas encore d'évaluation
- Risk Factors For Non-Communicable Diseases Among Adults of 25-65 Years at Kakamega County General Hospital, KenyaDocument9 pagesRisk Factors For Non-Communicable Diseases Among Adults of 25-65 Years at Kakamega County General Hospital, KenyaIJPHSPas encore d'évaluation
- Lowndes County Schools Return To School PlanDocument12 pagesLowndes County Schools Return To School PlanWTXL ABC27Pas encore d'évaluation