Vous aimerez peut-être aussi
- Pain Disability IndexDocument3 pagesPain Disability IndexscribdseewalPas encore d'évaluation
- Pain Disability IndexDocument4 pagesPain Disability Indexapi-496718295Pas encore d'évaluation
- GordonsDocument2 pagesGordonsAngelica OctotPas encore d'évaluation
- Pain Assessment in Older Adults Post Viewing ReportDocument2 pagesPain Assessment in Older Adults Post Viewing ReportLiam HenryPas encore d'évaluation
- Physical Assessment FormDocument14 pagesPhysical Assessment FormHedda Melriz DelimaPas encore d'évaluation
- Chiropractic Intake FormDocument4 pagesChiropractic Intake FormtmontagPas encore d'évaluation
- Case Study IcuDocument31 pagesCase Study Icujanna mae patriarcaPas encore d'évaluation
- PT Intake FormDocument4 pagesPT Intake FormChifor FlorinPas encore d'évaluation
- 130 Physicians-Report 7-21-2023Document2 pages130 Physicians-Report 7-21-2023medisnadaPas encore d'évaluation
- Dmas 99Document7 pagesDmas 99Billie_anderson2473Pas encore d'évaluation
- RFC Form (Physical)Document2 pagesRFC Form (Physical)dvolmy321Pas encore d'évaluation
- Sleep 50 QuestionnaireDocument5 pagesSleep 50 QuestionnaireSónia Alves100% (1)
- Health 8: Learning Activity Sheet Communicable DiseaseDocument5 pagesHealth 8: Learning Activity Sheet Communicable DiseaseJoeffrie G. CostalesPas encore d'évaluation
- Try This Pain Assessment Scale For People With DementiaDocument9 pagesTry This Pain Assessment Scale For People With DementiaElPas encore d'évaluation
- GEC Interview QuestionsDocument1 pageGEC Interview QuestionsTESL10621 Shameen Farah Binti Mohd AminPas encore d'évaluation
- Intake Form Page 2Document1 pageIntake Form Page 2Casey OrrPas encore d'évaluation
- IMCI Form2Document18 pagesIMCI Form2Cristina Bantilan MontenegroPas encore d'évaluation
- Back Pain Follow-UpDocument3 pagesBack Pain Follow-Upbarros6Pas encore d'évaluation
- Sleep Disorders Residual Functional Capacity QuestionnaireDocument3 pagesSleep Disorders Residual Functional Capacity QuestionnaireDellComputer99Pas encore d'évaluation
- Advance Care Plan BlankDocument3 pagesAdvance Care Plan BlankJanine Anderson100% (1)
- Form "D" Report of Practical Experience: Nursing Clinical Practice IDocument29 pagesForm "D" Report of Practical Experience: Nursing Clinical Practice IAnderson RebaPas encore d'évaluation
- Headaches Residual Functional Capacity QuestionnaireDocument3 pagesHeadaches Residual Functional Capacity QuestionnaireDellComputer99Pas encore d'évaluation
- BOA Website Intake+Form 2017Document3 pagesBOA Website Intake+Form 2017joannaPas encore d'évaluation
- Health FormDocument2 pagesHealth Formapi-247535323Pas encore d'évaluation
- Barthel Index of Activities of Daily LivingDocument4 pagesBarthel Index of Activities of Daily LivingMaePas encore d'évaluation
- Learning Activity For Formulating Nursing HistoryDocument6 pagesLearning Activity For Formulating Nursing HistoryGadez JeanpelPas encore d'évaluation
- Cif NTDocument2 pagesCif NTIvy marie BonPas encore d'évaluation
- Guided Notes - Your Lifestyle and Your HealthDocument4 pagesGuided Notes - Your Lifestyle and Your HealthAdam Fingersen0% (1)
- FCM Research QuestionnaireDocument1 pageFCM Research QuestionnaireHermie Alexander SiaPas encore d'évaluation
- Today's Date: - Name: - Date of Birth - Phone Number: - Age: - Email AddressDocument2 pagesToday's Date: - Name: - Date of Birth - Phone Number: - Age: - Email Addressanedik40Pas encore d'évaluation
- Multan College of NursingDocument9 pagesMultan College of NursingM Kamran QadirPas encore d'évaluation
- Intake Form 2020 OctDocument7 pagesIntake Form 2020 Octapi-277069774Pas encore d'évaluation
- Assessment FormDocument11 pagesAssessment FormSumbul JakhuraPas encore d'évaluation
- Nursing Care PlanDocument3 pagesNursing Care PlanAirglow GPas encore d'évaluation
- Donna - S Las Health10-Day 2 - (Week 4)Document4 pagesDonna - S Las Health10-Day 2 - (Week 4)bonzai guillenaPas encore d'évaluation
- Las Health Q3W2 3 M SantosDocument3 pagesLas Health Q3W2 3 M SantosJanezzka Zyan CupcupinPas encore d'évaluation
- RFC 2 PAGE Physical 2010 With OnsetDocument2 pagesRFC 2 PAGE Physical 2010 With OnsetghobbiePas encore d'évaluation
- Health Science LabsDocument7 pagesHealth Science LabsHamza ElmoubarikPas encore d'évaluation
- Medical Health RecordDocument1 pageMedical Health RecordNikay SerdeñaPas encore d'évaluation
- Instrumen Bartel Index-DigabungkanDocument49 pagesInstrumen Bartel Index-DigabungkanDian Dinnar Eka SafitriPas encore d'évaluation
- Staff Health PDFDocument1 pageStaff Health PDFJorgePas encore d'évaluation
- School: E.E.S. Nº 4 Year 3 6 Teacher Yésica Pretzlaff: RD THDocument3 pagesSchool: E.E.S. Nº 4 Year 3 6 Teacher Yésica Pretzlaff: RD THMyriam PitrelliPas encore d'évaluation
- Initial Intake Form: Patient InformationDocument13 pagesInitial Intake Form: Patient InformationFernandoPas encore d'évaluation
- Wesleyan University - Philippines: N U R S I N G C A R e P L A NDocument3 pagesWesleyan University - Philippines: N U R S I N G C A R e P L A NKristine CastilloPas encore d'évaluation
- New Patient FormDocument7 pagesNew Patient Formhamzahali039Pas encore d'évaluation
- TraumainterviewDocument9 pagesTraumainterviewKathy RojasPas encore d'évaluation
- Patient Information Form 2017Document1 pagePatient Information Form 2017Merabo SimonishviliPas encore d'évaluation
- New Patient Paperwork (FINAL DRAFT)Document4 pagesNew Patient Paperwork (FINAL DRAFT)andrew_sokolPas encore d'évaluation
- Students Medical RecordDocument2 pagesStudents Medical RecordMary Grace EncisaPas encore d'évaluation
- The Limits of Consciousness Are Hard To Define Satisfactorily and We Can Only Infer The Self-Awareness of Others by Their Appearance The Their Acts.Document26 pagesThe Limits of Consciousness Are Hard To Define Satisfactorily and We Can Only Infer The Self-Awareness of Others by Their Appearance The Their Acts.DrGasnasPas encore d'évaluation
- Page 1 of 4: PPGNNJ 11/09 Confidential Property of Planned Parenthood of Greater Northern NJ, IncDocument4 pagesPage 1 of 4: PPGNNJ 11/09 Confidential Property of Planned Parenthood of Greater Northern NJ, IncTINALEETNT723Pas encore d'évaluation
- Confidential Patient Information: C L C CDocument6 pagesConfidential Patient Information: C L C CPedroPas encore d'évaluation
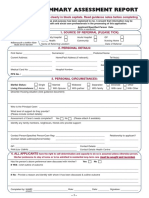
- Common Summary Assessment ReportDocument4 pagesCommon Summary Assessment ReportVaibhav DafalePas encore d'évaluation
- Bioethics Session 16 SASDocument4 pagesBioethics Session 16 SASAnthony BadiliPas encore d'évaluation
- Apta Eval-Fax Version Asapt 2007Document4 pagesApta Eval-Fax Version Asapt 2007Abdur RasyidPas encore d'évaluation
- My Personal Health RecordDocument2 pagesMy Personal Health RecordKimmi Joy BakerPas encore d'évaluation
- Medical Attendants Certificate17062019Document2 pagesMedical Attendants Certificate17062019PrathameshPas encore d'évaluation
- Healthcare Services: ObjectiveDocument7 pagesHealthcare Services: ObjectiveRubiks C. AddamsPas encore d'évaluation
- Dbt: Discovering Your Courage for Change and Commitment to Yourself (Mindfulness and Emotion Regulation Techniques for Overcoming Stress)D'EverandDbt: Discovering Your Courage for Change and Commitment to Yourself (Mindfulness and Emotion Regulation Techniques for Overcoming Stress)Pas encore d'évaluation
- Oblicon NotesDocument14 pagesOblicon NotesCee Silo Aban100% (1)
- Chemical and Biological Weapons Chair ReportDocument9 pagesChemical and Biological Weapons Chair ReportHong Kong MUN 2013100% (1)
- Managerial Accounting 14th Edition Warren Solutions Manual DownloadDocument28 pagesManagerial Accounting 14th Edition Warren Solutions Manual DownloadRose Speers100% (22)
- Text Al Capone B1Document2 pagesText Al Capone B1Andjela JevremovicPas encore d'évaluation
- 1040 A Day in The Life of A Veterinary Technician PDFDocument7 pages1040 A Day in The Life of A Veterinary Technician PDFSedat KorkmazPas encore d'évaluation
- Unit 25 Sound Recording Lab LacDocument16 pagesUnit 25 Sound Recording Lab Lacapi-471521676Pas encore d'évaluation
- Vince - Michael - Intermediate - Language Assive 1Document5 pagesVince - Michael - Intermediate - Language Assive 1Николай КолевPas encore d'évaluation
- Book Review "The TKT Course Clil Module"Document8 pagesBook Review "The TKT Course Clil Module"Alexander DeckerPas encore d'évaluation
- Principle of ManagementsDocument77 pagesPrinciple of ManagementsJayson LucenaPas encore d'évaluation
- Syllabus Tourism Laws CKSCDocument6 pagesSyllabus Tourism Laws CKSCDennis Go50% (2)
- Due Process of LawDocument2 pagesDue Process of Lawjoe100% (4)
- Gremath Set8-1Document48 pagesGremath Set8-1uzairmetallurgistPas encore d'évaluation
- The Spartacus Workout 2Document13 pagesThe Spartacus Workout 2PaulFM2100% (1)
- Sol2e Printables Unit 5ADocument2 pagesSol2e Printables Unit 5AGeorgio SentialiPas encore d'évaluation
- @PAKET A - TPM BAHASA INGGRIS KuDocument37 pages@PAKET A - TPM BAHASA INGGRIS KuRamona DessiatriPas encore d'évaluation
- ProjectDocument1 pageProjectDevil KingPas encore d'évaluation
- Teaching Students With High Incidence Disabilities Strategies For Diverse Classrooms 1St Edition Prater Test Bank Full Chapter PDFDocument35 pagesTeaching Students With High Incidence Disabilities Strategies For Diverse Classrooms 1St Edition Prater Test Bank Full Chapter PDFvaleriewashingtonfsnxgzyjbi100% (6)
- Cambridge Assessment International Education: Information Technology 9626/13 May/June 2019Document10 pagesCambridge Assessment International Education: Information Technology 9626/13 May/June 2019katiaPas encore d'évaluation
- Chapter 2: Related Theoretical Design Inputs 2.1 Sihwa Lake Tidal Power StationDocument9 pagesChapter 2: Related Theoretical Design Inputs 2.1 Sihwa Lake Tidal Power Stationaldrin leePas encore d'évaluation
- Aficionado PERDocument19 pagesAficionado PERMaecaella LlorentePas encore d'évaluation
- EpitheliumDocument48 pagesEpitheliumdrpankaj28100% (1)
- Proximity Principle of DesignDocument6 pagesProximity Principle of DesignSukhdeepPas encore d'évaluation
- (2010) Formulaic Language and Second Language Speech Fluency - Background, Evidence and Classroom Applications-Continuum (2010)Document249 pages(2010) Formulaic Language and Second Language Speech Fluency - Background, Evidence and Classroom Applications-Continuum (2010)Như Đặng QuếPas encore d'évaluation
- Balochistan Civil Servants (Appointment, Promotion and Transfer) Rules 2009 (22222)Document42 pagesBalochistan Civil Servants (Appointment, Promotion and Transfer) Rules 2009 (22222)Zarak KhanPas encore d'évaluation
- Exotic - March 2014Document64 pagesExotic - March 2014Almir Momenth35% (23)
- Violin Teaching in The New Millennium or Remembering The Future of Violin Performance by Gwendolyn Masin For Trinity College 2012Document241 pagesViolin Teaching in The New Millennium or Remembering The Future of Violin Performance by Gwendolyn Masin For Trinity College 2012Matheus Felipe Lessa Oliveira100% (4)
- Tesla, Inc.: Jump To Navigation Jump To Search Tesla Induction Motor AC MotorDocument90 pagesTesla, Inc.: Jump To Navigation Jump To Search Tesla Induction Motor AC MotorEdi RaduPas encore d'évaluation
- Mechanical Engineering Research PapersDocument8 pagesMechanical Engineering Research Papersfvfzfa5d100% (1)
- Paras Vs ComelecDocument2 pagesParas Vs ComelecAngel VirayPas encore d'évaluation
- Mercury and The WoodmanDocument1 pageMercury and The WoodmanLum Mei YeuanPas encore d'évaluation