Vous aimerez peut-être aussi
- Anti-VEGF Agents and Their Clinical Applications: Dr. Sriniwas Atal MD. Resident OphthalmologyDocument67 pagesAnti-VEGF Agents and Their Clinical Applications: Dr. Sriniwas Atal MD. Resident OphthalmologySriniwasPas encore d'évaluation
- Aflibercept (VEGF Trap-Eye) : The Newest anti-VEGF Drug: Michael W StewartDocument4 pagesAflibercept (VEGF Trap-Eye) : The Newest anti-VEGF Drug: Michael W StewartYuliyanaPas encore d'évaluation
- 933 001abedi2013Document7 pages933 001abedi20136jprsrbhkcPas encore d'évaluation
- Anti VEGF Therapy in OphthalmologyDocument27 pagesAnti VEGF Therapy in OphthalmologyAtreyee Bhattacharya100% (3)
- Retina 42 2243Document8 pagesRetina 42 2243mauriciosagredoPas encore d'évaluation
- Visual Acuity Outcomes and Anti-Vascular Endothelial Growth Factor Therapy Intensity in Neovascular Age-Related Macular Degeneration Patients A Real-World Analysis of 49 485 EyesDocument12 pagesVisual Acuity Outcomes and Anti-Vascular Endothelial Growth Factor Therapy Intensity in Neovascular Age-Related Macular Degeneration Patients A Real-World Analysis of 49 485 EyesmaleticjPas encore d'évaluation
- tmp5D2D TMPDocument4 pagestmp5D2D TMPFrontiersPas encore d'évaluation
- Anti Vegf Drugs in The Prevention of BlindnessDocument3 pagesAnti Vegf Drugs in The Prevention of BlindnessIndra PermanaPas encore d'évaluation
- PS Mahar 1Document5 pagesPS Mahar 1ErickeePas encore d'évaluation
- Aflibercept - Preclinical Efficacy and Safety of VEGF-Grab, A Novel Anti-VEGF Drug, and Its Comparison To AfliberceptDocument9 pagesAflibercept - Preclinical Efficacy and Safety of VEGF-Grab, A Novel Anti-VEGF Drug, and Its Comparison To AfliberceptCher IshPas encore d'évaluation
- 2004-08-02 Epzicom GlaxoSmithKline - Treatment For HIV InfectionDocument4 pages2004-08-02 Epzicom GlaxoSmithKline - Treatment For HIV InfectionShuona YuanPas encore d'évaluation
- Anti VEGFsDocument4 pagesAnti VEGFsVishPas encore d'évaluation
- Salma Case Series On Intravitreal Anti Vascular Endothelial Growth Factor Therapy Response in Retinopathy of Prematurity - Mia NursalamahDocument15 pagesSalma Case Series On Intravitreal Anti Vascular Endothelial Growth Factor Therapy Response in Retinopathy of Prematurity - Mia NursalamahalbaazaPas encore d'évaluation
- 2020 - 10.1007 - s00347 020 01250 yDocument10 pages2020 - 10.1007 - s00347 020 01250 yEko NoviantiPas encore d'évaluation
- Retinal Reperfusion in Diabetic Retinopathy Following Treatment With anti-VEGF Intravitreal InjectionsDocument10 pagesRetinal Reperfusion in Diabetic Retinopathy Following Treatment With anti-VEGF Intravitreal InjectionsAzizan HakimPas encore d'évaluation
- Anti - VEGF Agents: Presenter - Dr. Karan. A. K Moderator - Dr. Hemalatha .B.CDocument44 pagesAnti - VEGF Agents: Presenter - Dr. Karan. A. K Moderator - Dr. Hemalatha .B.CKaran Kumarswamy100% (1)
- Terpai Afli BerceptDocument12 pagesTerpai Afli Berceptanon_890511420Pas encore d'évaluation
- BR Med Bull-2013-Sivaprasad-201-11 PDFDocument11 pagesBR Med Bull-2013-Sivaprasad-201-11 PDFKarina Mega WPas encore d'évaluation
- 2006 Retina. Manzano. Testing IV Toxicity of AvastinDocument5 pages2006 Retina. Manzano. Testing IV Toxicity of Avastinmaria_mzPas encore d'évaluation
- Anti VEGFDocument43 pagesAnti VEGFanantkumar85Pas encore d'évaluation
- Persistent Elevation of Intraocular Pressure Following Intravitreal Injection of BevacizumabDocument4 pagesPersistent Elevation of Intraocular Pressure Following Intravitreal Injection of Bevacizumab6jprsrbhkcPas encore d'évaluation
- DR Abhishek Das Final ThesisDocument86 pagesDR Abhishek Das Final Thesissankhasubhra mandalPas encore d'évaluation
- Intravitreal Bevacizumab: Indications and Complications: Original ArticleDocument5 pagesIntravitreal Bevacizumab: Indications and Complications: Original ArticleVlady BordaPas encore d'évaluation
- Anti VEGF 2020Document18 pagesAnti VEGF 2020Denisse LizarragaPas encore d'évaluation
- CCO VEGF GI Cancers DownloadableDocument79 pagesCCO VEGF GI Cancers DownloadableOtilia SerescuPas encore d'évaluation
- International Journal of Case Reports (ISSN:2572-8776) Loading Doses of Bevacizumab in Branch Retinal Vein Occlusion (BRVO) : A Case ReportDocument5 pagesInternational Journal of Case Reports (ISSN:2572-8776) Loading Doses of Bevacizumab in Branch Retinal Vein Occlusion (BRVO) : A Case ReportPeony PinkPas encore d'évaluation
- Jurnal Reading DR Sofi SiapDocument28 pagesJurnal Reading DR Sofi SiapBima Bayu PutraPas encore d'évaluation
- Most Expensive Treatments in The US 16825Document8 pagesMost Expensive Treatments in The US 16825Francisco TellecheaPas encore d'évaluation
- Anti Vascular Endothelial Growth Factors in Management of Diabetic Macular EdemaDocument9 pagesAnti Vascular Endothelial Growth Factors in Management of Diabetic Macular EdemaPutri kartiniPas encore d'évaluation
- Treatment of Exudative Age-Related Macular DegenerationDocument2 pagesTreatment of Exudative Age-Related Macular DegenerationAgiu BogdanPas encore d'évaluation
- Jurnal Retinopaty DiabetikumDocument11 pagesJurnal Retinopaty DiabetikumrestikaPas encore d'évaluation
- Jo 2014Document8 pagesJo 2014yalocim666Pas encore d'évaluation
- Seminar Pre EclampsiaDocument50 pagesSeminar Pre EclampsiaManan BoobPas encore d'évaluation
- Aflibercept - VEGF-Trap A VEGF Blocker With Potentantitumor EffectsDocument6 pagesAflibercept - VEGF-Trap A VEGF Blocker With Potentantitumor EffectsCher IshPas encore d'évaluation
- VAPP Assessment in Nigeria - Training - SODocument41 pagesVAPP Assessment in Nigeria - Training - SOTella AdedamolaPas encore d'évaluation
- The Effect of Bevacizumab Versus Ranibizumab in The Treatment of Corneal NeovascularizationDocument8 pagesThe Effect of Bevacizumab Versus Ranibizumab in The Treatment of Corneal NeovascularizationmestevezfPas encore d'évaluation
- Recent Us Fda Approved MedicinesDocument17 pagesRecent Us Fda Approved MedicinesNAMAN KOTHARIPas encore d'évaluation
- VEGF and AngiogénesisDocument7 pagesVEGF and AngiogénesisMiranda YareliPas encore d'évaluation
- Expression of Vascular Endothelial Growth Factor (VEGF) and New Blood Vessels Formation On Wound Incision Post Ropivacaine Administration in Animal ModelDocument8 pagesExpression of Vascular Endothelial Growth Factor (VEGF) and New Blood Vessels Formation On Wound Incision Post Ropivacaine Administration in Animal ModelInternational Journal of Innovative Science and Research TechnologyPas encore d'évaluation
- ROP - Newer Treatment ModalitiesDocument24 pagesROP - Newer Treatment ModalitiesSiva RamakrishnanPas encore d'évaluation
- Two-Year Outcomes of Treat-and-ExtendDocument10 pagesTwo-Year Outcomes of Treat-and-ExtendPutri kartiniPas encore d'évaluation
- FDA's Role in Overseeing Vaccine Development, Approval and Post-Marketing SurveillanceDocument20 pagesFDA's Role in Overseeing Vaccine Development, Approval and Post-Marketing SurveillanceNational Press FoundationPas encore d'évaluation
- Journal ClubDocument31 pagesJournal Clubapi-669676793Pas encore d'évaluation
- Esc 150003Document5 pagesEsc 150003marlon GarcíaPas encore d'évaluation
- Guidelines On The Use of Intravenous Immune Globulin For Hematologic ConditionsDocument48 pagesGuidelines On The Use of Intravenous Immune Globulin For Hematologic ConditionssarahulfaaPas encore d'évaluation
- AllergeneDocument41 pagesAllergenesmartPas encore d'évaluation
- Immunity 4Document76 pagesImmunity 4Dr.vinod ParmarPas encore d'évaluation
- Modulation of Bevacizumab-Induced Toxicity For Cultured Human Corneal FibroblastsDocument10 pagesModulation of Bevacizumab-Induced Toxicity For Cultured Human Corneal FibroblastsmestevezfPas encore d'évaluation
- Ray 2012Document7 pagesRay 2012Nguyen Minh PhuPas encore d'évaluation
- Managing Itp at Home With Ivig: Marilyn Hanchett RN PHDDocument34 pagesManaging Itp at Home With Ivig: Marilyn Hanchett RN PHDLisa R GreenPas encore d'évaluation
- Cruise Study Journal ClubDocument47 pagesCruise Study Journal ClubRana AhmedPas encore d'évaluation
- Emerald Bioscience: Corporate PresentationDocument31 pagesEmerald Bioscience: Corporate PresentationRodolpho C. BragaPas encore d'évaluation
- Retinopathy of Prematurity: GGW Adams Moorfields Eye Hospital, LondonDocument29 pagesRetinopathy of Prematurity: GGW Adams Moorfields Eye Hospital, LondonJuan R. AntunezPas encore d'évaluation
- Efficacy of Bevacizumab, Ranibizumab, and Aflibercept For Treatment of Macular Edema Secondary To Retinal Vein OcclusionDocument15 pagesEfficacy of Bevacizumab, Ranibizumab, and Aflibercept For Treatment of Macular Edema Secondary To Retinal Vein OcclusionUlul AzmiPas encore d'évaluation
- Retina 39 426Document9 pagesRetina 39 426ryaalwiPas encore d'évaluation
- Single-Dose Versus Multiple-Dose Antibiotics Prophylaxis For Preventing Caesarean Section Postpartum Infections: A Randomized Controlled TrialDocument8 pagesSingle-Dose Versus Multiple-Dose Antibiotics Prophylaxis For Preventing Caesarean Section Postpartum Infections: A Randomized Controlled Trial18. Lusiana Aprilia SariPas encore d'évaluation
- S 000 LBLDocument15 pagesS 000 LBLزيد هشام السيدPas encore d'évaluation
- Intravitreal Injection of Bevacizumab: Review of Our Previous ExperienceDocument6 pagesIntravitreal Injection of Bevacizumab: Review of Our Previous ExperienceShintya DewiPas encore d'évaluation
- Intravenous ImmunoglobulinDocument6 pagesIntravenous ImmunoglobulinAnastasia TjanPas encore d'évaluation
- Drug StudyyDocument5 pagesDrug StudyyKiana Garlitos CasasPas encore d'évaluation
- What Is Biopharmaceutics?: Brand NameDocument10 pagesWhat Is Biopharmaceutics?: Brand NameAhmad Jamal HashmiPas encore d'évaluation
- VitiligoDocument13 pagesVitiligoFebyan AbotPas encore d'évaluation
- 1 s2.0 S0169409X16300552 MainDocument19 pages1 s2.0 S0169409X16300552 MainpavaniPas encore d'évaluation
- BSPH 307 Hospital Pharmacy PracticeDocument1 pageBSPH 307 Hospital Pharmacy PracticeCZYRA O. CUBALPas encore d'évaluation
- Pharmacy Time Table 2023-2024 1st IsseDocument8 pagesPharmacy Time Table 2023-2024 1st IsseIhtisham SafdarPas encore d'évaluation
- MBS Price List April 2021Document50 pagesMBS Price List April 2021Anonymous aaAQ6dgPas encore d'évaluation
- Mutu Farmasi Jan 24Document9 pagesMutu Farmasi Jan 24Fenny Aliska Larasaty WijayaPas encore d'évaluation
- Jurnal FE Kelompok 3 PDFDocument10 pagesJurnal FE Kelompok 3 PDFNur Kamilah IdzanPas encore d'évaluation
- QAS04 093rev4 FinalDocument39 pagesQAS04 093rev4 FinalRemi BoxiplentiPas encore d'évaluation
- Akson College of Health Sciences Mirpur AjkDocument48 pagesAkson College of Health Sciences Mirpur AjkAlna TechnicalPas encore d'évaluation
- NPB 168 Practice Exam 1Document4 pagesNPB 168 Practice Exam 1Kim WongPas encore d'évaluation
- CBT OutlineDocument2 pagesCBT OutlineRoss Laurenne FortunadoPas encore d'évaluation
- HematologyDocument28 pagesHematologyCarlos HernándezPas encore d'évaluation
- Pharmacy Critical CareDocument136 pagesPharmacy Critical CareTohShengPoo100% (1)
- KAPS SyllabusDocument1 pageKAPS Syllabusbeastwithin0004Pas encore d'évaluation
- The Treatment of Stage IV CancersDocument6 pagesThe Treatment of Stage IV CancersAnthony SullivanPas encore d'évaluation
- 384-File Utama Naskah-928-2-10-20210630Document19 pages384-File Utama Naskah-928-2-10-20210630Jeremia TogatoropPas encore d'évaluation
- An Overview On Asenapine MaleateDocument6 pagesAn Overview On Asenapine MaleatePetar DimkovPas encore d'évaluation
- Ncma 113 - FinalsDocument44 pagesNcma 113 - FinalsElay AbongPas encore d'évaluation
- Introduction To BiopharmaceuticsDocument4 pagesIntroduction To BiopharmaceuticsIvymae TrillesPas encore d'évaluation
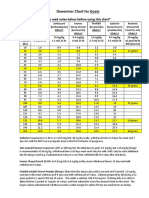
- Dewormer Chart GoatsDocument2 pagesDewormer Chart GoatsAbu Bakr AtikuPas encore d'évaluation
- Stenting of Bifucartion Lesions Classification, Treatment, and ResultsDocument10 pagesStenting of Bifucartion Lesions Classification, Treatment, and ResultsmonicamoniccPas encore d'évaluation
- In Memoriam of Dr. David White, PHD, FRCPath (1946-2017) Canadian Journal of SurgeryDocument1 pageIn Memoriam of Dr. David White, PHD, FRCPath (1946-2017) Canadian Journal of SurgeryVivian McAlisterPas encore d'évaluation
- Management For OsteosarcomaDocument2 pagesManagement For OsteosarcomakyawPas encore d'évaluation
- Paparan FGD - GP JamuDocument49 pagesPaparan FGD - GP JamuDewita AgusPas encore d'évaluation
- Guidance On Converting Between Anticoagulant RegimensDocument4 pagesGuidance On Converting Between Anticoagulant Regimenskratai NPas encore d'évaluation
- 1Document12 pages1RAED GhunaimPas encore d'évaluation
- Code Blue System: Hospital Sultanah Aminah Johor BahruDocument15 pagesCode Blue System: Hospital Sultanah Aminah Johor BahrumursidahanimPas encore d'évaluation
- Psychiatric Nursing Knowledge and Skills ChecklistDocument5 pagesPsychiatric Nursing Knowledge and Skills Checklistnorthweststaffing100% (4)