Vous aimerez peut-être aussi
- US Immigration Exam Study Guide in English and Albanian: Study Guides for the US Immigration TestD'EverandUS Immigration Exam Study Guide in English and Albanian: Study Guides for the US Immigration TestPas encore d'évaluation
- Request For Fee WaiverDocument11 pagesRequest For Fee WaiverWilma OcampoPas encore d'évaluation
- I-130 TONY 3 19 2020 OK (3) CorregidoDocument12 pagesI-130 TONY 3 19 2020 OK (3) Corregidoezra montoya velascoPas encore d'évaluation
- Form I-485, Application To Register Permanent Residence or Adjust StatusDocument6 pagesForm I-485, Application To Register Permanent Residence or Adjust Statusw_tahanPas encore d'évaluation
- Petition For Amerasian, Widow (Er), or Special Immigrant: Uscis Form I-360Document19 pagesPetition For Amerasian, Widow (Er), or Special Immigrant: Uscis Form I-360vicky4009Pas encore d'évaluation
- I 130Document12 pagesI 130ramnik20098676100% (1)
- Petition For Alien Relative: U.S. Citizenship and Immigration ServicesDocument12 pagesPetition For Alien Relative: U.S. Citizenship and Immigration ServicesNanik AstutiPas encore d'évaluation
- Application I-130Document18 pagesApplication I-130ya decidiPas encore d'évaluation
- Petition To Remove Conditions On Residence: U.S. Citizenship and Immigration ServicesDocument11 pagesPetition To Remove Conditions On Residence: U.S. Citizenship and Immigration ServicesAustin Smith100% (1)
- Petition For Alien Relative: U.S. Citizenship and Immigration ServicesDocument12 pagesPetition For Alien Relative: U.S. Citizenship and Immigration ServicesLismar DelgadoPas encore d'évaluation
- Planillas para Firma I-589Document3 pagesPlanillas para Firma I-589Andrea HernandezPas encore d'évaluation
- Electronic Form Only: Petition For Alien RelativeDocument18 pagesElectronic Form Only: Petition For Alien RelativeFelipe AmorosoPas encore d'évaluation
- I-130 Formato Solicitud de FamiliarDocument12 pagesI-130 Formato Solicitud de FamiliarLeopoldo PerezPas encore d'évaluation
- Form I-485, Application To Register Permanent Residence or Adjust StatusDocument6 pagesForm I-485, Application To Register Permanent Residence or Adjust StatusAnonymous MMKc1kkPPas encore d'évaluation
- I-130 Petition For Alien RelativeDocument20 pagesI-130 Petition For Alien RelativeCesar MaraverPas encore d'évaluation
- Electronic Form Only: Petition For Alien RelativeDocument14 pagesElectronic Form Only: Petition For Alien RelativeDewan Ahmed SaifPas encore d'évaluation
- Petition For A Nonimmigrant Worker: U.S. Citizenship and Immigration ServicesDocument36 pagesPetition For A Nonimmigrant Worker: U.S. Citizenship and Immigration Servicesdavidbiliy110Pas encore d'évaluation
- Sample Form I130 Petition For Alien Relative PDFDocument12 pagesSample Form I130 Petition For Alien Relative PDFAnnaPas encore d'évaluation
- Federal Information Worksheet 2018: Jerry Pryde J JR 570-86-7356 DisabledDocument1 pageFederal Information Worksheet 2018: Jerry Pryde J JR 570-86-7356 Disabledsherrif douchebagPas encore d'évaluation
- Petition For A Nonimmigrant Worker: U.S. Citizenship and Immigration ServicesDocument12 pagesPetition For A Nonimmigrant Worker: U.S. Citizenship and Immigration ServicesDUY PHAM QUANGPas encore d'évaluation
- Petition For Alien Relative: Department of Homeland Security Form I-130Document4 pagesPetition For Alien Relative: Department of Homeland Security Form I-130Hamedo SalmanPas encore d'évaluation
- N 400Document20 pagesN 400Leo FerrPas encore d'évaluation
- Petition For Alien Relative: Department of Homeland Security Form I-130Document5 pagesPetition For Alien Relative: Department of Homeland Security Form I-130Hamedo SalmanPas encore d'évaluation
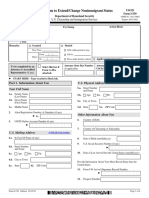
- Application To Extend/Change Nonimmigrant Status: Uscis Form I-539Document8 pagesApplication To Extend/Change Nonimmigrant Status: Uscis Form I-539James Jean-louisPas encore d'évaluation
- 5.tax Interview Questions Virtual Interview FiverrDocument4 pages5.tax Interview Questions Virtual Interview Fiverrfrantzloppe05Pas encore d'évaluation
- Petition For A Nonimmigrant Worker: U.S. Citizenship and Immigration ServicesDocument36 pagesPetition For A Nonimmigrant Worker: U.S. Citizenship and Immigration ServicesKim BadilloPas encore d'évaluation
- Register To Vote Anonymously Resident in EnglandDocument6 pagesRegister To Vote Anonymously Resident in EnglandRyan SmithPas encore d'évaluation
- Applying To Become A Member of The Discovery Health Medical Scheme 2018Document15 pagesApplying To Become A Member of The Discovery Health Medical Scheme 2018simbamikePas encore d'évaluation
- Petition For A Nonimmigrant Worker: U.S. Citizenship and Immigration ServicesDocument36 pagesPetition For A Nonimmigrant Worker: U.S. Citizenship and Immigration ServicesDaniel JonasPas encore d'évaluation
- Preview: Petition For A Nonimmigrant Worker: H1 ClassificationsDocument17 pagesPreview: Petition For A Nonimmigrant Worker: H1 ClassificationsSai Sunil ChandraaPas encore d'évaluation
- Petition For A Nonimmigrant Worker: U.S. Citizenship and Immigration ServicesDocument36 pagesPetition For A Nonimmigrant Worker: U.S. Citizenship and Immigration ServicesAnthony Gelig MontemayorPas encore d'évaluation
- I 134 PDFDocument8 pagesI 134 PDFKharbanda AcadmeyPas encore d'évaluation
- FORM I-129 (Completed On 9th October)Document36 pagesFORM I-129 (Completed On 9th October)KJ JaganPas encore d'évaluation
- Application To Register Permanent Residence or Adjust StatusDocument20 pagesApplication To Register Permanent Residence or Adjust StatusLuis ManotasPas encore d'évaluation
- Formulario n4003Document20 pagesFormulario n4003andykam26Pas encore d'évaluation
- Affidavit of Support: Part 1. Information About YouDocument8 pagesAffidavit of Support: Part 1. Information About YouRaini TorresPas encore d'évaluation
- Application To Register Permanent Residence or Adjust StatusDocument18 pagesApplication To Register Permanent Residence or Adjust StatusCristian BurnPas encore d'évaluation
- I 864 PDFDocument12 pagesI 864 PDFfrancisPas encore d'évaluation
- Statement of Live Birth: Vital Statistics ActDocument4 pagesStatement of Live Birth: Vital Statistics ActF rPas encore d'évaluation
- Appendix V Family Part Case Information Statement This Form and Attachments Are Confidential Pursuant To Rules 1:38-3 (D) (1) and 5:5-2 (F)Document10 pagesAppendix V Family Part Case Information Statement This Form and Attachments Are Confidential Pursuant To Rules 1:38-3 (D) (1) and 5:5-2 (F)Nard CruzPas encore d'évaluation
- N-600, Application For Certificate of CitizenshipDocument0 pageN-600, Application For Certificate of CitizenshipTaleen SakayanPas encore d'évaluation
- Perdon de Pago I-912Document11 pagesPerdon de Pago I-912ChrisPas encore d'évaluation
- Liheap ApplicationDocument10 pagesLiheap ApplicationSon BurnyoazPas encore d'évaluation
- US Internal Revenue Service: f13614Document2 pagesUS Internal Revenue Service: f13614IRSPas encore d'évaluation
- Application For Citizenship and Issuance of Certificate Under Section 322Document13 pagesApplication For Citizenship and Issuance of Certificate Under Section 322Julio OrtegaPas encore d'évaluation
- Questionnaire For Prospective Senate AppointeesDocument24 pagesQuestionnaire For Prospective Senate AppointeesCity Room100% (2)
- Formulario I 129Document36 pagesFormulario I 129Sandra YPPas encore d'évaluation
- Petition For A Nonimmigrant WorkerDocument16 pagesPetition For A Nonimmigrant WorkerulrichPas encore d'évaluation
- Pacific Access Category: Registration FormDocument8 pagesPacific Access Category: Registration FormSaif KhanPas encore d'évaluation
- N 400Document10 pagesN 400joshuayoon100% (1)
- Lleno I-589 PDFDocument12 pagesLleno I-589 PDFDiegou MaurixiouPas encore d'évaluation
- Form I-134, Affidavit of Support: Residing atDocument2 pagesForm I-134, Affidavit of Support: Residing atCrissy cavePas encore d'évaluation
- Form I-914Document12 pagesForm I-914ani preciadoPas encore d'évaluation
- Immigration and Family Law: An Attorney's Toolbox of Best PracticesD'EverandImmigration and Family Law: An Attorney's Toolbox of Best PracticesPas encore d'évaluation
- Immigration: A Fiance Petition Document Preparation Reference.D'EverandImmigration: A Fiance Petition Document Preparation Reference.Pas encore d'évaluation
- A Simple Guide to the Immigration Laws of the United States: What You Need to Know When You Come to AmericaD'EverandA Simple Guide to the Immigration Laws of the United States: What You Need to Know When You Come to AmericaÉvaluation : 1 sur 5 étoiles1/5 (1)
- US Immigration Exam Study Guide in English and AlbanianD'EverandUS Immigration Exam Study Guide in English and AlbanianÉvaluation : 1 sur 5 étoiles1/5 (2)
- School ListDocument4 pagesSchool ListRohit DsouzaPas encore d'évaluation
- STAR StrategyDocument4 pagesSTAR Strategyne_sullivanPas encore d'évaluation
- Ipcrf - Teacher 1 Final (Lacticse)Document35 pagesIpcrf - Teacher 1 Final (Lacticse)Christine De San JosePas encore d'évaluation
- Bihar School Examination Board, PatnaDocument1 pageBihar School Examination Board, PatnaChandan SharmaPas encore d'évaluation
- PSSA Grade 3 Math Sampler 2008Document110 pagesPSSA Grade 3 Math Sampler 2008Iris_04100% (1)
- W2 Day 2 and Day 3 J. RifeDocument9 pagesW2 Day 2 and Day 3 J. Rifeuniversaljuly100% (3)
- Intramurals Guidelines and Criteria 2022Document2 pagesIntramurals Guidelines and Criteria 2022Maria Sarah Del MundoPas encore d'évaluation
- Field Study 1: Dinalupihan Elementary SchoolDocument20 pagesField Study 1: Dinalupihan Elementary SchoolJimcris villamorPas encore d'évaluation
- Causes of Antisocial Behavior of AdolescentsDocument14 pagesCauses of Antisocial Behavior of AdolescentsGiulianaSantosAramburuPas encore d'évaluation
- 2019 Respiratory Care Education AnnualDocument64 pages2019 Respiratory Care Education AnnualGustavo OlguinPas encore d'évaluation
- EAPP-Week 9Document4 pagesEAPP-Week 9rose suarezPas encore d'évaluation
- School Action Plan in MAPEH S.Y. 2017 2018Document3 pagesSchool Action Plan in MAPEH S.Y. 2017 2018Elmalyn BernartePas encore d'évaluation
- Grammar - Passives - OnestopenglishDocument5 pagesGrammar - Passives - OnestopenglishDragoljub RadonjicPas encore d'évaluation
- Clinical Legal Education in India: A Contemporary Legal PedagogyDocument17 pagesClinical Legal Education in India: A Contemporary Legal PedagogySudev SinghPas encore d'évaluation
- Parents Play A Major Role in The Life of A ChildDocument3 pagesParents Play A Major Role in The Life of A ChildJmann JulaihiPas encore d'évaluation
- FdxgfgfhgfytiuyiuyihkjnkjDocument2 pagesFdxgfgfhgfytiuyiuyihkjnkjAkhil DevPas encore d'évaluation
- Schedules 2Document1 383 pagesSchedules 2api-241741490Pas encore d'évaluation
- Cross Cultural Communication Techniques and Negotiation Skills From International Business and DiplomacyDocument19 pagesCross Cultural Communication Techniques and Negotiation Skills From International Business and Diplomacy555junaidPas encore d'évaluation
- Division of Batangas: Pacucoa MeetingDocument5 pagesDivision of Batangas: Pacucoa MeetingVel Garcia CorreaPas encore d'évaluation
- My Personal Philosophy of EducationDocument7 pagesMy Personal Philosophy of Educationapi-250901151100% (1)
- One Grain of RiceDocument8 pagesOne Grain of RiceJay WrightPas encore d'évaluation
- Challan Form PDFDocument3 pagesChallan Form PDFArbab HaiderPas encore d'évaluation
- Kenya Education PlanDocument298 pagesKenya Education PlanTeachers Without Borders100% (2)
- Anna Miller Art Education Resume Classes in TablesDocument5 pagesAnna Miller Art Education Resume Classes in Tablesapi-488515294Pas encore d'évaluation
- Spus Thesis Writing 2Document71 pagesSpus Thesis Writing 2Edpher Leo SindolPas encore d'évaluation
- EDCI 517 F17 Reaves SyllabusDocument9 pagesEDCI 517 F17 Reaves Syllabusfostersds1Pas encore d'évaluation
- Sten HouseDocument17 pagesSten HouseNurshazlie AliPas encore d'évaluation
- Bulletin 2018-19 Grad EngineeringDocument109 pagesBulletin 2018-19 Grad EngineeringLuciana Mendoza FlorezPas encore d'évaluation
- TcsDocument51 pagesTcsnivitha90Pas encore d'évaluation
- Noor Zuliana BT Mohd FuziDocument6 pagesNoor Zuliana BT Mohd FuziPPA JakartaPas encore d'évaluation