Vous aimerez peut-être aussi
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeD'EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeÉvaluation : 4 sur 5 étoiles4/5 (5794)
- Shoe Dog: A Memoir by the Creator of NikeD'EverandShoe Dog: A Memoir by the Creator of NikeÉvaluation : 4.5 sur 5 étoiles4.5/5 (537)
- Criterion A: Focus and MethodDocument7 pagesCriterion A: Focus and MethodShania SmithPas encore d'évaluation
- Tok-Essay-Work-Book-Courseleap-2019 (New)Document26 pagesTok-Essay-Work-Book-Courseleap-2019 (New)Shreya ChhabriaPas encore d'évaluation
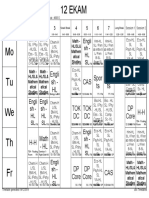
- TT Effective From 4th January 2020 - INSPIRUSDocument1 pageTT Effective From 4th January 2020 - INSPIRUSShreya ChhabriaPas encore d'évaluation
- 3.1 GenesDocument1 page3.1 GenesShreya ChhabriaPas encore d'évaluation
- Ia Checklist PDFDocument1 pageIa Checklist PDFRayya Shahwar HussainPas encore d'évaluation
- 5.4 Cladistics PDFDocument1 page5.4 Cladistics PDFShreya ChhabriaPas encore d'évaluation
- Why I Write: Vers D'occasion, Semi-Comic PoemsDocument4 pagesWhy I Write: Vers D'occasion, Semi-Comic PoemsShreya ChhabriaPas encore d'évaluation
- Chlorophyll in Olive OilDocument5 pagesChlorophyll in Olive OilShreya ChhabriaPas encore d'évaluation
- Biases, Fallacies, ArgumentDocument3 pagesBiases, Fallacies, ArgumentShreya ChhabriaPas encore d'évaluation
- Figaro Olive OilDocument4 pagesFigaro Olive OilShreya Chhabria0% (1)
- 3Document7 pages3Shreya ChhabriaPas encore d'évaluation
- Plant Phyla: BryophytaDocument5 pagesPlant Phyla: BryophytaShreya ChhabriaPas encore d'évaluation
- A Nice Cup of TeaDocument2 pagesA Nice Cup of TeaShreya ChhabriaPas encore d'évaluation
- Plant Phyla: BryophytaDocument5 pagesPlant Phyla: BryophytaShreya ChhabriaPas encore d'évaluation
- Vertebrate ClassesDocument3 pagesVertebrate ClassesShreya ChhabriaPas encore d'évaluation
- Vertebrate ClassesDocument3 pagesVertebrate ClassesShreya ChhabriaPas encore d'évaluation
- The Yellow House: A Memoir (2019 National Book Award Winner)D'EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Évaluation : 4 sur 5 étoiles4/5 (98)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceD'EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceÉvaluation : 4 sur 5 étoiles4/5 (895)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersD'EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersÉvaluation : 4.5 sur 5 étoiles4.5/5 (344)
- The Little Book of Hygge: Danish Secrets to Happy LivingD'EverandThe Little Book of Hygge: Danish Secrets to Happy LivingÉvaluation : 3.5 sur 5 étoiles3.5/5 (399)
- Grit: The Power of Passion and PerseveranceD'EverandGrit: The Power of Passion and PerseveranceÉvaluation : 4 sur 5 étoiles4/5 (588)
- The Emperor of All Maladies: A Biography of CancerD'EverandThe Emperor of All Maladies: A Biography of CancerÉvaluation : 4.5 sur 5 étoiles4.5/5 (271)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaD'EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaÉvaluation : 4.5 sur 5 étoiles4.5/5 (266)
- Never Split the Difference: Negotiating As If Your Life Depended On ItD'EverandNever Split the Difference: Negotiating As If Your Life Depended On ItÉvaluation : 4.5 sur 5 étoiles4.5/5 (838)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryD'EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryÉvaluation : 3.5 sur 5 étoiles3.5/5 (231)
- On Fire: The (Burning) Case for a Green New DealD'EverandOn Fire: The (Burning) Case for a Green New DealÉvaluation : 4 sur 5 étoiles4/5 (73)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureD'EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureÉvaluation : 4.5 sur 5 étoiles4.5/5 (474)
- Team of Rivals: The Political Genius of Abraham LincolnD'EverandTeam of Rivals: The Political Genius of Abraham LincolnÉvaluation : 4.5 sur 5 étoiles4.5/5 (234)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyD'EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyÉvaluation : 3.5 sur 5 étoiles3.5/5 (2259)
- The Unwinding: An Inner History of the New AmericaD'EverandThe Unwinding: An Inner History of the New AmericaÉvaluation : 4 sur 5 étoiles4/5 (45)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreD'EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreÉvaluation : 4 sur 5 étoiles4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)D'EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Évaluation : 4.5 sur 5 étoiles4.5/5 (121)
- Her Body and Other Parties: StoriesD'EverandHer Body and Other Parties: StoriesÉvaluation : 4 sur 5 étoiles4/5 (821)
- Morphology & Syntax "Morpheme Forms": Page - 1Document10 pagesMorphology & Syntax "Morpheme Forms": Page - 1محمد ناصر عليويPas encore d'évaluation
- Managing New VenturesDocument1 pageManaging New VenturesPrateek RaoPas encore d'évaluation
- Management Decision Case: Restoration HardwaDocument3 pagesManagement Decision Case: Restoration HardwaRishha Devi Ravindran100% (5)
- The Last LeafDocument42 pagesThe Last LeafNguyen LePas encore d'évaluation
- Community-Based Health Planning Services: Topic OneDocument28 pagesCommunity-Based Health Planning Services: Topic OneHigh TechPas encore d'évaluation
- Par Vol2i10Document66 pagesPar Vol2i10Bakhita MaryamPas encore d'évaluation
- Unilever IFE EFE CPM MatrixDocument7 pagesUnilever IFE EFE CPM MatrixNabeel Raja73% (11)
- BPHC HRSA-23-025 (H8H) FY 2023 Ending HIV Epidemic - FinalDocument44 pagesBPHC HRSA-23-025 (H8H) FY 2023 Ending HIV Epidemic - FinalTuhin DeyPas encore d'évaluation
- Chapter 3. Different Kinds of ObligationDocument17 pagesChapter 3. Different Kinds of ObligationTASNIM MUSAPas encore d'évaluation
- Industry ProfileDocument16 pagesIndustry Profileactive1cafePas encore d'évaluation
- Transformation of Green Areas in Urban Landscape of Lucknow: Need For Holistic Intervention With Respect To River GomtiDocument10 pagesTransformation of Green Areas in Urban Landscape of Lucknow: Need For Holistic Intervention With Respect To River GomtiASHUTOSH SINGHPas encore d'évaluation
- CCOB 021 and CCOC 021 Module Outline For 2022Document5 pagesCCOB 021 and CCOC 021 Module Outline For 2022Matodzi ArehonePas encore d'évaluation
- 08 - Case Law-Unknown Case Law ListDocument28 pages08 - Case Law-Unknown Case Law ListNausheen100% (1)
- Color Code Look For Complied With ECE Look For With Partial Compliance, ECE Substitute Presented Look For Not CompliedDocument2 pagesColor Code Look For Complied With ECE Look For With Partial Compliance, ECE Substitute Presented Look For Not CompliedMelanie Nina ClaretePas encore d'évaluation
- Bharat Prachin Eanv Aadhunik Shiksha Pranali: Ek Gahan AdhyayanDocument6 pagesBharat Prachin Eanv Aadhunik Shiksha Pranali: Ek Gahan AdhyayanAnonymous CwJeBCAXpPas encore d'évaluation
- SLRC InstPage Paper IIIDocument5 pagesSLRC InstPage Paper IIIgoviPas encore d'évaluation
- Cosmetics & Toiletries Market Overviews 2015Document108 pagesCosmetics & Toiletries Market Overviews 2015babidqn100% (1)
- Apple Case ReportDocument2 pagesApple Case ReportAwa SannoPas encore d'évaluation
- Midterm ExamDocument3 pagesMidterm ExamRafael CensonPas encore d'évaluation
- Company Loan PolicyDocument2 pagesCompany Loan PolicyKaleem60% (5)
- ĐỀ SỐ 6 - KEYDocument6 pagesĐỀ SỐ 6 - KEYAnh MaiPas encore d'évaluation
- Luovutuskirja Ajoneuvon Vesikulkuneuvon Omistusoikeuden Siirrosta B124eDocument2 pagesLuovutuskirja Ajoneuvon Vesikulkuneuvon Omistusoikeuden Siirrosta B124eAirsoftPas encore d'évaluation
- Tallado V. ComelecDocument3 pagesTallado V. ComelecLorelain ImperialPas encore d'évaluation
- NMML Occasional Paper: The Anticolonial Ethics of Lala Har Dayal'sDocument22 pagesNMML Occasional Paper: The Anticolonial Ethics of Lala Har Dayal'sСаша ПаповићPas encore d'évaluation
- Business Requirement Document HR Portal 1.0Document16 pagesBusiness Requirement Document HR Portal 1.0Usman TariqPas encore d'évaluation
- Ultima Underworld II - A Safe Passage Through Britannia PDFDocument28 pagesUltima Underworld II - A Safe Passage Through Britannia PDFEdgar Sánchez FuentesPas encore d'évaluation
- Marathi 3218Document11 pagesMarathi 3218Nuvishta RammaPas encore d'évaluation
- District Memo 2021 PPST PPSSHDocument2 pagesDistrict Memo 2021 PPST PPSSHRosalie MarquezPas encore d'évaluation
- The Six Day War: Astoneshing Warfear?Document3 pagesThe Six Day War: Astoneshing Warfear?Ruben MunteanuPas encore d'évaluation
- Mẫu Kế Hoạch Digital Marketing File ExcelDocument14 pagesMẫu Kế Hoạch Digital Marketing File ExcelTrangPas encore d'évaluation