Vous aimerez peut-être aussi
- Shoe Dog: A Memoir by the Creator of NikeD'EverandShoe Dog: A Memoir by the Creator of NikeÉvaluation : 4.5 sur 5 étoiles4.5/5 (537)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeD'EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeÉvaluation : 4 sur 5 étoiles4/5 (5794)
- Congenital Heart Defects Test Five Nursing FourDocument6 pagesCongenital Heart Defects Test Five Nursing FourTiffany D'Alessandro GordonPas encore d'évaluation
- Bariatric DrugsDocument3 pagesBariatric DrugsTiffany D'Alessandro Gordon100% (1)
- 8/24/2010 Lecture Condensed To 3 PagesDocument3 pages8/24/2010 Lecture Condensed To 3 PagesTiffany D'Alessandro GordonPas encore d'évaluation
- Everything I Have Highlighted From 8/24/10 LecturesDocument1 pageEverything I Have Highlighted From 8/24/10 LecturesTiffany D'Alessandro GordonPas encore d'évaluation
- Nursing Exam Test V Crisis InterventionDocument3 pagesNursing Exam Test V Crisis InterventionTiffany D'Alessandro GordonPas encore d'évaluation
- Nursing Exam Questions Practice Test VDocument6 pagesNursing Exam Questions Practice Test VTiffany D'Alessandro Gordon94% (18)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceD'EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceÉvaluation : 4 sur 5 étoiles4/5 (895)
- The Yellow House: A Memoir (2019 National Book Award Winner)D'EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Évaluation : 4 sur 5 étoiles4/5 (98)
- Grit: The Power of Passion and PerseveranceD'EverandGrit: The Power of Passion and PerseveranceÉvaluation : 4 sur 5 étoiles4/5 (588)
- The Little Book of Hygge: Danish Secrets to Happy LivingD'EverandThe Little Book of Hygge: Danish Secrets to Happy LivingÉvaluation : 3.5 sur 5 étoiles3.5/5 (400)
- The Emperor of All Maladies: A Biography of CancerD'EverandThe Emperor of All Maladies: A Biography of CancerÉvaluation : 4.5 sur 5 étoiles4.5/5 (271)
- Never Split the Difference: Negotiating As If Your Life Depended On ItD'EverandNever Split the Difference: Negotiating As If Your Life Depended On ItÉvaluation : 4.5 sur 5 étoiles4.5/5 (838)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyD'EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyÉvaluation : 3.5 sur 5 étoiles3.5/5 (2259)
- On Fire: The (Burning) Case for a Green New DealD'EverandOn Fire: The (Burning) Case for a Green New DealÉvaluation : 4 sur 5 étoiles4/5 (74)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureD'EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureÉvaluation : 4.5 sur 5 étoiles4.5/5 (474)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryD'EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryÉvaluation : 3.5 sur 5 étoiles3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnD'EverandTeam of Rivals: The Political Genius of Abraham LincolnÉvaluation : 4.5 sur 5 étoiles4.5/5 (234)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaD'EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaÉvaluation : 4.5 sur 5 étoiles4.5/5 (266)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersD'EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersÉvaluation : 4.5 sur 5 étoiles4.5/5 (345)
- The Unwinding: An Inner History of the New AmericaD'EverandThe Unwinding: An Inner History of the New AmericaÉvaluation : 4 sur 5 étoiles4/5 (45)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreD'EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreÉvaluation : 4 sur 5 étoiles4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)D'EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Évaluation : 4.5 sur 5 étoiles4.5/5 (121)
- Her Body and Other Parties: StoriesD'EverandHer Body and Other Parties: StoriesÉvaluation : 4 sur 5 étoiles4/5 (821)
- EEG ReportDocument2 pagesEEG ReportxiakenliangPas encore d'évaluation
- Referat Letak SungsangDocument13 pagesReferat Letak SungsangIsma Resti PratiwiPas encore d'évaluation
- Yoga at Your DeskDocument8 pagesYoga at Your DeskGuruprashanth Rao100% (2)
- Clinical Biomechanics - Body Alignment, Posture, and GaitDocument53 pagesClinical Biomechanics - Body Alignment, Posture, and Gaitmihaela_moldova91280% (1)
- Murphy Homeopathi Clinical Repertory PrefaceDocument5 pagesMurphy Homeopathi Clinical Repertory PrefaceKrishna25% (4)
- Hunter Education HandbookDocument210 pagesHunter Education HandbookJuan Francisco Lecay Alegre100% (1)
- Trauma: Clinical Practice Guidelines - TraumaDocument41 pagesTrauma: Clinical Practice Guidelines - TraumamuhamadmukhlisPas encore d'évaluation
- Water Seal Chest DrainageDocument5 pagesWater Seal Chest DrainageAmadelle FaithPas encore d'évaluation
- Sample Case StudyDocument38 pagesSample Case Studyanon-387573100% (3)
- ISSN 2347-2375: Conceptual Study On ShoshaDocument7 pagesISSN 2347-2375: Conceptual Study On ShosharakeshPas encore d'évaluation
- Enumeration of Human Body Parts According To AyurvedaDocument13 pagesEnumeration of Human Body Parts According To AyurvedaKrishna Venkat VPas encore d'évaluation
- Notes On Anatomy and Physiology For Yoga PDFDocument195 pagesNotes On Anatomy and Physiology For Yoga PDFPetar MogilskiPas encore d'évaluation
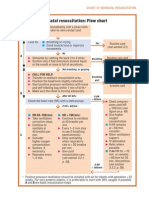
- Neonatal Resuscitation Program Flow ChartDocument3 pagesNeonatal Resuscitation Program Flow ChartChin Nam80% (5)
- Relationship Between Chapman's Reflexes and Acupuncture Meridians by Traditional Chinese Medicine Practitioners in TaiwanDocument22 pagesRelationship Between Chapman's Reflexes and Acupuncture Meridians by Traditional Chinese Medicine Practitioners in TaiwanFrederic Dubois100% (2)
- How To Sing (Meine Gesangskunst) by Lehmann, Lilli, 1848-1929Document88 pagesHow To Sing (Meine Gesangskunst) by Lehmann, Lilli, 1848-1929Gutenberg.org100% (2)
- Breathing TechniquesDocument26 pagesBreathing TechniquessherryPas encore d'évaluation
- Pediatric Chest PhysiotherapyDocument25 pagesPediatric Chest PhysiotherapyShubha DiwakarPas encore d'évaluation
- Flashcards About Medical DefinitionsDocument62 pagesFlashcards About Medical DefinitionsSrikanth PagidiPas encore d'évaluation
- Sternotomi PDFDocument11 pagesSternotomi PDFHeri PrasetyoPas encore d'évaluation
- Criminal Law CasesDocument253 pagesCriminal Law CasesMuli MJPas encore d'évaluation
- Chest PBLDocument2 pagesChest PBLRamish IrfanPas encore d'évaluation
- 1907 Towne Just How To Wake Solar PlexusDocument29 pages1907 Towne Just How To Wake Solar PlexusAlcibiades TeixeiraPas encore d'évaluation
- Illustrated Guide To The Homoeopathic Treatment Harbaris Singh Khaneja.01169 3chestDocument7 pagesIllustrated Guide To The Homoeopathic Treatment Harbaris Singh Khaneja.01169 3chestMarija VelkoskiPas encore d'évaluation
- Nursing Flash CardsDocument5 pagesNursing Flash CardsJan Clarisse RamosPas encore d'évaluation
- Gil Boyne Method of Conditioning TJDocument3 pagesGil Boyne Method of Conditioning TJsshhmmuueell100% (1)
- MRCS Part-A January 2019 RECALL PDFDocument4 pagesMRCS Part-A January 2019 RECALL PDFRajib Pal ChowdhuryPas encore d'évaluation
- Test Bank For Essentials of Medical Language 4th Edition David Allan Rachel BascoDocument61 pagesTest Bank For Essentials of Medical Language 4th Edition David Allan Rachel BascopandoraissacziaePas encore d'évaluation
- Introduction Secrets of SingingDocument26 pagesIntroduction Secrets of SingingAdrian Barilà100% (3)
- Performance Checklist (Pa)Document3 pagesPerformance Checklist (Pa)Kaye Castellano100% (1)
- Compliance and ResistanceDocument5 pagesCompliance and ResistanceNissie DegulacionPas encore d'évaluation