Vous aimerez peut-être aussi
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeD'EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeÉvaluation : 4 sur 5 étoiles4/5 (5794)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreD'EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreÉvaluation : 4 sur 5 étoiles4/5 (1090)
- Never Split the Difference: Negotiating As If Your Life Depended On ItD'EverandNever Split the Difference: Negotiating As If Your Life Depended On ItÉvaluation : 4.5 sur 5 étoiles4.5/5 (838)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceD'EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceÉvaluation : 4 sur 5 étoiles4/5 (894)
- Grit: The Power of Passion and PerseveranceD'EverandGrit: The Power of Passion and PerseveranceÉvaluation : 4 sur 5 étoiles4/5 (587)
- Shoe Dog: A Memoir by the Creator of NikeD'EverandShoe Dog: A Memoir by the Creator of NikeÉvaluation : 4.5 sur 5 étoiles4.5/5 (537)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureD'EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureÉvaluation : 4.5 sur 5 étoiles4.5/5 (474)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersD'EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersÉvaluation : 4.5 sur 5 étoiles4.5/5 (344)
- Her Body and Other Parties: StoriesD'EverandHer Body and Other Parties: StoriesÉvaluation : 4 sur 5 étoiles4/5 (821)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)D'EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Évaluation : 4.5 sur 5 étoiles4.5/5 (119)
- The Emperor of All Maladies: A Biography of CancerD'EverandThe Emperor of All Maladies: A Biography of CancerÉvaluation : 4.5 sur 5 étoiles4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingD'EverandThe Little Book of Hygge: Danish Secrets to Happy LivingÉvaluation : 3.5 sur 5 étoiles3.5/5 (399)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyD'EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyÉvaluation : 3.5 sur 5 étoiles3.5/5 (2219)
- The Yellow House: A Memoir (2019 National Book Award Winner)D'EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Évaluation : 4 sur 5 étoiles4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaD'EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaÉvaluation : 4.5 sur 5 étoiles4.5/5 (265)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryD'EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryÉvaluation : 3.5 sur 5 étoiles3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnD'EverandTeam of Rivals: The Political Genius of Abraham LincolnÉvaluation : 4.5 sur 5 étoiles4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealD'EverandOn Fire: The (Burning) Case for a Green New DealÉvaluation : 4 sur 5 étoiles4/5 (73)
- The Unwinding: An Inner History of the New AmericaD'EverandThe Unwinding: An Inner History of the New AmericaÉvaluation : 4 sur 5 étoiles4/5 (45)
- Vi Crimes Against Public MoralsDocument25 pagesVi Crimes Against Public MoralsDennis Aran Tupaz AbrilPas encore d'évaluation
- Chastity Rape ComparisonDocument2 pagesChastity Rape ComparisonDennis Aran Tupaz AbrilPas encore d'évaluation
- Transportation Law UpdatesDocument83 pagesTransportation Law UpdatesDennis Aran Tupaz AbrilPas encore d'évaluation
- NOTES ON SUCCESSION KEY TERMS AND CONCEPTSDocument26 pagesNOTES ON SUCCESSION KEY TERMS AND CONCEPTSDennis Aran Tupaz Abril100% (1)
- Southwest Africa To ReyesDocument29 pagesSouthwest Africa To ReyesDennis Aran Tupaz AbrilPas encore d'évaluation
- Agency CasesDocument113 pagesAgency CasesDennis Aran Tupaz AbrilPas encore d'évaluation
- Parties Facts Issue/S SC Ruling Province of Abra: Digested Tax Cases Part Iii Dennisaranabriljdii 1Document19 pagesParties Facts Issue/S SC Ruling Province of Abra: Digested Tax Cases Part Iii Dennisaranabriljdii 1Dennis Aran Tupaz AbrilPas encore d'évaluation
- The Qualifieds in Criminal LawDocument2 pagesThe Qualifieds in Criminal LawDennis Aran Tupaz AbrilPas encore d'évaluation
- Complaint 3A Delcastillo AbrilDocument7 pagesComplaint 3A Delcastillo AbrilDennis Aran Tupaz AbrilPas encore d'évaluation
- Cir V. Pilipinas Shell Petroleum Facts:: Exemption Provided in Sec. 135 Attaches To The PetroleumDocument5 pagesCir V. Pilipinas Shell Petroleum Facts:: Exemption Provided in Sec. 135 Attaches To The PetroleumDennis Aran Tupaz AbrilPas encore d'évaluation
- Conflict CasesDocument13 pagesConflict CasesDennis Aran Tupaz AbrilPas encore d'évaluation
- Rabadilla Vs CA SuccessionDocument16 pagesRabadilla Vs CA SuccessionDennis Aran Tupaz AbrilPas encore d'évaluation
- Oca (Sca (: Special Civil Actions Introductory ConceptsDocument1 pageOca (Sca (: Special Civil Actions Introductory ConceptsDennis Aran Tupaz AbrilPas encore d'évaluation
- Procedures for Original Cases and Appeals in the Supreme CourtDocument23 pagesProcedures for Original Cases and Appeals in the Supreme CourtDennis Aran Tupaz AbrilPas encore d'évaluation
- Rule 66Document2 pagesRule 66Dennis Aran Tupaz AbrilPas encore d'évaluation
- Special Civil Actions Expropriation Proceedings ExplainedDocument2 pagesSpecial Civil Actions Expropriation Proceedings ExplainedDennis Aran Tupaz AbrilPas encore d'évaluation
- Provisional Remedies Support Pendente LiteDocument2 pagesProvisional Remedies Support Pendente LiteDennis Aran Tupaz AbrilPas encore d'évaluation
- Oca (Sca (: Special Civil Actions Introductory ConceptsDocument9 pagesOca (Sca (: Special Civil Actions Introductory ConceptsDennis Aran Tupaz AbrilPas encore d'évaluation
- Rule 58Document7 pagesRule 58Dennis Aran Tupaz AbrilPas encore d'évaluation
- Rule 57Document6 pagesRule 57Dennis Aran Tupaz AbrilPas encore d'évaluation
- ESTATE TAX NOTESDocument6 pagesESTATE TAX NOTESDennis Aran Tupaz AbrilPas encore d'évaluation
- Quickie Notes EvidenceDocument9 pagesQuickie Notes EvidenceDennis Aran Tupaz AbrilPas encore d'évaluation
- Special Complex CrimesDocument7 pagesSpecial Complex CrimesDennis Aran Tupaz AbrilPas encore d'évaluation
- Lawyer's Role in SocietyDocument14 pagesLawyer's Role in SocietyDennis Aran Tupaz AbrilPas encore d'évaluation
- Labor Finals MatrixDocument24 pagesLabor Finals MatrixDennis Aran Tupaz Abril100% (1)
- 2019 Bar Examinations Civil Law SyllabusDocument4 pages2019 Bar Examinations Civil Law SyllabusclarizzzPas encore d'évaluation
- Nil Quickie NotesDocument8 pagesNil Quickie NotesDennis Aran Tupaz AbrilPas encore d'évaluation
- Criminal Law I MatricesDocument9 pagesCriminal Law I MatricesDennis Aran Tupaz AbrilPas encore d'évaluation
- Quorum Voting Constitutional LawDocument2 pagesQuorum Voting Constitutional LawDennis AbrilPas encore d'évaluation
- Intellectual Property LawDocument34 pagesIntellectual Property LawDennis Aran Tupaz AbrilPas encore d'évaluation
- Notable Pandemics in HistoryDocument2 pagesNotable Pandemics in Historyapi-264004571Pas encore d'évaluation
- CDC - Overuse of Antibiotics Is Killing AmericansDocument4 pagesCDC - Overuse of Antibiotics Is Killing AmericansjohntandraPas encore d'évaluation
- Alopecia 203Document14 pagesAlopecia 203api-535005469Pas encore d'évaluation
- Multiple SclerosisDocument96 pagesMultiple SclerosisDrGasnasPas encore d'évaluation
- Transfusion Support of Autoimmune Hemolytic AnemiaDocument7 pagesTransfusion Support of Autoimmune Hemolytic AnemiaMohamed ElmasryPas encore d'évaluation
- Slide Test For Anti - Streptolysin O (Latex Agglutination Test)Document2 pagesSlide Test For Anti - Streptolysin O (Latex Agglutination Test)Dinesh SreedharanPas encore d'évaluation
- Rntcp-Revised National Tuberculosis Control ProgrammeDocument29 pagesRntcp-Revised National Tuberculosis Control ProgrammedranshulitrivediPas encore d'évaluation
- MC Great Lakes SlidesDocument26 pagesMC Great Lakes Slidesapi-666654042Pas encore d'évaluation
- Gana Tra 2010Document10 pagesGana Tra 2010Shofi Dhia AiniPas encore d'évaluation
- Immunology NotesDocument58 pagesImmunology Notespawnjabi100% (1)
- Istar 500 Drawray Catalog PDFDocument2 pagesIstar 500 Drawray Catalog PDFCV Langgeng Jaya Bojonegoro50% (2)
- Toll-Like Receptors Role in Periodontal Health and DiseaseDocument15 pagesToll-Like Receptors Role in Periodontal Health and DiseaseAdyas AdrianaPas encore d'évaluation
- Introduction To BiotechnologyDocument335 pagesIntroduction To BiotechnologySamson TizazuPas encore d'évaluation
- Malaria Managment Algorithm 202208Document1 pageMalaria Managment Algorithm 202208Marianne Joy PontigonPas encore d'évaluation
- Block 1 (40) Infectious Diseases As-CompressedDocument173 pagesBlock 1 (40) Infectious Diseases As-CompressedanweridrisejazPas encore d'évaluation
- National Rabies Control Programme GuidelineDocument7 pagesNational Rabies Control Programme GuidelineHari Pawan Kishore GarimellaPas encore d'évaluation
- Chapter 3 Infection Control: Phlebotomy, 5e (Booth)Document13 pagesChapter 3 Infection Control: Phlebotomy, 5e (Booth)Carol Reed100% (1)
- Tocilizumab Drug Monograph - 1JUN2020Document43 pagesTocilizumab Drug Monograph - 1JUN2020juanferrePas encore d'évaluation
- M-M-R Ii: Swollen GlandsDocument9 pagesM-M-R Ii: Swollen GlandsJoanne Alyssa Hernandez LascanoPas encore d'évaluation
- Covid Vaccine CertificateDocument1 pageCovid Vaccine CertificateShiva ShivaPas encore d'évaluation
- CBC Test Results and InterpretationDocument9 pagesCBC Test Results and InterpretationamiosaPas encore d'évaluation
- BT102-Microbiology Current Paper Solved Question Final Term February 2020Document11 pagesBT102-Microbiology Current Paper Solved Question Final Term February 2020Awais Bhutta100% (1)
- IIP2015 IntroductionDocument6 pagesIIP2015 Introductionjanaka100% (1)
- Pertussis (Whooping Cough) : University of BuroaDocument42 pagesPertussis (Whooping Cough) : University of BuroaMumin Alamin AllaminPas encore d'évaluation
- Inflammatory Bowel Disease WardDocument103 pagesInflammatory Bowel Disease WardAsad Khan KhalilPas encore d'évaluation
- Betamethasone Oral Drops for Registered Medical PractitionersDocument8 pagesBetamethasone Oral Drops for Registered Medical PractitionersAnamika VatsalPas encore d'évaluation
- Care, Compassion, Excellence Mount Lockyer Primary School A Place To Learn and GrowDocument4 pagesCare, Compassion, Excellence Mount Lockyer Primary School A Place To Learn and GrowMountLockyerPas encore d'évaluation
- Module 4 Immediate Kidney Transplant Care 1 1Document1 pageModule 4 Immediate Kidney Transplant Care 1 1fouad tabetPas encore d'évaluation
- Presentation CovidDocument2 pagesPresentation CovidYungfuPas encore d'évaluation
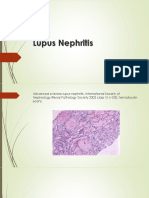
- Lupus Nephritis: Diagnosis and ManagementDocument38 pagesLupus Nephritis: Diagnosis and ManagementTristan EugenePas encore d'évaluation