Vous aimerez peut-être aussi
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeD'EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeÉvaluation : 4 sur 5 étoiles4/5 (5794)
- Shoe Dog: A Memoir by the Creator of NikeD'EverandShoe Dog: A Memoir by the Creator of NikeÉvaluation : 4.5 sur 5 étoiles4.5/5 (537)
- The Yellow House: A Memoir (2019 National Book Award Winner)D'EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Évaluation : 4 sur 5 étoiles4/5 (98)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceD'EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceÉvaluation : 4 sur 5 étoiles4/5 (895)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersD'EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersÉvaluation : 4.5 sur 5 étoiles4.5/5 (344)
- The Little Book of Hygge: Danish Secrets to Happy LivingD'EverandThe Little Book of Hygge: Danish Secrets to Happy LivingÉvaluation : 3.5 sur 5 étoiles3.5/5 (399)
- Grit: The Power of Passion and PerseveranceD'EverandGrit: The Power of Passion and PerseveranceÉvaluation : 4 sur 5 étoiles4/5 (588)
- The Emperor of All Maladies: A Biography of CancerD'EverandThe Emperor of All Maladies: A Biography of CancerÉvaluation : 4.5 sur 5 étoiles4.5/5 (271)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaD'EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaÉvaluation : 4.5 sur 5 étoiles4.5/5 (266)
- Never Split the Difference: Negotiating As If Your Life Depended On ItD'EverandNever Split the Difference: Negotiating As If Your Life Depended On ItÉvaluation : 4.5 sur 5 étoiles4.5/5 (838)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryD'EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryÉvaluation : 3.5 sur 5 étoiles3.5/5 (231)
- On Fire: The (Burning) Case for a Green New DealD'EverandOn Fire: The (Burning) Case for a Green New DealÉvaluation : 4 sur 5 étoiles4/5 (73)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureD'EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureÉvaluation : 4.5 sur 5 étoiles4.5/5 (474)
- Team of Rivals: The Political Genius of Abraham LincolnD'EverandTeam of Rivals: The Political Genius of Abraham LincolnÉvaluation : 4.5 sur 5 étoiles4.5/5 (234)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyD'EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyÉvaluation : 3.5 sur 5 étoiles3.5/5 (2259)
- The Unwinding: An Inner History of the New AmericaD'EverandThe Unwinding: An Inner History of the New AmericaÉvaluation : 4 sur 5 étoiles4/5 (45)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreD'EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreÉvaluation : 4 sur 5 étoiles4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)D'EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Évaluation : 4.5 sur 5 étoiles4.5/5 (120)
- Her Body and Other Parties: StoriesD'EverandHer Body and Other Parties: StoriesÉvaluation : 4 sur 5 étoiles4/5 (821)
- Endocrine GlandDocument10 pagesEndocrine GlandRS100% (1)
- Pharmacology AssignmentDocument6 pagesPharmacology AssignmentMaria MushtaquePas encore d'évaluation
- Feline Occult Hyperthyroidism: Consultant On CallDocument3 pagesFeline Occult Hyperthyroidism: Consultant On CallNguyễn Tấn TàiPas encore d'évaluation
- Index Index: SMN1 Mutation, 546Document9 pagesIndex Index: SMN1 Mutation, 546Luis Jose VelazquezPas encore d'évaluation
- Graves Disease - StatPearls - NCBI BookshelfDocument8 pagesGraves Disease - StatPearls - NCBI BookshelfDr.Pradip PatilPas encore d'évaluation
- Casos EndocrinoDocument72 pagesCasos EndocrinoAlfredo JaureguiPas encore d'évaluation
- Pharmacology of The Endocrine SystemDocument74 pagesPharmacology of The Endocrine SystemarpanabiswassshetyePas encore d'évaluation
- Graves' Disease: Bella I. Putri 16-025Document29 pagesGraves' Disease: Bella I. Putri 16-025anon_414347743Pas encore d'évaluation
- Simranpreet KaurDocument10 pagesSimranpreet KaurSimranpreet KaurPas encore d'évaluation
- Thyroid Gland: Pactical Activity No. 5Document19 pagesThyroid Gland: Pactical Activity No. 5Damian CorinaPas encore d'évaluation
- Thyroid CrisisDocument17 pagesThyroid CrisisFebriliana Mao-maoPas encore d'évaluation
- Endocrine Tess 1-7Document41 pagesEndocrine Tess 1-7필리우크Pas encore d'évaluation
- PuerperiumDocument85 pagesPuerperiumHema MaliniPas encore d'évaluation
- Thyroid DisordersDocument5 pagesThyroid DisordersAnggunNMPas encore d'évaluation
- Cases Studies in Clinical Pharmacy - Final - 2018Document7 pagesCases Studies in Clinical Pharmacy - Final - 2018Abood NamerPas encore d'évaluation
- Papillary Thyroid CarcinomaDocument42 pagesPapillary Thyroid CarcinomaHerman ZoletaPas encore d'évaluation
- NUR 300 - Final Exam Study Guide - 2016Document548 pagesNUR 300 - Final Exam Study Guide - 2016MSU_nursing_4_lifePas encore d'évaluation
- Drugs Used in Disorders of Endocrine System Ppt. Book (Lectures 1-6)Document467 pagesDrugs Used in Disorders of Endocrine System Ppt. Book (Lectures 1-6)Marc Imhotep Cray, M.D.100% (1)
- Benign Diseases of ThyroidDocument70 pagesBenign Diseases of ThyroidMounica MekalaPas encore d'évaluation
- Thyroid Eye DiseaseDocument32 pagesThyroid Eye Disease-Yohanes Firmansyah-Pas encore d'évaluation
- (Pha) Le 5Document19 pages(Pha) Le 5Gabby TanPas encore d'évaluation
- Hormonal ChangesDocument6 pagesHormonal Changesvin DVCPas encore d'évaluation
- Overview of Thyroiditis - UpToDateDocument7 pagesOverview of Thyroiditis - UpToDateCamila NogueiraPas encore d'évaluation
- EndoquestionssolvedDocument14 pagesEndoquestionssolvedPuteri Nursyamimi Mohd SabilanPas encore d'évaluation
- Disorders of Endocrine SystemDocument48 pagesDisorders of Endocrine SystemSHARIM ASGHARPas encore d'évaluation
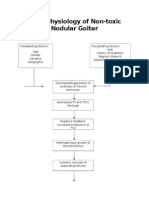
- Pathophysiology of Nontoxic Nodular GoiterDocument2 pagesPathophysiology of Nontoxic Nodular GoiterJan Jewey80% (10)
- Hypokalemic Paralysis PDFDocument7 pagesHypokalemic Paralysis PDFFanny SimaPas encore d'évaluation
- Jurnal Grave DiseaseDocument10 pagesJurnal Grave DiseasePutri Alfira ElfPas encore d'évaluation
- THYROID YunitaDocument81 pagesTHYROID YunitaPandu KusumawardhanyPas encore d'évaluation
- NCLEX Study GuideDocument38 pagesNCLEX Study GuideBEN GPas encore d'évaluation