Vous aimerez peut-être aussi
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeD'EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeÉvaluation : 4 sur 5 étoiles4/5 (5794)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreD'EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreÉvaluation : 4 sur 5 étoiles4/5 (1090)
- Never Split the Difference: Negotiating As If Your Life Depended On ItD'EverandNever Split the Difference: Negotiating As If Your Life Depended On ItÉvaluation : 4.5 sur 5 étoiles4.5/5 (838)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceD'EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceÉvaluation : 4 sur 5 étoiles4/5 (895)
- Grit: The Power of Passion and PerseveranceD'EverandGrit: The Power of Passion and PerseveranceÉvaluation : 4 sur 5 étoiles4/5 (588)
- Shoe Dog: A Memoir by the Creator of NikeD'EverandShoe Dog: A Memoir by the Creator of NikeÉvaluation : 4.5 sur 5 étoiles4.5/5 (537)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersD'EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersÉvaluation : 4.5 sur 5 étoiles4.5/5 (345)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureD'EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureÉvaluation : 4.5 sur 5 étoiles4.5/5 (474)
- Her Body and Other Parties: StoriesD'EverandHer Body and Other Parties: StoriesÉvaluation : 4 sur 5 étoiles4/5 (821)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)D'EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Évaluation : 4.5 sur 5 étoiles4.5/5 (121)
- The Emperor of All Maladies: A Biography of CancerD'EverandThe Emperor of All Maladies: A Biography of CancerÉvaluation : 4.5 sur 5 étoiles4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingD'EverandThe Little Book of Hygge: Danish Secrets to Happy LivingÉvaluation : 3.5 sur 5 étoiles3.5/5 (400)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyD'EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyÉvaluation : 3.5 sur 5 étoiles3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)D'EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Évaluation : 4 sur 5 étoiles4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaD'EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaÉvaluation : 4.5 sur 5 étoiles4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryD'EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryÉvaluation : 3.5 sur 5 étoiles3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnD'EverandTeam of Rivals: The Political Genius of Abraham LincolnÉvaluation : 4.5 sur 5 étoiles4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealD'EverandOn Fire: The (Burning) Case for a Green New DealÉvaluation : 4 sur 5 étoiles4/5 (74)
- The Unwinding: An Inner History of the New AmericaD'EverandThe Unwinding: An Inner History of the New AmericaÉvaluation : 4 sur 5 étoiles4/5 (45)
- GavareskiDocument7 pagesGavareskiMohamed MostafaPas encore d'évaluation
- Urodynamics (Aquick Pocket Guide)Document210 pagesUrodynamics (Aquick Pocket Guide)ZICO100% (2)
- Nursing Shift EndorsementDocument6 pagesNursing Shift Endorsementebrahim102099Pas encore d'évaluation
- MSBOS PrithvirajDocument8 pagesMSBOS Prithvirajkarun1889Pas encore d'évaluation
- Services: Hospital GasesDocument41 pagesServices: Hospital GasesRevati shinde100% (1)
- Advertisement KMTC 2019.2020. CleanedDocument2 pagesAdvertisement KMTC 2019.2020. CleanedMigori ArtPas encore d'évaluation
- Braxton Hicks or True Labor ContractionsDocument2 pagesBraxton Hicks or True Labor ContractionsJellyAnnGomezPas encore d'évaluation
- Part 1 MRCOG - SyllabusDocument6 pagesPart 1 MRCOG - SyllabusDr. Zaheer AliPas encore d'évaluation
- Pregnancy Polarity TherapyDocument3 pagesPregnancy Polarity TherapyJim FultonPas encore d'évaluation
- Advance Instruments For Laparoscopic SurgeryDocument7 pagesAdvance Instruments For Laparoscopic SurgeryAroelPas encore d'évaluation
- Pediatric Neuroanesthesia.3Document4 pagesPediatric Neuroanesthesia.3Mae Importers IncPas encore d'évaluation
- A Study of Patient Satisfaction Level in Out Patient Department (OPD) in A Tertiary Care Hospital in MaharashtraDocument9 pagesA Study of Patient Satisfaction Level in Out Patient Department (OPD) in A Tertiary Care Hospital in MaharashtraVital TejaPas encore d'évaluation
- Displacement of UtreusDocument13 pagesDisplacement of UtreusswethashakiPas encore d'évaluation
- PCOS DR BasimaDocument18 pagesPCOS DR BasimaA.H.APas encore d'évaluation
- Blood Storage Policy and ProcedureDocument3 pagesBlood Storage Policy and ProcedureMohamed AllamPas encore d'évaluation
- Retropubic SpaceDocument4 pagesRetropubic SpacesakuraleeshaoranPas encore d'évaluation
- OR AppendixDocument9 pagesOR AppendixDan HizonPas encore d'évaluation
- Health Family Welfare 3Document225 pagesHealth Family Welfare 3Gopala Sundararaj SPas encore d'évaluation
- VAC Diversified FlowDocument1 pageVAC Diversified FlowWinnie AtienoPas encore d'évaluation
- Colposcopy - UpToDateDocument25 pagesColposcopy - UpToDatemew2xxPas encore d'évaluation
- Relationship Between Maternal Haemoglobin and Fetal Weight: Rana SS, Sharma S, Chand A, Malla RDocument4 pagesRelationship Between Maternal Haemoglobin and Fetal Weight: Rana SS, Sharma S, Chand A, Malla RSatria UtamaPas encore d'évaluation
- Self Applied Topical Fluorides ClassDocument23 pagesSelf Applied Topical Fluorides ClassultraswamyPas encore d'évaluation
- Effects of High Dose Vitamin C Supplementation On Severe Covid19 Patients in The ICU - A Retrospective AnalysisDocument1 pageEffects of High Dose Vitamin C Supplementation On Severe Covid19 Patients in The ICU - A Retrospective AnalysiszipzoinkPas encore d'évaluation
- 1 - Overview of Maternal and Newborn Care - 08022014 - PHA RHMPP and NDPsDocument25 pages1 - Overview of Maternal and Newborn Care - 08022014 - PHA RHMPP and NDPsBoj OdejarPas encore d'évaluation
- 20140424040901417Document8 pages20140424040901417Anonymous h0DxuJTPas encore d'évaluation
- Abdominal Incisions: A Simple Guide For NursesDocument25 pagesAbdominal Incisions: A Simple Guide For Nursesfaris.surgeonPas encore d'évaluation
- Documentation of Nutritional Care ProcessDocument22 pagesDocumentation of Nutritional Care ProcessRojeil Mark Napudo MovillaPas encore d'évaluation
- Maternal & Child NursingDocument10 pagesMaternal & Child Nursingnokolip100% (2)
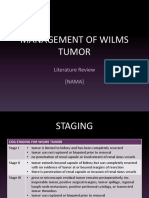
- Management of Wilms Tumor: Literature Review (NAMA)Document15 pagesManagement of Wilms Tumor: Literature Review (NAMA)DeaNataliaPas encore d'évaluation
- Self-Directed Learning (Nur 146 - Clinical Area)Document2 pagesSelf-Directed Learning (Nur 146 - Clinical Area)Dyan Bianca Suaso LastimosaPas encore d'évaluation