Académique Documents
Professionnel Documents
Culture Documents
Comparison of Gadolinium-Enhanced Fat-Saturated T1 - Weighted FLAIR and Fast Spin - Echo MRI of The Spine at 3 T For Evaluation of Extradural Lesions
Transféré par
anon_302681452Titre original
Copyright
Formats disponibles
Partager ce document
Partager ou intégrer le document
Avez-vous trouvé ce document utile ?
Ce contenu est-il inapproprié ?
Signaler ce documentDroits d'auteur :
Formats disponibles
Comparison of Gadolinium-Enhanced Fat-Saturated T1 - Weighted FLAIR and Fast Spin - Echo MRI of The Spine at 3 T For Evaluation of Extradural Lesions
Transféré par
anon_302681452Droits d'auteur :
Formats disponibles
Neuroradiolog y / Head and Neck Imaging • Original Research
Shah et al.
3-T T1-Weighted Imaging of Extradural Spinal Lesions
Neuroradiology/Head and Neck Imaging
Original Research
Comparison of Gadolinium-
Enhanced Fat-Saturated T1-
Downloaded from www.ajronline.org by 101.255.45.218 on 04/20/19 from IP address 101.255.45.218. Copyright ARRS. For personal use only; all rights reserved
Weighted FLAIR and Fast Spin-
Echo MRI of the Spine at 3 T for
Evaluation of Extradural Lesions
Komal B. Shah1 OBJECTIVE. Inversion recovery has been used to correct the loss of CSF and tissue contrast
Nandita Guha-Thakurta at 3 T versus 1.5 T but has not been formally investigated in the spine after IV administration of
Dawid Schellingerhout gadolinium-based contrast agent. The purpose of this study is to compare two sequences for gad-
John E. Madewell olinium-enhanced spine imaging at 3 T—fat-saturated T1-weighted FLAIR and fat-saturated T1-
Ashok J. Kumar weighted fast spin-echo (FSE)—for evaluation of extradural lesions and CSF-cord contrast.
MATERIALS AND METHODS. After IV administration of gadolinium-based con-
Colleen M. Costelloe
trast agent, fat-saturated T1-weighted FSE and FLAIR sequences were obtained in 156 MRI
Shah KB, Guha-Thakurta N, Schellingerhout D, scans of 143 patients at 3 T. Three experienced radiologists compared these sequences for
Madewell JE, Kumar AJ, Costelloe CM conspicuity differences in bone lesions, disk lesions, other epidural lesions, and cord-CSF
contrast. A 7-point visual rating scale was used, with lower numbers indicating increased
conspicuity on gadolinium-enhanced fat-saturated T1-weighted FLAIR and higher numbers
indicating increased conspicuity on gadolinium-enhanced fat-saturated T1-weighted FSE.
RESULTS. A slight increase in the conspicuity of gadolinium-enhancing bone lesions
(mean score, 3.6; p < 0.0001), disk lesions (mean score, 3.5; p < 0.0001), and epidural le-
sions (mean score, 3.4; p < 0.0001) was seen on fat-saturated T1-weighted FLAIR compared
with fat-saturated T1-weighted FSE. A higher degree of contrast between the spinal cord and
CSF was seen on fat-saturated T1-weighted FLAIR, by a large margin (mean score, 1.8; p <
0.0001). All enhancing lesions seen on fat-saturated T1-weighted FSE images were also seen
on fat-saturated T1-weighted FLAIR images.
CONCLUSION. Decreased CSF-cord contrast at 3 T, as seen on T1-weighted FSE, can be
regained by using T1-weighted FLAIR. Fat-saturated T1-weighted FLAIR may increase conspi-
cuity of gadolinium-enhancing extradural lesions compared with fat-saturated T1-weighted FSE.
O
ne of the advantages of high-field- liseconds and the time at 3 T was 993 ± 47
strength MRI is the potential to milliseconds. Rooney et al. [1] found that the
increase signal-to-noise ratios and, T1 relaxation time for intracranial CSF at 1.5
thus, image quality. The promise T was 4070 ± 65 milliseconds and the time
of high-field-strength imaging is often not at 4 T was 4472 ± 85 milliseconds. Because
met, however, because of new problems intro- the increase in T1 relaxation time as a func-
Keywords: 3 T, contrast enhancement,
MRI techniques, spine duced by these systems. One such problem is tion of magnetic field strength is expected to
found in 3-T imaging of the spine. T1-weight- be linear [2], the T1 relaxation time for CSF
DOI:10.2214/AJR.10.4887 ed fast spin-echo (FSE) sequences of the spine at 3 T would fall between the two values giv-
at 3 T show lower contrast between the CSF en. Thus, the T1 relaxation time of the spinal
Received May 1, 2010; accepted after revision
March 4, 2011.
and the spinal cord compared with 1.5-T im- cord increases by about 20% between 1.5 T
aging (Fig. 1). and 3 T, whereas the T1 relaxation time for
1
All authors: Department of Diagnostic Imaging, The paradoxical loss of contrast between CSF increases by less than 10%.
University of Texas M. D. Anderson Cancer Center, CSF and cord at 3 T is attributed to a rela- Adequate CSF nulling is important to dif-
1515 Holcombe Blvd, Unit 370, Houston, TX 77030.
Address correspondence to K. B. Shah
tively large increase in T1 relaxation time of ferentiate syrinx or syringomyelia from cord
(komal.shah@mdanderson.org). the spinal cord with increasing field strength edema and to avoid unnecessary suspicion of
[1], whereas the T1 relaxation time of CSF subarachnoid tumor seeding. One suggested
AJR 2011; 197:697–703 increases relatively slowly with increasing solution to the problem of lost CSF-cord con-
field strength. Stanisz et al. [2] found that trast at 3 T is the use of FLAIR sequences
0361–803X/11/1973–697
the mean (± SD) T1 relaxation time of the (Fig. 2), which have a broader dynamic con-
© American Roentgen Ray Society rat spinal cord at 1.5 T was 745 ± 37 mil- trast range and can recover some of the lost
AJR:197, September 2011 697
Shah et al.
Downloaded from www.ajronline.org by 101.255.45.218 on 04/20/19 from IP address 101.255.45.218. Copyright ARRS. For personal use only; all rights reserved
A B C
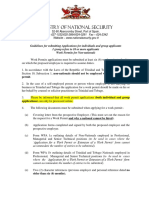
Fig. 1—67-year-old man with bone metastasis resulting from prostate cancer, 2 months after radiation treatment to T4.
A, Image of 3-T contrast-enhanced fat-saturated T1-weighted fast spin-echo (FSE) sequence (TR/TE, 700/14.544; inversion time [TI], 0; echo-train length [ETL], 4) shows
enhancing metastasis at T4 (arrow) and disk-osteophyte complex at T8–9 (asterisk). Cord and CSF are barely distinguishable from each other.
B, Image of 3-T contrast-enhanced fat-saturated T1-weighted FLAIR sequence (TR/TE, 3562/21.5; TI, 1238; ETL, 8) obtained immediately before fat-saturated T1-
weighted FSE shows improved cord-CSF distinction.
C, Comparison 1.5-T contrast-enhanced fat-saturated T1-weighted FSE sequence (TR/TE, 450/11.3; TI, 0; ETL, 3) obtained 10 weeks after 3-T scan shows typical cord-
CSF contrast. Compared with FSE sequence (A), deficiency of CSF-cord contrast at 3 T is evident.
contrast between spine and cord at 3 T [3, 4]. hanced T1-weighted FSE [10]. The purpose T1-weighted FLAIR, parameters were TR/TE of
Inversion recovery has been used success- of our study is to evaluate the clinical util- 2000–3600/21–22 and TI of 824–1238. IV contrast
fully in unenhanced spine imaging studies at ity of gadolinium-enhanced fat-saturated T1- consisted of 0.1 mmol/kg gadopentetate dimeglu-
both 1.5 and 3 T and has been shown to im- weighted FLAIR by comparing the conspi- mine (Magnevist, Bayer Healthcare Pharmaceuti-
prove CSF-cord distinction and detection of cuity of bone and soft-tissue spine lesions cals). The thoracic and lumbar spines were scanned
cord and marrow lesions at 1.5 T [5, 6]. How- to gadolinium-enhanced fat-saturated T1- using separate FOVs, at a single appointment, us-
ever, it is not known whether inversion re- weighted FSE sequences at 3 T. ing high-definition cervico-thoraco-lumbar coils.
covery affects evaluation of contrast-enhanc- The order in which the contrast-enhanced sagit-
ing intradural and extradural spine lesions. Materials and Methods tal sequences (thoracic fat-saturated T1-weighted
At our institution, spine imaging is more Patients FSE, thoracic fat-saturated T1-weighted FLAIR,
commonly requested for evaluation of bone This retrospective study was approved by the in- lumbar fat-saturated T1-weighted FSE, and lum-
metastasis than for cord pathology or de- stitutional review board, and written informed con- bar fat-saturated T1-weighted FLAIR) were to be
generative change. Fat-saturated T1-weight- sent was waived. The study was conducted in ac- scanned was not specified.
ed imaging after the IV administration of cordance with HIPAA guidelines. All consecutive
gadolinium-based contrast agent has been combined thoracic and lumbar spine MRI scans Image Analysis
shown to improve specificity for the diag- performed at 3 T between February and July 2008, All MRI scans were reviewed on a PACS (iSite,
nosis of bone metastases [7, 8], and this se- which included contrast-enhanced fat-saturated Philips Healthcare). Sagittal contrast-enhanced
quence is routinely performed at our insti- T1-weighted FSE and fat-saturated T1-weighted sequences were reviewed independently by one
tution. With respect to the brain, an early FLAIR in the sagittal plane, were reviewed. musculoskeletal radiologist with 6 years of expe-
study of gadolinium-enhanced T1-weight- rience and two neuroradiologists each with 3 years
ed FLAIR at 1.5 T concluded that enhanc- Image Acquisition of experience. Readings were independent and not
ing lesions were much less conspicuous on Scans were obtained on 3-T MRI units ca- in consensus.
T1-weighted FLAIR [9], whereas a more pable of 8- or 16-channel reconstruction (Excite A visual rating system of 1–7 was used to evalu-
recent study showed improved conspicuity HD or HDxt, GE Healthcare). The parameters ate lesion conspicuity in the following diagnostic
of enhancing brain lesions on T1-weighted for fat-saturated T1-weighted FSE were TR/TE categories: enhancing bone lesions, disk-osteophyte
FLAIR at 1.5 T compared with contrast-en- of 700–800/12–13 and TI of 0. For fat-saturated complexes, and other epidural lesions. A score of 1
698 AJR:197, September 2011
3-T T1-Weighted Imaging of Extradural Spinal Lesions
Fig. 2—30-year-old woman with von Hippel-Lindau
syndrome, thoracic cord syringomyelia, and
hemangioblastoma (not shown but seen equally well
on 3-T contrast-enhanced fat-saturated T1-weighted
FLAIR and fat-saturated T1-weighted fast spin-echo
[FSE]).
A, Image of 1.5-T contrast-enhanced fat-saturated
T1-weighted FSE sequence (TR/TE, 500/16.3;
Downloaded from www.ajronline.org by 101.255.45.218 on 04/20/19 from IP address 101.255.45.218. Copyright ARRS. For personal use only; all rights reserved
inversion time [TI], 0; echo-train length [ETL], 3)
shows syringomyelia at C7 and from T4 through T10.
B, Image of 3-T contrast-enhanced fat-saturated T1-
weighted FSE sequence (TR/TE, 900/12.8; TI, 0; ETL,
4) obtained 3 months later, at same time as images
shown in (C) and (D), shows decreased CSF-cord
contrast (arrowhead), possibly causing confusion as
to edema versus syringomyelia.
C, Image of 3-T contrast-enhanced fat-saturated
T1-weighted FLAIR sequence (TR/TE, 2994/21.8;
TI, 1067; ETL, 8) shows significantly improved CSF-
cord contrast clearly indicating fluid within cord
(arrowhead).
D, Image of 3-T T2-weighted FSE obtained at same
time as the images obtained in (A) and (B) reveals
intramedullary T2 hyperintensity, which may be in
keeping with edema or syringomyelia.
signified that the lesion was much more conspicu-
ous on the gadolinium-enhanced fat-saturated T1-
weighted FLAIR sequence, and a score of 7 signi-
fied that the lesion was much more conspicuous on
the gadolinium-enhanced fat-saturated T1-weight-
ed FSE sequence (Fig. 3). When multiple lesions in
a category were present, the readers were asked to
A B give a single overall score for all lesions in that cat-
egory. When chemical shift artifact was present in
the thoracic spine, the reviewer was asked to focus
on lesions that were not affected by the artifact. The
scale of 1 to 7 was also used to evaluate CSF-cord
contrast, with 1 indicating much higher CSF-cord
contrast on fat-saturated T1-weighted FLAIR and
7 indicating much higher CSF-cord contrast on fat-
saturated T1-weighted FSE.
The influence of the order of image acquisition
(injection time bias) was evaluated by comparing
the results of two subsets of patients: those who
had both thoracic and lumbar sagittal gadolinium-
enhanced fat-saturated T1-weighted FLAIR se-
quences performed before gadolinium-enhanced
fat-saturated T1-weighted FSE sequences, and
those who had both thoracic and lumbar gado-
linium-enhanced fat-saturated T1-weighted FSE
sequences performed before contrast-enhanced
fat-saturated T1-weighted FLAIR. Average con-
spicuity scores of these two subsets were compared
with each other and to a score of 4 (neutral).
Statistical Analysis
All statistical analyses were performed using
commercially available software (SAS version
9.1.3 for Windows, SAS Institute). The frequen-
cies of ratings were summarized by diagnostic
category (bone lesions, disk-osteophyte complex-
es, and other epidural lesions) and reader. Average
ratings for each lesion category were calculated
C D
AJR:197, September 2011 699
Shah et al.
Fig. 3—Rating sagittal scan may have been performed us-
1 4 7 system for evaluation
2 3 5 6 of conspicuity of
ing fat-saturated T1-weighted FSE before
lesions and CSF-cord fat-saturated T1-weighted FLAIR, but in the
distinction on FLAIR lumbar spine, the fat-saturated T1-weighted
and fast spin-echo (FSE) FLAIR sequence was performed first.
sequences.
Downloaded from www.ajronline.org by 101.255.45.218 on 04/20/19 from IP address 101.255.45.218. Copyright ARRS. For personal use only; all rights reserved
Much more Equally Much more
conspicuous conspicuous conspicuous Analysis
on FLAIR on SE Table 1 summarizes the average conspicu-
ity ratings in each category. The qualitative
for pooled data. The conspicuity scores were trans- scans, disk-osteophyte complexes were de- contrast between CSF and spinal cord was
formed to the logarithmic scale before subsequent tected on 138 scans, and 68 scans showed oth- much greater on contrast-enhanced fat-sat-
statistical analyses. er epidural lesions. In 68 scans with epidural urated T1-weighted FLAIR than on fat-sat-
lesions, 56 were due to metastasis (as diag- urated T1-weighted FSE, and the difference
Assessment of Conspicuity and Sequence nosed by the presence of a focal enhancing was statistically significant (mean score, 1.8;
of Scans epidural mass extending from a bone metasta- p < 0.0001). For bone lesions, the mean con-
Each lesion category was analyzed separately. sis), including three cases of pathologic frac- spicuity score was 3.6, the score for disk-os-
Because there were multiple observations per pa- ture. Two cases of suspected insufficiency teophyte complexes was 3.5, and the score
tient, a linear mixed model was used to account fracture, one case of diskitis, and four Tarlov for other epidural lesions was 3.4, indicating
for the correlation between observations from the cysts were also seen. The rest of the epidural a mild increase in conspicuity on contrast-
same patient. The mean and standard error were lesions were due to degenerative changes. All enhanced fat-saturated T1-weighted FLAIR.
estimated from the linear mixed model. The es- lesions seen on gadolinium-enhanced fat-sat- These mean conspicuities were significantly
timated mean was compared against log4, and a urated T1-weighted FSE were also identifiable different from a score of 4 (p < 0.0001).
p value was provided on the basis of z statistics. on gadolinium-enhanced fat-saturated T1-
Estimates of the mean and corresponding 95% CI weighted FLAIR. One enhancing bone lesion Comparison of Gadolinium-Enhanced Fat-
were back-transformed to the raw scale for report- seen on fat-saturated T1-weighted FLAIR was Saturated T1-Weighted FLAIR and Fat-
ing. A linear mixed model was also used to assess not visible on the fat-saturated T1-weighted Saturated T1-Weighted FSE by Scan Sequence
whether the sequence of scans affected the conspi- FSE sequence because of motion artifact. Injection-time bias was tested by compar-
cuity of the scores. Four scans revealed leptomeningeal en- ing the results of patients with gadolinium-
hancement, presumably due to metastasis. enhanced fat-saturated T1-weighted FLAIR
Interobserver Agreement Two scans revealed a syrinx, defined as fluid performed before fat-saturated T1-weighted
Agreement between readers was assessed by signal without enhancement, within the cord. FSE with the results of patients whose scans
using weighted kappa statistic. Scores were col- One of the scans with syrinx also included were performed in the opposite order. Across
lapsed into the following categories for analysis: intramedullary enhancing lesions. all diagnostic categories, the average rating
3 or less, 4, and 5 or greater. The 95% CIs for the In 55 of 156 scans, the gadolinium-en- when fat-saturated T1-weighted FLAIR was
weighted kappa values were calculated. The fol- hanced fat-saturated T1-weighted FLAIR se- performed first was 3.7, whereas the average
lowing criteria explain the kappa values: a kap- quence was performed before the gadolini- rating when fat-saturated T1-weighted FSE
pa value of 0.20 or less indicated poor agreement, um-enhanced fat-saturated T1-weighted FSE was performed first was 3.4 (Table 2). This
0.21–0.40 indicated fair agreement, 0.41–0.60 in- sequence in the thoracic spine, as well as in difference in conspicuity between the two se-
dicated moderate agreement, 0.61–0.80 indicated the lumbar spine. In 60 of 156 scans, the gad- quences when FLAIR was performed before
good agreement, and 0.81–1.00 indicated excel- olinium-enhanced fat-saturated T1-weighted FSE was not statistically significant (p = 0.15
lent agreement [11]. FSE sequence was obtained before the gad- for bone lesions, p = 0.20 for disk-osteophyte
olinium-enhanced fat-saturated T1-weighted complexes, and p = 0.11 for epidural lesions).
Results FLAIR in the thoracic spine, as well as in
Patients the lumbar spine. In the remaining 41 scans, Interobserver Agreement
There were 156 scans of 143 patients (101 the order of scanning was not consistent; Frequency graphs of the ratings in each
scans of women [mean age, 56 ± 13 years; age for example, the thoracic contrast-enhanced diagnostic category by reader are shown in
range, 20–90 years] and 55 scans of men [mean
age, 58 ± 13 years; age range, 18–79 years]).
TABLE 1: Scores for Conspicuity of Bone, Disk and Other Epidural Lesions,
Imaging and for CSF-Cord Distinction
Both contrast-enhanced fat-saturated T1- Diagnostic Category Score, Mean (95% CI)
weighted FLAIR and fat-saturated T1-weight- Bone lesion 3.6 (3.5–3.7)
ed FSE sequences were similar in duration
Disk-osteophyte complex 3.5 (3.4–3.6)
(3.5–4 minutes). All scans were rated for
CSF-cord distinction. In 99.6% of cases, the Other epidural disease 3.4 (3.2–3.6)
score for CSF-cord distinction was 3 or less CSF-cord distinction 1.8 (1.7–2.0)
(one reviewer gave a score of 4 on two scans). Note—p values indicate significant differences in the ratings from a score of 4 (neutral value); p < 0.0001 for
Bone lesions were detected on 129 of 156 all comparisons.
700 AJR:197, September 2011
3-T T1-Weighted Imaging of Extradural Spinal Lesions
TABLE 2: Scores for Conspicuity According to When Contrast-Enhanced noise ratio, contrast, and contrast-to-noise ra-
Fat-Saturated T1-Weighted Fast Spin-Echo (FSE) and Contrast- tio. Zhao et al. [12] reported improved contrast
Enhanced Fat-Saturated T1-Weighted FLAIR Was Performed between normal and neoplastic bone marrow
Order of Scan Sequences Bone Lesions Disk-Osteophyte Complex Other Epidural Disease signal using T1-weighted FSE without gado-
FSE performed first 3.4 (3.2–3.6) 3.4 (3.2–3.5) 3.4 (3.1–3.6)
linium enhancement at 3 T compared with
1.5 T. Lavdas et al. [13] showed qualitative
Downloaded from www.ajronline.org by 101.255.45.218 on 04/20/19 from IP address 101.255.45.218. Copyright ARRS. For personal use only; all rights reserved
FLAIR performed first 3.7 (3.5–3.9) 3.7 (3.4–4.0) 3.7 (3.4–4.0)
improvement in contrast-to-noise and signal-
pa 0.15 0.20 0.11 to-noise ratios and quantitative improvement
Note—Except for p values, data are mean score (95% CI). using unenhanced T1-weighted FLAIR com-
aIndicates significance of difference between the two groups.
pared with unenhanced T1-weighted FSE for
CSF nulling, viewing normal anatomic struc-
Figures 4–6. For bone lesions (Fig. 4), all re- 2 and for reviewers 2 and 3 with respect to tures, and evaluating degenerative and meta-
viewers gave scores of 3 or 4 for 75–80% of epidural lesions; these reviewer pairs com- static bone lesions at 3 T. Lavdas et al. [14] also
scans. For disk-osteophyte complexes (Fig. prised a small number of scans, with very recently found that chemical shift artifact in
5), reviewer 1 gave more scores of 4 than any few scores of 5 or greater. The kappa value the thoracic spine was decreased on contrast-
other, whereas reviewers 2 and 3 gave mainly for reviewers 1 and 3 with respect to epidural enhanced fat-saturated T1-weighted FLAIR
scores of 3 and 5. For epidural lesions (Fig. lesions was 0.15 (95% CI, 0.15–0.44). compared with contrast-enhanced fat-saturat-
6), reviewers 1 and 3 gave mainly scores of 4, ed T1-weighted FSE. However, the use of T1-
whereas reviewer 2 slightly favored a score of Discussion FLAIR imaging after IV administration of
3, but again all reviewers gave a score of 3 or Recent investigations of 3-T spine imag- gadolinium-based contrast agent in the spine
4 in 73–85% of cases. Reviewer 3 rated fewer ing have found improvements in signal-to- at 3 T has not been previously evaluated.
scans for epidural lesions than did reviewers
1 and 3. Figure 7 shows that nearly all ratings
TABLE 3: Interobserver Agreement for Bone Lesions and Disk-Osteophyte
for CSF-cord distinction were less than 3.
Complexes
Table 3 shows kappa statistics for the di-
agnostic categories. Kappa statistics could Disk-Osteophyte Complexes, κ
not be calculated for CSF-cord distinction Reader Pair Bone Lesions, κ (95% CI) (95% CI)
because all reviewers rated nearly all of the Readers 1 and 2 0.29 (0.15–0.44) 0.08 (−0.09 to 0.25)
scans at 3 or less and only one reviewer gave
Readers 2 and 3 0.29 (0.15–0.44) 0.47 (0.26–0.68)
two scans a score of 4. Kappa values also
could not be calculated for reviewers 1 and Readers 1 and 3 0.49 (0.36–0.63) 0.20 (0–0.40)
80 Reader 1 40 Reader 1 35 Reader 1
Reader 2 Reader 2 Reader 2
Reader 3 Reader 3 Reader 3
70 35 30
60 30
25
50 25
Frequency (%)
Frequency (%)
Frequency (%)
20
40 20
15
30 15
10
20 10
5
10 5
0 0 0
1 2 3 4 5 6 7 1 2 3 4 5 6 7 1 2 3 4 5 6 7
Conspicuity Rating Conspicuity Rating Conspicuity Rating
Fig. 4—Plot of frequency of conspicuity ratings Fig. 5—Plot of frequency of conspicuity ratings for Fig. 6—Plot of frequency of conspicuity ratings for
for bone lesions by reader. Each line represents disk-osteophyte complexes by reader. Reader 1 gave epidural lesions by reader. Readers 1 and 3 gave
one reviewer. Reviewer 1 gave scores of mostly 4. mostly scores of 4. Readers 2 and 3 gave mostly mainly scores of 4, whereas reader 2 gave mainly
Reviewer 2 gave mostly scores of 3. Reviewer 3 gave scores of 3 and 5. Number of scans each reader scores of 3 and 4. Number of scans rated for epidural
relatively even number of scores of 3 and 4. scored for disk-osteophyte complex varied by reader. lesions varied by reader.
AJR:197, September 2011 701
Shah et al.
elapsed after contrast injection in this retro- slightly increased conspicuity of all bone le-
140 Reader 1 spective study, we did find that the average sions, disk-osteophyte complexes, and other
Reader 2
scan time for the fat-saturated T1-weighted epidural lesions was perceived on contrast-
Reader 3
120 FLAIR and fat-saturated T1-weighted FSE enhanced T1-weighted FLAIR. The results
sequences in our study was 3.5–4.0 minutes. of this study suggest that contrast-enhanced
A review of prior studies of dynamic en- fat-saturated T1-weighted FLAIR can replace
Downloaded from www.ajronline.org by 101.255.45.218 on 04/20/19 from IP address 101.255.45.218. Copyright ARRS. For personal use only; all rights reserved
100
hancement of bone malignancies, including contrast-enhanced fat-saturated T1-weighted
bone metastases, reveals that steep time-en- FSE for diagnosis of extradural lesions and
Frequency (%)
80 hancement curves, on first-pass dynamic im- may be advantageous because abnormalities
aging, are usually seen within 40 seconds af- that are more conspicuous tend to be easier to
ter injection [16, 17]. In malignancies, this detect than ones that are less conspicuous. Of
60
may be followed by an early phase washout note, our study was limited by its retrospec-
or plateau, within about 80 seconds of injec- tive design. The results of this study can be
40 tion. Typically, the time-intensity curve in verified in a prospective manner.
these studies is not extended past 5 minutes; The marked improvement in contrast be-
Chen et al. [17] found a gradual washout at tween CSF and spinal cord on contrast-en-
20
280 seconds for both malignant and nonma- hanced fat-saturated T1-weighted FLAIR
lignant categories of bone lesions examined. image suggests that detection of enhancing in-
0 Assuming that the gradual washout contin- tradural lesions, as well as syrinx and syrin-
1 2 3 4 5 6 7 ued, our second scan would have been ex- gomyelia, may be improved by using this se-
Conspicuity Rating pected to show decreased signal intensity and quence at 3 T. This idea will be investigated in
decreased conspicuity in contrast-enhancing future studies. Intradural lesions were not inves-
Fig. 7—Plot of frequency of conspicuity ratings for lesions, compared with the first scan. This was tigated in our study because of the lack of posi-
CSF-cord distinction by reader. All but two scores not the case. It may be that a second plateau is tive findings in this selected group of patients.
(99.6%) were 3 or less.
reached after the late (280 seconds) gradual
washout and that both of our scans fell into References
Our study found that all extradural lesion this plateau, such that there was no significant 1. Rooney WD, Johnson G, Li X, et al. Magnetic
conspicuity was increased on contrast-en- difference between our two scans. field and tissue dependencies of human brain lon-
hanced fat-saturated T1-weighted FLAIR com- Interobserver agreement in our study over- gitudinal 1H2O relaxation in vivo. Magn Reson
pared with contrast-enhanced fat-saturated T1- all was no better than moderate. This is most Med 2007; 57:308–318
weighted FSE. Conspicuity has been defined likely because of the choice of a qualitative 2. Stanisz GJ, Odrobina EE, Pun J, et al. T1, T2 re-
as lesion contrast against surround complexi- 7-point scale, in which reviewers could make laxation and magnetization transfer in tissue at
ty [15]. The increased conspicuity on FLAIR fine distinctions between one rating and the 3T. Magn Reson Med 2005; 54:507–512
may be due to increased lesion contrast inher- adjacent one. Variability in the number of 3. Shapiro MD. MR imaging of the spine at 3T. Magn
ent to the sequence, as seen on unenhanced epidural lesions rated was due to differences Reson Imaging Clin N Am 2006; 14:97–108
comparison of 3-T T1-weighted FLAIR and in interpretation of whether the cortex of the 4. Runge VM. Spine: thoracic—cord. In: Runge
T1-weighted FSE [13], as a result of broader bone was involved by bone metastasis, which VM, Nitz WR, Schmeets SH, Schoenberg SO,
dynamic contrast range [6], or because of ac- can be difficult to distinguish by MRI. eds. Clinical 3T magnetic resonance. New York,
cumulation of gadolinium-based contrast agent Because an increase in contrast intensity can NY: Thieme Medical Publishers, 2007:126
within the lesion over time. Alternatively, in- be an indication of disease progression in pa- 5. Erdem LO, Erdem CZ, Acikgoz B, Gundogdu S.
creased conspicuity can arise from decreased tients with cancer with bony metastases, use Degenerative disc disease of the lumbar spine: a
surround complexity, perhaps because of sup- of the gadolinium-enhanced fat-saturated T1- prospective comparison of fast T1-weighted fluid-
pression of background marrow fluid content. weighted FLAIR sequence could result in a attenuated inversion recovery and T1-weighted
We did not quantify lesion contrast or surround spurious appearance of progressive metastasis turbo spin echo MR imaging. Eur J Radiol 2005;
complexity, but quantification with the aim of compared with a prior gadolinium-enhanced fat- 55:277–282
defining the mechanism of increased conspicu- saturated T1-weighted FSE. When comparing 6. Melhem ER, Israel DA, Eustace S, Jara H. MR of the
ity could be pursued in further studies. gadolinium-enhanced fat-saturated T1-weight- spine with a fast T1-weighted fluid-attenuated inver-
The finding that enhancing lesions were ed FLAIR to a prior gadolinium-enhanced fat- sion recovery sequence. AJNR 1997; 18:447–454
more conspicuous on the second of the two saturated T1-weighted FSE sequence, increased 7. Mahnken AH, Wildberger JE, Adam G, et al. Is
scans (i.e., lower average score for all le- conspicuity of bone metastasis in itself should there a need for contrast-enhanced T1-weighted
sions when gadolinium-enhanced fat-satu- not be construed as progression of metastasis; MRI of the spine after inconspicuous short tau
rated T1-weighted FSE was performed first evidence of increased size or number of metas- inversion recovery imaging? Eur Radiol 2005; 15:
vs higher average score when gadolinium- tases should be sought. 1387–1392
enhanced fat-saturated T1-weighted FLAIR In summary, comparison of sagittal con- 8. Meyer JS, Siegel MJ, Farooqui SO, Jaramillo D,
was performed first) might have been com- trast-enhanced fat-saturated T1-weighted FSE Fletcher BD, Hoffer FA. Which MRI sequence of
patible with an injection-time bias, but the and FLAIR on 156 spine MRI scans revealed the spine best reveals bone-marrow metastases of
difference was not statistically significant. that all extradural lesions were identifiable by neuroblastoma? Pediatr Radiol 2005; 35:778–785
Although we could not control the time the reviewers on T1-weighted FLAIR and that 9. Melhem ER, Bert RJ, Walker RE. Usefulness of
702 AJR:197, September 2011
3-T T1-Weighted Imaging of Extradural Spinal Lesions
optimized gadolinium-enhanced fast fluid-attenu- marrow contrast at 3 T versus 1.5 T. AJR 2009; tured noise, and film reader error. AJR 1976;
ated inversion recovery MR imaging in revealing 192:873–880 126:1233–1238
lesions of the brain. AJR 1998; 171:803–807 13. Lavdas E, Vlychou M, Arikidis N, Kapsalaki E, 16. Verstraete KL, De Deene Y, Roels H, Dierick A,
10. Hori M, Okubo T, Uozumi K, Ishigame K, Kuma- Roka V, Fezoulidis IV. Comparison of T1-weight- Uyttendaele D, Kunnen M. Benign and malignant
gai H, Araki T. T1-weighted fluid-attenuated in- ed fast spin-echo and T1-weighted fluid-attenuat- musculoskeletal lesions: dynamic contrast-en-
version recovery at low field strength: a viable al- ed inversion recovery images of the lumbar spine hanced MR imaging—parametric “first-pass” im-
Downloaded from www.ajronline.org by 101.255.45.218 on 04/20/19 from IP address 101.255.45.218. Copyright ARRS. For personal use only; all rights reserved
ternative for T1-weighted intracranial imaging. at 3.0 Tesla. Acta Radiol 2010; 51:290–295 ages depict tissue vascularization and perfusion.
AJNR 2003; 24:648–651 14. Lavdas E, Mavroidis P, Vassiou K, Roka V, Fe- Radiology 1994; 192:835–843
11. Cohen J. Weighted kappa: nominal scale agree- zoulidis IV, Vlychou M. Elimination of chemical 17. Chen WT, Shih TT, Chen RC, et al. Blood perfu-
ment with provision for scaled disagreement or shift artifacts of thoracic spine with contrast-en- sion of vertebral lesions evaluated with gadolini-
partial credit. Psychol Bull 1968; 70:213–220 hanced FLAIR imaging with fat suppression at um-enhanced dynamic MRI: in comparison with
12. Zhao J, Krug R, Xu D, Lu Y, Link TM. MRI of the 3.0 T. Magn Reson Imaging 2010; 28:1535–1540 compression fracture and metastasis. J Magn Re-
spine: image quality and normal-neoplastic bone 15. Kundel HL, Revesz G. Lesion conspicuity, struc- son Imaging 2002; 15:308–314
AJR:197, September 2011 703
Vous aimerez peut-être aussi
- Comparative Analysis of Radiation Dose and Image Quality BetweenDocument5 pagesComparative Analysis of Radiation Dose and Image Quality BetweenIshani Anushika JayakodyPas encore d'évaluation
- Eye Lens Dose During CT ExamDocument7 pagesEye Lens Dose During CT ExamSamu SimamesaPas encore d'évaluation
- Lens Dose in Routine Head CTDocument8 pagesLens Dose in Routine Head CTAglaia T.Pas encore d'évaluation
- Ajr 14 14266Document5 pagesAjr 14 14266Jorge Alberto GCPas encore d'évaluation
- CT of Globe Rupture: Analysis and Frequency of FindingsDocument8 pagesCT of Globe Rupture: Analysis and Frequency of FindingsdrmgroaPas encore d'évaluation
- Lung Nodule Detection by Microdose CT Versus Chest RadiographyDocument9 pagesLung Nodule Detection by Microdose CT Versus Chest RadiographyTatiana RecinosPas encore d'évaluation
- No Reference Journal Study Design Level of EvidenceDocument6 pagesNo Reference Journal Study Design Level of EvidenceHendra HamzahPas encore d'évaluation
- Ajr 17 19185Document9 pagesAjr 17 19185Bruno MeloPas encore d'évaluation
- Solid Renal Masses: What The Numbers Tell Us: Stella K. Kang William C. Huang Pari V. Pandharipande Hersh ChandaranaDocument11 pagesSolid Renal Masses: What The Numbers Tell Us: Stella K. Kang William C. Huang Pari V. Pandharipande Hersh ChandaranaTạ Minh ZSPas encore d'évaluation
- The Clinical Correlation of A New Practical MRI Method For Grading Cervical Neural Foraminal Stenosis Based On Oblique Sagittal ImagesDocument6 pagesThe Clinical Correlation of A New Practical MRI Method For Grading Cervical Neural Foraminal Stenosis Based On Oblique Sagittal ImagesThiago Astil RizzettoPas encore d'évaluation
- Dual-Energy CT of The Brain and Intracranial VesselsDocument8 pagesDual-Energy CT of The Brain and Intracranial VesselsMuhammad Rafiee SukmaPas encore d'évaluation
- PROPELLER Technique To Improve Image Quality of MRI of The ShoulderDocument8 pagesPROPELLER Technique To Improve Image Quality of MRI of The ShoulderDhoni AvantasiaPas encore d'évaluation
- Comparison of MERGE and Axial T2-Weighted Fast Spin-Echo Sequences For Detection of Multiple Sclerosis Lesions in The Cervical Spinal CordDocument6 pagesComparison of MERGE and Axial T2-Weighted Fast Spin-Echo Sequences For Detection of Multiple Sclerosis Lesions in The Cervical Spinal CordOtong Zam ZamyPas encore d'évaluation
- Scanning Beyond Anatomic Limits of The Thorax in Chest CT - Findings, Radiation Dose, and Automatic Tube Current ModulationDocument6 pagesScanning Beyond Anatomic Limits of The Thorax in Chest CT - Findings, Radiation Dose, and Automatic Tube Current Modulationdestian ryanPas encore d'évaluation
- Ajr 09 4032Document7 pagesAjr 09 4032Roshi_11Pas encore d'évaluation
- Uas CT Scan - Jurnal - Dwi Ajeng Risqy Hasanah Syam - P1337430219162 PDFDocument6 pagesUas CT Scan - Jurnal - Dwi Ajeng Risqy Hasanah Syam - P1337430219162 PDFDwi Ajeng Risqy HasanahSyamPas encore d'évaluation
- CTA ExtremityDocument8 pagesCTA Extremityrio trisonaPas encore d'évaluation
- Sagittal Plane Analysis of Head, Neck, and Trunk Kinematics and Electromyographic Activity During LocomotionDocument8 pagesSagittal Plane Analysis of Head, Neck, and Trunk Kinematics and Electromyographic Activity During LocomotionashimaPas encore d'évaluation
- Jospt 1999 29 7 413Document8 pagesJospt 1999 29 7 413محمد مصطفيPas encore d'évaluation
- 8.thoracic BlocksDocument39 pages8.thoracic BlocksMiguel AradaPas encore d'évaluation
- Clinical Practice in PET CT For The Management of Head and Neck Squamous Cell CancerDocument15 pagesClinical Practice in PET CT For The Management of Head and Neck Squamous Cell CancerlkitkatgirlPas encore d'évaluation
- Ajr 09 3543Document5 pagesAjr 09 3543Jakaria Khan SakibPas encore d'évaluation
- Subchondroplasty What TheDocument6 pagesSubchondroplasty What TheikhsanPas encore d'évaluation
- Ajr 14 12810Document5 pagesAjr 14 12810Eka JuliantaraPas encore d'évaluation
- Ajr 15 14806Document5 pagesAjr 15 14806rulitoss_41739Pas encore d'évaluation
- Bone Marrow T1-W DifferentialDocument17 pagesBone Marrow T1-W DifferentialStancu Oana RuxandraPas encore d'évaluation
- MRI of Spinal Bone Marrow Part 2 T1-Weighted Imaging-Based Differential DiagnosisDocument13 pagesMRI of Spinal Bone Marrow Part 2 T1-Weighted Imaging-Based Differential DiagnosisAyşe BanuPas encore d'évaluation
- Thoracic CT Findings in Birt-Hogg-Dubé SyndromeDocument4 pagesThoracic CT Findings in Birt-Hogg-Dubé SyndromeicaeePas encore d'évaluation
- Berlin Et Al 2015 Successful Dose Reduction Using Reduced Tube Voltage With Hybrid Iterative Reconstruction inDocument8 pagesBerlin Et Al 2015 Successful Dose Reduction Using Reduced Tube Voltage With Hybrid Iterative Reconstruction inJonah D'nominee La'ReplicaPas encore d'évaluation
- Akramazad A 10 1528 6 9a4ec16Document10 pagesAkramazad A 10 1528 6 9a4ec16Aryan ShamiliPas encore d'évaluation
- TMP A467Document9 pagesTMP A467FrontiersPas encore d'évaluation
- Ajr Dect PDFDocument11 pagesAjr Dect PDFTom PatrickPas encore d'évaluation
- AndrogenreceptorsDocument6 pagesAndrogenreceptorsReda MostaPas encore d'évaluation
- Benefits of Use of Power Lab in Practica PDFDocument4 pagesBenefits of Use of Power Lab in Practica PDFRoy HarperPas encore d'évaluation
- RSC Advances: PaperDocument8 pagesRSC Advances: PaperTrần Thị Như HoaPas encore d'évaluation
- MR Angiography at 3 T of Peripheral Arterial Disease: A Randomized Prospective Comparison of Gadoterate Meglumine and GadobutrolDocument11 pagesMR Angiography at 3 T of Peripheral Arterial Disease: A Randomized Prospective Comparison of Gadoterate Meglumine and GadobutrolKevin AdrianPas encore d'évaluation
- Ajr 163 1 8010211Document5 pagesAjr 163 1 8010211Eliana NataliaPas encore d'évaluation
- Top Down Control of Spinal Sensorimotor Circuits Essential For SurvivalDocument8 pagesTop Down Control of Spinal Sensorimotor Circuits Essential For SurvivalErick SolisPas encore d'évaluation
- Csi Plan StudyDocument8 pagesCsi Plan Studyapi-527662950Pas encore d'évaluation
- Oral-Maxillary Sinus Fistula (Oroantral Fistula) :: Clinical Features and Findings On Multiplanar CTDocument4 pagesOral-Maxillary Sinus Fistula (Oroantral Fistula) :: Clinical Features and Findings On Multiplanar CTnataliayobeantoPas encore d'évaluation
- Evaluation of Dural Venous Sinuses and Con Uence of Sinuses Via MRI Venography: Anatomy, Anatomic Variations, and The Classification of VariationsDocument7 pagesEvaluation of Dural Venous Sinuses and Con Uence of Sinuses Via MRI Venography: Anatomy, Anatomic Variations, and The Classification of VariationsYulita MustikasariPas encore d'évaluation
- Acupuncture For Chronic PainDocument10 pagesAcupuncture For Chronic PaindanielPas encore d'évaluation
- Persiapan Osce Nasional: Dept. Obstetri Dan Ginekologi FK UnairDocument5 pagesPersiapan Osce Nasional: Dept. Obstetri Dan Ginekologi FK UnairYanis Widhiya NingrumPas encore d'évaluation
- Lit Matrix FinalDocument3 pagesLit Matrix Finalapi-420731316Pas encore d'évaluation
- IMRT: A Review and Preview: Physics in Medicine & BiologyDocument18 pagesIMRT: A Review and Preview: Physics in Medicine & BiologychatsashPas encore d'évaluation
- Serum Protein Electrophoresis Procedure: BibliographyDocument4 pagesSerum Protein Electrophoresis Procedure: BibliographyAhmad SolihinPas encore d'évaluation
- A Correlative Study of Solitary Thyroid Nodules.18Document6 pagesA Correlative Study of Solitary Thyroid Nodules.18Nan NaanPas encore d'évaluation
- Contreras-Vidal 2016 J. Neural Eng. 13 031001Document17 pagesContreras-Vidal 2016 J. Neural Eng. 13 031001Vitor Alves CruzPas encore d'évaluation
- Incidental Thyroid Nodules On Chest CT: Review of The Literature and Management SuggestionsDocument6 pagesIncidental Thyroid Nodules On Chest CT: Review of The Literature and Management SuggestionstaufikolingPas encore d'évaluation
- Protable Ultra Sound AlokaDocument4 pagesProtable Ultra Sound AlokaAjish joPas encore d'évaluation
- Christensen Et Al 2012 Characterization of The Solitary Pulmonary Nodule 18f FDG Pet Versus Nodule Enhancement CTDocument7 pagesChristensen Et Al 2012 Characterization of The Solitary Pulmonary Nodule 18f FDG Pet Versus Nodule Enhancement CTLeticia PortilloPas encore d'évaluation
- Ou,°a, O, Applied PhysiologyDocument6 pagesOu,°a, O, Applied PhysiologyCristian BáscoloPas encore d'évaluation
- Aging Changes of The Midfacial Fat Compartments A.45Document11 pagesAging Changes of The Midfacial Fat Compartments A.45Juliana BrunettoPas encore d'évaluation
- BT200 - Clinical Evaluation ReportDocument5 pagesBT200 - Clinical Evaluation ReportfjvillamunozPas encore d'évaluation
- Evaluation of Total Corneal Power MeasurementsDocument7 pagesEvaluation of Total Corneal Power MeasurementsMariana Luzardo bravoPas encore d'évaluation
- Electrical Stimulation of Denervated Muscles: First Results of A Clinical StudyDocument5 pagesElectrical Stimulation of Denervated Muscles: First Results of A Clinical StudychicnblinkPas encore d'évaluation
- Artigo 01 Model-Based Iterative Reconstruction in CT EnterographyDocument9 pagesArtigo 01 Model-Based Iterative Reconstruction in CT EnterographyKleytonSilvaPas encore d'évaluation
- Small Animal Cardiology Auscultation - Vet VisionsDocument1 pageSmall Animal Cardiology Auscultation - Vet Visionsyuaifafa25Pas encore d'évaluation
- Abdominal MRI at 3.0 T: The Basics Revisited: Elmar M. Merkle Brian M. DaleDocument9 pagesAbdominal MRI at 3.0 T: The Basics Revisited: Elmar M. Merkle Brian M. DalehusadaPas encore d'évaluation
- The Sutures of the Skull: Anatomy, Embryology, Imaging, and SurgeryD'EverandThe Sutures of the Skull: Anatomy, Embryology, Imaging, and SurgeryPas encore d'évaluation
- Cardiac MriDocument35 pagesCardiac Mrianon_302681452Pas encore d'évaluation
- Jmri 21141Document7 pagesJmri 21141anon_302681452Pas encore d'évaluation
- Sar22 (Edit)Document1 pageSar22 (Edit)anon_302681452Pas encore d'évaluation
- Sar (Safety Magnetic Resonance Imaging)Document1 pageSar (Safety Magnetic Resonance Imaging)anon_302681452Pas encore d'évaluation
- Ajr 2Document3 pagesAjr 2anon_302681452Pas encore d'évaluation
- Optimizing Imaging Parameters For MR Evaluation of The SpineDocument10 pagesOptimizing Imaging Parameters For MR Evaluation of The Spineanon_302681452Pas encore d'évaluation
- Ajr 2Document3 pagesAjr 2anon_302681452Pas encore d'évaluation
- Coefficient of Restitution - Center of MassDocument3 pagesCoefficient of Restitution - Center of MassMannyCesPas encore d'évaluation
- The Chassis OC 500 LE: Technical InformationDocument12 pagesThe Chassis OC 500 LE: Technical InformationAbdelhak Ezzahrioui100% (1)
- Ace 2Document184 pagesAce 2Raju LaxmipathiPas encore d'évaluation
- Quiz 2 I - Prefix and Suffix TestDocument10 pagesQuiz 2 I - Prefix and Suffix Testguait9Pas encore d'évaluation
- Salwico CS4000 Fire Detection System: Consilium Marine ABDocument38 pagesSalwico CS4000 Fire Detection System: Consilium Marine ABJexean SañoPas encore d'évaluation
- Visual Inspection ReportDocument45 pagesVisual Inspection ReportKhoirul AnamPas encore d'évaluation
- The Impact of Personnel Behaviour in Clean RoomDocument59 pagesThe Impact of Personnel Behaviour in Clean Roomisrael afolayan mayomiPas encore d'évaluation
- Work Permits New Guideline Amendments 2021 23.11.2021Document7 pagesWork Permits New Guideline Amendments 2021 23.11.2021Sabrina BrathwaitePas encore d'évaluation
- Certificate of Attendance: Yosapat NashulahDocument2 pagesCertificate of Attendance: Yosapat NashulahStrata WebPas encore d'évaluation
- Catch Up RPHDocument6 pagesCatch Up RPHபிரதீபன் இராதேPas encore d'évaluation
- NJEX 7300G: Pole MountedDocument130 pagesNJEX 7300G: Pole MountedJorge Luis MartinezPas encore d'évaluation
- Crusader Castle Al-Karak Jordan Levant Pagan Fulk, King of Jerusalem MoabDocument3 pagesCrusader Castle Al-Karak Jordan Levant Pagan Fulk, King of Jerusalem MoabErika CalistroPas encore d'évaluation
- Listening Tests 81112Document13 pagesListening Tests 81112luprof tpPas encore d'évaluation
- International Business ManagementDocument3 pagesInternational Business Managementkalaiselvi_velusamyPas encore d'évaluation
- Verilog A Model To CadenceDocument56 pagesVerilog A Model To CadenceJamesPas encore d'évaluation
- EvolutionCombatMedic 2022Document17 pagesEvolutionCombatMedic 2022smith.kevin1420344100% (1)
- Market EquilibriumDocument36 pagesMarket EquilibriumLiraOhPas encore d'évaluation
- 353 Version 7thDocument1 page353 Version 7thDuc NguyenPas encore d'évaluation
- Chapter I. Scope of Distributive Trade StatisticsDocument11 pagesChapter I. Scope of Distributive Trade StatisticsNguyễn Hà Diệu LinhPas encore d'évaluation
- 0409 Book About Minoru Yamasaki, ReviewDocument4 pages0409 Book About Minoru Yamasaki, RevieweviannPas encore d'évaluation
- Dash8 200 300 Electrical PDFDocument35 pagesDash8 200 300 Electrical PDFCarina Ramo LakaPas encore d'évaluation
- Poka-Yoke or Mistake Proofing: Historical Evolution.Document5 pagesPoka-Yoke or Mistake Proofing: Historical Evolution.Harris ChackoPas encore d'évaluation
- Reflective Memo 1-PracticumDocument5 pagesReflective Memo 1-Practicumapi-400515862Pas encore d'évaluation
- RADMASTE CAPS Grade 11 Chemistry Learner GuideDocument66 pagesRADMASTE CAPS Grade 11 Chemistry Learner Guideamajobe34Pas encore d'évaluation
- Investing in Granada's Property Market - Gaspar LinoDocument1 pageInvesting in Granada's Property Market - Gaspar LinoGaspar LinoPas encore d'évaluation
- 8D & 7QC ToolsDocument117 pages8D & 7QC ToolsAshok Kumar100% (1)
- p7000 Series PDFDocument592 pagesp7000 Series PDFtony445Pas encore d'évaluation
- CP3 - June2019 2Document5 pagesCP3 - June2019 2Sifei ZhangPas encore d'évaluation
- PEA Comp Study - Estate Planning For Private Equity Fund Managers (ITaback, JWaxenberg 10 - 10)Document13 pagesPEA Comp Study - Estate Planning For Private Equity Fund Managers (ITaback, JWaxenberg 10 - 10)lbaker2009Pas encore d'évaluation
- Pepperberg Notes On The Learning ApproachDocument3 pagesPepperberg Notes On The Learning ApproachCristina GherardiPas encore d'évaluation