Vous aimerez peut-être aussi
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)D'EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Évaluation : 4.5 sur 5 étoiles4.5/5 (121)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryD'EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryÉvaluation : 3.5 sur 5 étoiles3.5/5 (231)
- Grit: The Power of Passion and PerseveranceD'EverandGrit: The Power of Passion and PerseveranceÉvaluation : 4 sur 5 étoiles4/5 (588)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaD'EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaÉvaluation : 4.5 sur 5 étoiles4.5/5 (266)
- Never Split the Difference: Negotiating As If Your Life Depended On ItD'EverandNever Split the Difference: Negotiating As If Your Life Depended On ItÉvaluation : 4.5 sur 5 étoiles4.5/5 (838)
- The Emperor of All Maladies: A Biography of CancerD'EverandThe Emperor of All Maladies: A Biography of CancerÉvaluation : 4.5 sur 5 étoiles4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingD'EverandThe Little Book of Hygge: Danish Secrets to Happy LivingÉvaluation : 3.5 sur 5 étoiles3.5/5 (400)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeD'EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeÉvaluation : 4 sur 5 étoiles4/5 (5794)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyD'EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyÉvaluation : 3.5 sur 5 étoiles3.5/5 (2259)
- Shoe Dog: A Memoir by the Creator of NikeD'EverandShoe Dog: A Memoir by the Creator of NikeÉvaluation : 4.5 sur 5 étoiles4.5/5 (537)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreD'EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreÉvaluation : 4 sur 5 étoiles4/5 (1090)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersD'EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersÉvaluation : 4.5 sur 5 étoiles4.5/5 (345)
- Team of Rivals: The Political Genius of Abraham LincolnD'EverandTeam of Rivals: The Political Genius of Abraham LincolnÉvaluation : 4.5 sur 5 étoiles4.5/5 (234)
- Her Body and Other Parties: StoriesD'EverandHer Body and Other Parties: StoriesÉvaluation : 4 sur 5 étoiles4/5 (821)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceD'EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceÉvaluation : 4 sur 5 étoiles4/5 (895)
- Bank StatementDocument4 pagesBank StatementKristin BrooksPas encore d'évaluation
- AKT - 2023-04-04 - Franchise Disclosure DocumentDocument243 pagesAKT - 2023-04-04 - Franchise Disclosure DocumentFuzzy PandaPas encore d'évaluation
- The Unwinding: An Inner History of the New AmericaD'EverandThe Unwinding: An Inner History of the New AmericaÉvaluation : 4 sur 5 étoiles4/5 (45)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureD'EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureÉvaluation : 4.5 sur 5 étoiles4.5/5 (474)
- On Fire: The (Burning) Case for a Green New DealD'EverandOn Fire: The (Burning) Case for a Green New DealÉvaluation : 4 sur 5 étoiles4/5 (74)
- The Yellow House: A Memoir (2019 National Book Award Winner)D'EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Évaluation : 4 sur 5 étoiles4/5 (98)
- Problems Chapter 11Document29 pagesProblems Chapter 11Incia100% (1)
- Types of Production ProcessDocument24 pagesTypes of Production ProcessPRIYANK89% (18)
- Cargo Handling: (C) UPESDocument382 pagesCargo Handling: (C) UPESAditya SharmaPas encore d'évaluation
- The Political Economy of Growth in Vietnam BetweenDocument29 pagesThe Political Economy of Growth in Vietnam BetweenrexPas encore d'évaluation
- Ecommerce in Diff Cultures PDFDocument97 pagesEcommerce in Diff Cultures PDFInciaPas encore d'évaluation
- Kavanagh3e LN17 Styled 17Document17 pagesKavanagh3e LN17 Styled 17InciaPas encore d'évaluation
- See For Research DesignDocument25 pagesSee For Research DesignInciaPas encore d'évaluation
- Literature Review On Feature Identification in Sentiment AnalysisDocument6 pagesLiterature Review On Feature Identification in Sentiment AnalysisInciaPas encore d'évaluation
- Impact of Culture On Ecommerce Purchase IntentionDocument38 pagesImpact of Culture On Ecommerce Purchase IntentionInciaPas encore d'évaluation
- E Commerce A Solution To Pakistans Economic WoesDocument27 pagesE Commerce A Solution To Pakistans Economic WoesInciaPas encore d'évaluation
- Lecture Outline: Human Resource Information Systems and International Human Resource ManagementDocument19 pagesLecture Outline: Human Resource Information Systems and International Human Resource ManagementInciaPas encore d'évaluation
- Lecture Outline: Performance Management, Compensation, Benefits, Payroll, and The Human Resource Information SystemDocument22 pagesLecture Outline: Performance Management, Compensation, Benefits, Payroll, and The Human Resource Information SystemInciaPas encore d'évaluation
- Kavanagh3e LN16 Styled 15Document15 pagesKavanagh3e LN16 Styled 15InciaPas encore d'évaluation
- Lecture Outline: Training and Development: Issues and Human Resource Information Systems ApplicationsDocument20 pagesLecture Outline: Training and Development: Issues and Human Resource Information Systems ApplicationsInciaPas encore d'évaluation
- Inward Foreign Direct Investment: A Case Study of Pakistan: Mediterranean Journal of Social Sciences October 2018Document20 pagesInward Foreign Direct Investment: A Case Study of Pakistan: Mediterranean Journal of Social Sciences October 2018InciaPas encore d'évaluation
- Solutions To Exercises - Chap 6Document20 pagesSolutions To Exercises - Chap 6InciaPas encore d'évaluation
- Political Ideology and FDI: Radical ViewDocument11 pagesPolitical Ideology and FDI: Radical ViewInciaPas encore d'évaluation
- European Union Creation and Brexit by Farhan Ahmed Visiting Faculty at Bahria UniversityDocument39 pagesEuropean Union Creation and Brexit by Farhan Ahmed Visiting Faculty at Bahria UniversityInciaPas encore d'évaluation
- Chapter 12 ProblemsDocument40 pagesChapter 12 ProblemsInciaPas encore d'évaluation
- Global Theories by Farhan AhmedDocument19 pagesGlobal Theories by Farhan AhmedInciaPas encore d'évaluation
- Globalization in 21st CenturyDocument15 pagesGlobalization in 21st CenturyInciaPas encore d'évaluation
- Geopolitics Gulf WarDocument2 pagesGeopolitics Gulf WarInciaPas encore d'évaluation
- CORE CV Template 1Document3 pagesCORE CV Template 1InciaPas encore d'évaluation
- Solutions To Exercises - Chap 3Document27 pagesSolutions To Exercises - Chap 3InciaPas encore d'évaluation
- Solutions To Exercises - CHAP4Document16 pagesSolutions To Exercises - CHAP4InciaPas encore d'évaluation
- Launching An Employment BlaDocument42 pagesLaunching An Employment BlaInciaPas encore d'évaluation
- Your Current / Preferred Job Title: Career ObjectiveDocument3 pagesYour Current / Preferred Job Title: Career ObjectiveInciaPas encore d'évaluation
- Protean Vs BoundarylessDocument23 pagesProtean Vs BoundarylessInciaPas encore d'évaluation
- Protean vs. Boundaryless CareersDocument15 pagesProtean vs. Boundaryless CareersInciaPas encore d'évaluation
- Course Title: Operations Research Course Supervisor: Syed Ali ImranDocument21 pagesCourse Title: Operations Research Course Supervisor: Syed Ali ImranInciaPas encore d'évaluation
- Individual Development PlanDocument16 pagesIndividual Development PlanInciaPas encore d'évaluation
- Linear Programming ApproachDocument15 pagesLinear Programming ApproachInciaPas encore d'évaluation
- INterview & CV LectDocument31 pagesINterview & CV LectInciaPas encore d'évaluation
- Tax Invoice: Original For RecipientDocument2 pagesTax Invoice: Original For RecipientSubhasis MallikPas encore d'évaluation
- Special Attachment Annual Income Tax Return For Corporate: ResetDocument3 pagesSpecial Attachment Annual Income Tax Return For Corporate: ResetMusi jayaPas encore d'évaluation
- The City of Asher Had The Following Transactions Among OthersDocument1 pageThe City of Asher Had The Following Transactions Among Otherstrilocksp SinghPas encore d'évaluation
- Mouse PadDocument2 pagesMouse Pad20MA32 - PRABAVATHI TPas encore d'évaluation
- Full Jet Powered by Baozun - 2021 China EC Digital ReportDocument12 pagesFull Jet Powered by Baozun - 2021 China EC Digital Reportzackandrian25Pas encore d'évaluation
- 11 MKTG - 104 Product Management-Brand ValuationDocument14 pages11 MKTG - 104 Product Management-Brand ValuationMaynard RolloPas encore d'évaluation
- Shabbir AhmadDocument2 pagesShabbir AhmadEkhlas AmmariPas encore d'évaluation
- UnlockedDocument27 pagesUnlockedSameer DeshmukhPas encore d'évaluation
- Advertisement For Fixed Term Engagement (FTE) - Unfilled VacancyDocument8 pagesAdvertisement For Fixed Term Engagement (FTE) - Unfilled VacancyQBIT bitPas encore d'évaluation
- TWSJ 08062022Document42 pagesTWSJ 08062022Naivedya KatyayanPas encore d'évaluation
- Offer T&C - Domino'sDocument3 pagesOffer T&C - Domino'sSanjiv GargPas encore d'évaluation
- Conept of RetailingDocument13 pagesConept of RetailingAniSh ThapaPas encore d'évaluation
- Answer 1 (1) : The Insolvency and Bankruptcy Code, 2016 Innoventive Industries Ltd. vs. ICICI Bank & Anr (2017) 1 SCC 356Document6 pagesAnswer 1 (1) : The Insolvency and Bankruptcy Code, 2016 Innoventive Industries Ltd. vs. ICICI Bank & Anr (2017) 1 SCC 356Usmaa HashmiPas encore d'évaluation
- Analysis of Financial Performance of Everest Bank LimitedDocument56 pagesAnalysis of Financial Performance of Everest Bank LimitedHima RijalPas encore d'évaluation
- Luxury AssignmentDocument3 pagesLuxury AssignmentMohit NavalkhaPas encore d'évaluation
- Day 1 Audit Report (Day 1)Document31 pagesDay 1 Audit Report (Day 1)Farman Shaikh100% (1)
- Revision Practice PaperDocument10 pagesRevision Practice Paperbehlolahmad7Pas encore d'évaluation
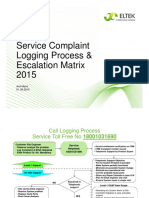
- Eltek Complaint Logging Escalation Matrix-080915Document5 pagesEltek Complaint Logging Escalation Matrix-080915sandeep bhadolaPas encore d'évaluation
- Aarong ProjectDocument29 pagesAarong ProjectIfaz AhmedPas encore d'évaluation
- Taixing Longyi Terminals Co. LTD.: ClarificationDocument9 pagesTaixing Longyi Terminals Co. LTD.: ClarificationMaria Nancy Vásquez LeónPas encore d'évaluation
- D&D 5.0 - Aventura (Nível 7) O Refúgio Perdido Do ArquimagoDocument30 pagesD&D 5.0 - Aventura (Nível 7) O Refúgio Perdido Do ArquimagoMurilo TeixeiraPas encore d'évaluation
- Inventory ManagementDocument15 pagesInventory ManagementAnna Lyssa BatasPas encore d'évaluation
- General Principles of Contracts & Transactions in Islamic PDFDocument19 pagesGeneral Principles of Contracts & Transactions in Islamic PDFMuhammad Ammar100% (1)
- Final MCom Dissertation Lloyd Uta 482059Document126 pagesFinal MCom Dissertation Lloyd Uta 482059Phi BaiPas encore d'évaluation
- Business Communication: RevisionDocument77 pagesBusiness Communication: RevisionTrang TrươngPas encore d'évaluation