Vous aimerez peut-être aussi
- Good Health in the Tropics: Advice to Travellers and SettlersD'EverandGood Health in the Tropics: Advice to Travellers and SettlersPas encore d'évaluation
- Guidelines for African Swine Fever (ASF) prevention and Control in Smallholder Pig Farming in Asia: Culling and Disposal of Pigs in an African Swine Fever OutbreakD'EverandGuidelines for African Swine Fever (ASF) prevention and Control in Smallholder Pig Farming in Asia: Culling and Disposal of Pigs in an African Swine Fever OutbreakPas encore d'évaluation
- WHO 2019 NCov IHR Ship Outbreak 2020Document12 pagesWHO 2019 NCov IHR Ship Outbreak 2020Bheru LalPas encore d'évaluation
- Outbreaks On ShipsDocument12 pagesOutbreaks On ShipscaptkcPas encore d'évaluation
- Standard Operating ProcedureDocument15 pagesStandard Operating ProcedureAyman AliPas encore d'évaluation
- Health and Safety Guidelines Governing The Operations of Mice Organizers and Venues or Facilities Under The New NormalDocument14 pagesHealth and Safety Guidelines Governing The Operations of Mice Organizers and Venues or Facilities Under The New NormalRave PerezPas encore d'évaluation
- EVD WHO Guidance PoE 14.1 EngDocument11 pagesEVD WHO Guidance PoE 14.1 EngAsri RachmawatiPas encore d'évaluation
- 10 Healty Gateways Info For Ships To Prepare For COVID-19 PDFDocument16 pages10 Healty Gateways Info For Ships To Prepare For COVID-19 PDFDennis VolodchenkoPas encore d'évaluation
- RevisedGuidelinesforDialysisofCOVID19Patients PDFDocument8 pagesRevisedGuidelinesforDialysisofCOVID19Patients PDFSaurav KumarPas encore d'évaluation
- RevisedGuidelinesforDialysisofCOVID19Patients PDFDocument8 pagesRevisedGuidelinesforDialysisofCOVID19Patients PDFAmjadali ChoudhariPas encore d'évaluation
- Infection Prevention and Control Guideline For Ports of EntryDocument12 pagesInfection Prevention and Control Guideline For Ports of EntryHareth Al NajriPas encore d'évaluation
- Tanzania - SOPs For Case Management and Infection Prevention and ControlDocument115 pagesTanzania - SOPs For Case Management and Infection Prevention and ControlXuan Nguyen100% (1)
- IPC GUIDELINE Version 2Document20 pagesIPC GUIDELINE Version 2Nrs KhalidPas encore d'évaluation
- 22-10 Health Advisory - Guidance For EMS Professionals On Suspected Cases of MonkeypoxDocument4 pages22-10 Health Advisory - Guidance For EMS Professionals On Suspected Cases of MonkeypoxNorth Country EMSPas encore d'évaluation
- Viral Hemorrhagic Fever Surveillance Protocol: Provider ResponsibilitiesDocument32 pagesViral Hemorrhagic Fever Surveillance Protocol: Provider ResponsibilitiesAmadi OgbondaPas encore d'évaluation
- prehospital-EMS-COVID-19-recommendations - 4.4Document19 pagesprehospital-EMS-COVID-19-recommendations - 4.4MEONEPas encore d'évaluation
- 28june2020 20200628 Guidelines For International Departure From Pakistan 02Document5 pages28june2020 20200628 Guidelines For International Departure From Pakistan 02Ozair MansoorPas encore d'évaluation
- dm2020 0168 PDFDocument4 pagesdm2020 0168 PDFalissalvqs50% (2)
- Guidance For Routine Immunization Services During COVID-19: - PageDocument14 pagesGuidance For Routine Immunization Services During COVID-19: - PagePrisma CahyaPas encore d'évaluation
- 5600 - Updated Interim Guidance For Airlines and Airline Crew - Coronavirus Disease 2019 (COVID-19) - CDCDocument4 pages5600 - Updated Interim Guidance For Airlines and Airline Crew - Coronavirus Disease 2019 (COVID-19) - CDCPutri SyawalPas encore d'évaluation
- An Implementation Guide For The Management of COVID-19 On Board Cargo Ships and Fishing VesselsDocument14 pagesAn Implementation Guide For The Management of COVID-19 On Board Cargo Ships and Fishing VesselsE.Caglar BugraPas encore d'évaluation
- Coronavirus Covid 19 Guidelines For Infection Prevention and Control in Residential Care Facilities - 0Document11 pagesCoronavirus Covid 19 Guidelines For Infection Prevention and Control in Residential Care Facilities - 0Shenelle NashPas encore d'évaluation
- Guia CovidDocument4 pagesGuia CovidAndrés E. Espinoza NolascoPas encore d'évaluation
- DM No. 2020-0063 - Interim Guidelines On The Repatriation of Overseas Filipinos Due To 2019-NCoV ARD - Feb.3, 2020Document6 pagesDM No. 2020-0063 - Interim Guidelines On The Repatriation of Overseas Filipinos Due To 2019-NCoV ARD - Feb.3, 2020Lhota Neilsen DumatogPas encore d'évaluation
- Considerations For Health Screening For COVID-19 at Points of EntryDocument7 pagesConsiderations For Health Screening For COVID-19 at Points of EntryJery JsPas encore d'évaluation
- (COVID-19) Guideline For Airports Is Developed.: 1. Prevention and Control Measure For Passengers During Air TravelDocument8 pages(COVID-19) Guideline For Airports Is Developed.: 1. Prevention and Control Measure For Passengers During Air TravelFouad RatemePas encore d'évaluation
- Issues Related To Kidney Disease and HypertensionDocument12 pagesIssues Related To Kidney Disease and HypertensionCarlos Huaman ZevallosPas encore d'évaluation
- IPC Guidelines For COVID 19Document15 pagesIPC Guidelines For COVID 19Henry OseiPas encore d'évaluation
- DOT MC No. 2020-006 - MICE Organizers and Venues or FacilitiesDocument9 pagesDOT MC No. 2020-006 - MICE Organizers and Venues or FacilitiesMark Kenneth B. CamamaPas encore d'évaluation
- COVID 19 Outpatient DialysisDocument5 pagesCOVID 19 Outpatient DialysisTheala RadistaPas encore d'évaluation
- AssignmentDocument5 pagesAssignmentClaire ChiuPas encore d'évaluation
- Guidance COVID 19Document3 pagesGuidance COVID 19Fitri Najmi NajidPas encore d'évaluation
- WHO EVD Guidance PoE 14.2 EngDocument25 pagesWHO EVD Guidance PoE 14.2 Eng420192420192Pas encore d'évaluation
- Covid ProtocolDocument24 pagesCovid ProtocolFedhii TammiruPas encore d'évaluation
- Office of The Secretary: Temporary TreatmentDocument14 pagesOffice of The Secretary: Temporary TreatmentBenjamin Karlo Delos SantosPas encore d'évaluation
- 2) 09-03-2020 - MOPH Quarantine GuidelinesDocument10 pages2) 09-03-2020 - MOPH Quarantine GuidelinesraghagayuPas encore d'évaluation
- 2019 Novel Coronavirus (COVID-19) : Availability of Personal Protective EquipmentDocument4 pages2019 Novel Coronavirus (COVID-19) : Availability of Personal Protective EquipmentPetroPas encore d'évaluation
- SwineInfluenza InfectioncontrolDocument5 pagesSwineInfluenza InfectioncontrolAbidi HichemPas encore d'évaluation
- Cinema Safety During The COVID-19 Pandemic in The CaribbeanDocument7 pagesCinema Safety During The COVID-19 Pandemic in The CaribbeanNishelle JeffreyPas encore d'évaluation
- Interim Guidance For Healthcare Providers During COVID-19 OutbreakDocument3 pagesInterim Guidance For Healthcare Providers During COVID-19 OutbreakDita Ambarsari SyafruddinPas encore d'évaluation
- Aha RCP CovidDocument3 pagesAha RCP Covidalex zuluagaPas encore d'évaluation
- COVID-19 Preparedness 14apr2020Document13 pagesCOVID-19 Preparedness 14apr2020Andre3893Pas encore d'évaluation
- Standard Operating Procedure For Handling of Corona Virus Disease (Covid-19) PatientsDocument6 pagesStandard Operating Procedure For Handling of Corona Virus Disease (Covid-19) PatientsHiJackPas encore d'évaluation
- WHO 2019 nCoV Policy Brief Risk Based International Travel 2021.1 EngDocument6 pagesWHO 2019 nCoV Policy Brief Risk Based International Travel 2021.1 EngOsama RathorePas encore d'évaluation
- Understanding Recent Coronavirus Outbreak & Prevention TechniquesDocument15 pagesUnderstanding Recent Coronavirus Outbreak & Prevention TechniquesNachikethus NarayanPas encore d'évaluation
- Australia Covid PpeDocument5 pagesAustralia Covid PpeAbidi HichemPas encore d'évaluation
- PAHOPHEIHMCovid1920002 EngDocument5 pagesPAHOPHEIHMCovid1920002 EngfrehanyaqPas encore d'évaluation
- (Document) Covid-19: Voici L'operational Plan Du Ministère de La SantéDocument10 pages(Document) Covid-19: Voici L'operational Plan Du Ministère de La SantéDefimedia50% (2)
- Qso-20-14-Nh - Revised 3-13-2020 PDFDocument6 pagesQso-20-14-Nh - Revised 3-13-2020 PDFAdrian RuxandaPas encore d'évaluation
- Interim Guidance Pediatric Patients March 27 2020Document4 pagesInterim Guidance Pediatric Patients March 27 2020Luis Alberto Anco CórdovaPas encore d'évaluation
- Infection Control and Covid SafetyDocument41 pagesInfection Control and Covid SafetyAdeuga ADEKUOYEPas encore d'évaluation
- SOP Air Ambulance-IsakovDocument6 pagesSOP Air Ambulance-IsakovSankar CdmPas encore d'évaluation
- Who 2019 Ncov Ipc Ppe Use 2020.3 EngDocument28 pagesWho 2019 Ncov Ipc Ppe Use 2020.3 EngKumanan1304Pas encore d'évaluation
- Community Quarantine RecommendationsDocument5 pagesCommunity Quarantine RecommendationsRapplerPas encore d'évaluation
- Temporary Covid-19 Precautions During An Inspection: Vers 1 - 8 June 2020Document5 pagesTemporary Covid-19 Precautions During An Inspection: Vers 1 - 8 June 2020KhaledMazenPas encore d'évaluation
- Covid-19: Guide On Home-Based Care, Screening & Isolation Ward Set UpDocument9 pagesCovid-19: Guide On Home-Based Care, Screening & Isolation Ward Set Upvimalraj vtPas encore d'évaluation
- Principles For COVID-19 Cohorting in Long-Term Care: Key Infection Prevention and Control TermsDocument7 pagesPrinciples For COVID-19 Cohorting in Long-Term Care: Key Infection Prevention and Control TermssimplyrosalynPas encore d'évaluation
- DOT - MC No. 2020-002-ADocument12 pagesDOT - MC No. 2020-002-AMark Kenneth B. CamamaPas encore d'évaluation
- In TRL CEMEX-COVID-19 Construction Site ProtocolsDocument16 pagesIn TRL CEMEX-COVID-19 Construction Site Protocolsevrim korıPas encore d'évaluation
- Standard Precautions: 1.1 Hand HygieneDocument9 pagesStandard Precautions: 1.1 Hand HygieneSandra Ann BijuPas encore d'évaluation
- Homeostasis: Proudly Presents byDocument23 pagesHomeostasis: Proudly Presents byBheru LalPas encore d'évaluation
- CNA LPN Curriculum 11 March 2013Document72 pagesCNA LPN Curriculum 11 March 2013Bheru LalPas encore d'évaluation
- Policy Guidelines For Nursing Education in Pakista - 220418 - 132804Document3 pagesPolicy Guidelines For Nursing Education in Pakista - 220418 - 132804Bheru LalPas encore d'évaluation
- Nutritional Assessment of Children AdmittedDocument8 pagesNutritional Assessment of Children AdmittedBheru LalPas encore d'évaluation
- Nursing Health Assessment: Akram Mohammad Abusalah BNS, MSN, Ph. D. Islamic University of Gaza StripDocument262 pagesNursing Health Assessment: Akram Mohammad Abusalah BNS, MSN, Ph. D. Islamic University of Gaza StripBheru LalPas encore d'évaluation
- Intestinal ObstructionDocument12 pagesIntestinal ObstructionBheru LalPas encore d'évaluation
- CH 8 Digestive System: StructuresDocument18 pagesCH 8 Digestive System: StructuresBheru LalPas encore d'évaluation
- Intestinal ObstructionDocument21 pagesIntestinal ObstructionBheru LalPas encore d'évaluation
- Intestinal Obstruction: Dr. Mohammad Jamil AlhashlamonDocument19 pagesIntestinal Obstruction: Dr. Mohammad Jamil AlhashlamonBheru LalPas encore d'évaluation
- Assessment and Management of Patients With Biliary DisordersDocument18 pagesAssessment and Management of Patients With Biliary DisordersBheru LalPas encore d'évaluation
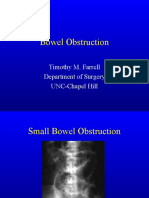
- Bowel Obstruction: Timothy M. Farrell Department of Surgery UNC-Chapel HillDocument27 pagesBowel Obstruction: Timothy M. Farrell Department of Surgery UNC-Chapel HillBheru LalPas encore d'évaluation
- NEET MCQs ON COVID - 19Document3 pagesNEET MCQs ON COVID - 19Abid KaziPas encore d'évaluation
- Malaria 8Document35 pagesMalaria 8Fuad Nasir 0913Pas encore d'évaluation
- Urology and Urinary Tract InfectionsDocument15 pagesUrology and Urinary Tract InfectionsMonica CiorneiPas encore d'évaluation
- PNLE IV For Psychiatric NursingDocument10 pagesPNLE IV For Psychiatric NursingASDF ASDF100% (1)
- Test Bank For Brunner and Suddarths Textbook of Medical Surgical Nursing 12th Edition Suzanne C Smeltzer 2Document27 pagesTest Bank For Brunner and Suddarths Textbook of Medical Surgical Nursing 12th Edition Suzanne C Smeltzer 2amandawrightrwfdcombka100% (33)
- Onychomycosis: An Updated Review: Recent Patents On Inflammation & Allergy Drug Discovery October 2019Document15 pagesOnychomycosis: An Updated Review: Recent Patents On Inflammation & Allergy Drug Discovery October 2019jungHAENAPas encore d'évaluation
- Perinatology: Journal of Perinatal and Neonatal CareDocument56 pagesPerinatology: Journal of Perinatal and Neonatal CareSayed Fareed HasanPas encore d'évaluation
- Case P On Lung AbscessDocument20 pagesCase P On Lung AbscessanShUl 002100% (1)
- Human Health and Diseases Imp QuestionsDocument21 pagesHuman Health and Diseases Imp QuestionsMadhumathi SSPas encore d'évaluation
- leptospirosis钩体Document29 pagesleptospirosis钩体russonegroPas encore d'évaluation
- ONCOLOGY Post TestDocument5 pagesONCOLOGY Post TestmycovesmanePas encore d'évaluation
- Hurt and Grievous HurtDocument8 pagesHurt and Grievous HurtVaishnavi PandeyPas encore d'évaluation
- Learning FeedbackDocument2 pagesLearning FeedbackDeejay L. RaramaPas encore d'évaluation
- Organ System PDFDocument73 pagesOrgan System PDFbae joohyunPas encore d'évaluation
- 4c Aguilar Gasmen Quitoriano Rabena Valeros Viado VillalobosDocument19 pages4c Aguilar Gasmen Quitoriano Rabena Valeros Viado VillalobosBitz Basos ViadoPas encore d'évaluation
- Cell Therapy For HIV: Investigatory Project byDocument18 pagesCell Therapy For HIV: Investigatory Project byAthiya ZainabPas encore d'évaluation
- Case 2-1-1Document11 pagesCase 2-1-1Shakshi RainaPas encore d'évaluation
- Acute Upper Airway Obstruction in Children: Paediatric Anaesthesia Tutorial 368Document9 pagesAcute Upper Airway Obstruction in Children: Paediatric Anaesthesia Tutorial 368Fireka JuniantikaPas encore d'évaluation
- Dialog AnamnesisDocument2 pagesDialog AnamnesisMona Ahmd100% (1)
- Assessment of The Thorax and Lungs 2014Document9 pagesAssessment of The Thorax and Lungs 2014alphabennydelta4468Pas encore d'évaluation
- 11-Acid-Base BalanceDocument28 pages11-Acid-Base BalanceKathlene BarasiPas encore d'évaluation
- ENT DiseasesDocument75 pagesENT DiseasesGudeta shegerPas encore d'évaluation
- Chhabhadiya Laxman (Ent)Document7 pagesChhabhadiya Laxman (Ent)Venkatesh GarikapatiPas encore d'évaluation
- Bu Erger 'S Disea Se OR Thromboan Gitis Obliter An S (TAO) : DR Bhupendra Chouhan Assistant ProfessorDocument19 pagesBu Erger 'S Disea Se OR Thromboan Gitis Obliter An S (TAO) : DR Bhupendra Chouhan Assistant ProfessorAnupam MantriPas encore d'évaluation
- Wksiteposter - en OSHADocument1 pageWksiteposter - en OSHARaúlPas encore d'évaluation
- Malaria 1Document24 pagesMalaria 1Jamuna PatelPas encore d'évaluation
- COVID-19 - Evidence Over Hysteria - Zero HedgeDocument38 pagesCOVID-19 - Evidence Over Hysteria - Zero HedgeFabiana BPas encore d'évaluation
- Slide Materi Dr. Mita, SPKFR - Foot Abnormalities in Children - PMR4GP 2022Document46 pagesSlide Materi Dr. Mita, SPKFR - Foot Abnormalities in Children - PMR4GP 2022LitaPas encore d'évaluation
- Articulos Finales Gastro PDFDocument41 pagesArticulos Finales Gastro PDFGabii RodasPas encore d'évaluation
- IDB Assessment Tool (Questionnaire)Document7 pagesIDB Assessment Tool (Questionnaire)Somcio, Denise Grazelle Anne P.Pas encore d'évaluation