Vous aimerez peut-être aussi
- Fibromyalgia: Understanding, managing, and improving Fibromyalgia and its signs and symptoms!D'EverandFibromyalgia: Understanding, managing, and improving Fibromyalgia and its signs and symptoms!Pas encore d'évaluation
- 01 Pathophysiology of PainDocument3 pages01 Pathophysiology of PainBani ZakiyahPas encore d'évaluation
- Reviews: Fibromyalgia: From Pathophysiology To TherapyDocument10 pagesReviews: Fibromyalgia: From Pathophysiology To TherapyCriss RodriguezPas encore d'évaluation
- Fibromyalgia Clinical Features, Diagnosis and Management (2016) PDFDocument13 pagesFibromyalgia Clinical Features, Diagnosis and Management (2016) PDFBecados PsiquiatriaPas encore d'évaluation
- Neurofeedback For Pain Management A Systematic ReviewDocument22 pagesNeurofeedback For Pain Management A Systematic ReviewLevente BalázsPas encore d'évaluation
- CCJM Essential Tremor Choosing The Right Management Plan For Your PatientDocument8 pagesCCJM Essential Tremor Choosing The Right Management Plan For Your PatientBrian HarrisPas encore d'évaluation
- Keywords Joint PainDocument10 pagesKeywords Joint PainMayank JhaPas encore d'évaluation
- Drug Free Nutrition For Brain ImbalancesDocument41 pagesDrug Free Nutrition For Brain ImbalancesricardfelipePas encore d'évaluation
- Combined Nutcracker and Ehlers-Danlos Syndromes: A Case ReportDocument6 pagesCombined Nutcracker and Ehlers-Danlos Syndromes: A Case ReportAlexandre Campos Moraes AmatoPas encore d'évaluation
- Messages From The Body Book Index 2016Document29 pagesMessages From The Body Book Index 2016ap0% (1)
- Measureable Changes in The Neuro-Endocrinal Mechanism Following Spinal Manipulation - 2015Document6 pagesMeasureable Changes in The Neuro-Endocrinal Mechanism Following Spinal Manipulation - 2015Renan O. Pravatta PivettaPas encore d'évaluation
- Inflammation and HealingDocument15 pagesInflammation and HealingRachel Niu II100% (1)
- Guidelines PDFDocument37 pagesGuidelines PDFNicole Amanda Nieto QuiñonezPas encore d'évaluation
- MFTB Intro 2019 PDF NewDocument6 pagesMFTB Intro 2019 PDF Newap100% (1)
- The Cervical Spine and Sensorimotor ControlDocument10 pagesThe Cervical Spine and Sensorimotor Controlpuchio100% (1)
- Brietzke Fibromyalgia 2019Document39 pagesBrietzke Fibromyalgia 2019jem bistrePas encore d'évaluation
- Phrenic Nerve DamageDocument15 pagesPhrenic Nerve DamageIzza Mae Ferrancol PastranaPas encore d'évaluation
- PainDocument10 pagesPainBrian S. OlajePas encore d'évaluation
- Lymphatic Rescue Summit 2022 Day 1Document4 pagesLymphatic Rescue Summit 2022 Day 1Paul Ioan PopescuPas encore d'évaluation
- Understanding Self Components of Self Self Concept Self Confidence Self Image Sabnam BasuDocument28 pagesUnderstanding Self Components of Self Self Concept Self Confidence Self Image Sabnam BasuRoldan Dela CruzPas encore d'évaluation
- Vitamins, Supplements, Herbal Medicines, and ArrhythmiasDocument12 pagesVitamins, Supplements, Herbal Medicines, and ArrhythmiashyntnenPas encore d'évaluation
- The Effects of Music On Chronic Pain: Oula VaaralaDocument33 pagesThe Effects of Music On Chronic Pain: Oula Vaaralacam1000Pas encore d'évaluation
- Differential Release of Mast Cell Mediators and The Pathogenesis of InflammationDocument14 pagesDifferential Release of Mast Cell Mediators and The Pathogenesis of InflammationklaumrdPas encore d'évaluation
- Intellectual Wellness - Group 1Document10 pagesIntellectual Wellness - Group 1Psi-J BacolodPas encore d'évaluation
- Rheumatoid Arthritis "An Autoimmune Mystery"Document23 pagesRheumatoid Arthritis "An Autoimmune Mystery"Manisanthosh KumarPas encore d'évaluation
- Brainchange: Grea T D Oor ChinaDocument4 pagesBrainchange: Grea T D Oor ChinaJack CarneyPas encore d'évaluation
- Shiatsu & Back ProblemDocument33 pagesShiatsu & Back ProblemlaukunePas encore d'évaluation
- Chronic Psoas Syndrome Caused by The Inappropriate Use of A Heel Lift PDFDocument4 pagesChronic Psoas Syndrome Caused by The Inappropriate Use of A Heel Lift PDFTito AlhoPas encore d'évaluation
- Fibromyalgia PDFDocument10 pagesFibromyalgia PDFRuan VerzosaPas encore d'évaluation
- Motor Imagery and MirrorTherapyDocument5 pagesMotor Imagery and MirrorTherapyLorenaMariaPas encore d'évaluation
- Holistic Healthcare For Transgender and Gender Variant Folks - Dori MidnightDocument17 pagesHolistic Healthcare For Transgender and Gender Variant Folks - Dori Midnightpille83100% (1)
- PDF VersionDocument6 pagesPDF Versionservicesmi123100% (1)
- Fibromyalgia and Cognitive Behavioral TherapyDocument2 pagesFibromyalgia and Cognitive Behavioral TherapyАлексPas encore d'évaluation
- Understanding The Stress Response - Harvard HealthDocument3 pagesUnderstanding The Stress Response - Harvard HealthCarlos Vidal WittPas encore d'évaluation
- Facet Joint SyndromeDocument17 pagesFacet Joint Syndromepaulvaso27100% (1)
- Neurogenic BowlDocument21 pagesNeurogenic BowlFaridatul IsniyahPas encore d'évaluation
- Fibromyalgia and Myofascial PainDocument33 pagesFibromyalgia and Myofascial Painlichugojavier100% (1)
- Disease Activity Scoring in RheumatologyDocument28 pagesDisease Activity Scoring in RheumatologyLeo FluxPas encore d'évaluation
- MYOFASCIAL Resources Sheet 2017Document2 pagesMYOFASCIAL Resources Sheet 2017pbi tvPas encore d'évaluation
- Degenerative Joint DiseaseDocument35 pagesDegenerative Joint DiseaseWendy EscalantePas encore d'évaluation
- Fatigue (Medical)Document9 pagesFatigue (Medical)Wira SentanuPas encore d'évaluation
- Lesions of Upper Motor Neurons and Lower Motor NeuronsDocument9 pagesLesions of Upper Motor Neurons and Lower Motor NeuronsAdhitya Rama Jr.Pas encore d'évaluation
- What Is A Migraine Headache - CourseDocument14 pagesWhat Is A Migraine Headache - CourseKARL PASCUAPas encore d'évaluation
- Mechanism of Pain and Pain Management: Questions ANSWERS and Rationale ReferencesDocument23 pagesMechanism of Pain and Pain Management: Questions ANSWERS and Rationale ReferencesAngela Nicole LaredoPas encore d'évaluation
- Curable Meditation LessonDocument22 pagesCurable Meditation LessonSandra KhanPas encore d'évaluation
- Skin PhysiotherapyDocument6 pagesSkin PhysiotherapyPavan Vivek RajPas encore d'évaluation
- Fibromyalgia Impact Questionnaire (Fiq) : DirectionsDocument4 pagesFibromyalgia Impact Questionnaire (Fiq) : Directionsece142Pas encore d'évaluation
- Japanese Lymphedema TreatmentDocument4 pagesJapanese Lymphedema TreatmentLou L MontoyaPas encore d'évaluation
- Disorders of The Cerebellum or The Posterior Columns of The Spinal Cord May Involve The Limbs, Head, or TrunkDocument5 pagesDisorders of The Cerebellum or The Posterior Columns of The Spinal Cord May Involve The Limbs, Head, or TrunkNaina Karamina Sakina100% (1)
- What Is PolymyositisDocument24 pagesWhat Is PolymyositisAshraf MobyPas encore d'évaluation
- Recovering After A StrokeDocument17 pagesRecovering After A StrokeTiffany MatthewsPas encore d'évaluation
- FibromyalgiaDocument1 pageFibromyalgiashailesh284100% (1)
- Brochure Stretching For People With MS An Illustrated ManualDocument32 pagesBrochure Stretching For People With MS An Illustrated ManualAnonymous Ak60ysM7qEPas encore d'évaluation
- Drugs For Osteoarthritis Revise 2010Document65 pagesDrugs For Osteoarthritis Revise 2010Nofilia Citra CandraPas encore d'évaluation
- Psoriatic ArthritisDocument33 pagesPsoriatic Arthritisini_etuk100% (1)
- Shock Wave Therapy - DosageDocument4 pagesShock Wave Therapy - DosageAniesa Nur Laily PertiwiPas encore d'évaluation
- High Voltage Galvanic StimulationDocument4 pagesHigh Voltage Galvanic StimulationmichidoodlePas encore d'évaluation
- Iliopsoas Syndrome - The Hidden Root of PainDocument13 pagesIliopsoas Syndrome - The Hidden Root of Painpeter1234u0% (1)
- Center For Integrative MedicineDocument45 pagesCenter For Integrative MedicineJaypee EnteresoPas encore d'évaluation
- Peripheral Neuropathy BreakthroughDocument4 pagesPeripheral Neuropathy BreakthroughMavrick802100% (3)
- KissPrep-Anatomy Physiology PDFDocument1 pageKissPrep-Anatomy Physiology PDFVon HippoPas encore d'évaluation
- Joint and Connective Tissue Disorders: QuestionsDocument11 pagesJoint and Connective Tissue Disorders: QuestionsVon HippoPas encore d'évaluation
- Gyne 2.6 - Benign and Malignant Tumors of The Ovaries and Fallopian TubesDocument8 pagesGyne 2.6 - Benign and Malignant Tumors of The Ovaries and Fallopian TubesVon HippoPas encore d'évaluation
- Diagnostic Performance of International Ovarian Tumor Analysis IotaDocument7 pagesDiagnostic Performance of International Ovarian Tumor Analysis IotaVon HippoPas encore d'évaluation
- Adnexal Mass in Pregnancy UpToDate PDFDocument21 pagesAdnexal Mass in Pregnancy UpToDate PDFVon HippoPas encore d'évaluation
- Leptospirosis Policy StatementsDocument6 pagesLeptospirosis Policy StatementsKay RuzPas encore d'évaluation
- Psychiatric EmergencyDocument3 pagesPsychiatric EmergencyVon HippoPas encore d'évaluation
- Psychiatric 3: Suicide (DR Rosales) June 8, 2011Document4 pagesPsychiatric 3: Suicide (DR Rosales) June 8, 2011Von HippoPas encore d'évaluation
- Urinary Tract Infection (Book) : NephrologyDocument4 pagesUrinary Tract Infection (Book) : NephrologyVon HippoPas encore d'évaluation
- Psychiatric 3: Suicide (DR Rosales) June 8, 2011Document4 pagesPsychiatric 3: Suicide (DR Rosales) June 8, 2011Von HippoPas encore d'évaluation
- Suicide, Psychiatric Emergency, Substance Abuse PDFDocument14 pagesSuicide, Psychiatric Emergency, Substance Abuse PDFVon HippoPas encore d'évaluation
- Ob Gyne PDFDocument27 pagesOb Gyne PDFVon HippoPas encore d'évaluation
- Psychopharmacology-Mood StabilizerDocument5 pagesPsychopharmacology-Mood StabilizerVon Hippo100% (1)
- Psychiatric 3: Substance Abuse (DR Rosales) : Substance Use Related DisordersDocument11 pagesPsychiatric 3: Substance Abuse (DR Rosales) : Substance Use Related DisordersVon HippoPas encore d'évaluation
- Abdominal: Al HerniaDocument3 pagesAbdominal: Al HerniaVon Hippo100% (1)
- Adult Emergency PDFDocument2 pagesAdult Emergency PDFVon HippoPas encore d'évaluation
- Child PsychiatryDocument6 pagesChild PsychiatryVon HippoPas encore d'évaluation
- Motor System: Three Types of Movement Generated by Motor SystemDocument10 pagesMotor System: Three Types of Movement Generated by Motor SystemVon Hippo100% (1)
- Recalls: 2nd Shifting ExamDocument13 pagesRecalls: 2nd Shifting ExamVon HippoPas encore d'évaluation
- CLINPATH Finals ReviewerDocument28 pagesCLINPATH Finals ReviewerVon HippoPas encore d'évaluation
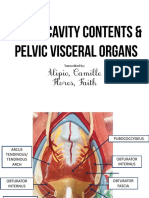
- Alipio, Camille Flores, Faith: Transcribed byDocument7 pagesAlipio, Camille Flores, Faith: Transcribed byVon HippoPas encore d'évaluation
- Vitamins B ComplexDocument4 pagesVitamins B ComplexVon HippoPas encore d'évaluation
- Patho B Prelims RBCDocument12 pagesPatho B Prelims RBCVon HippoPas encore d'évaluation
- PEDIA2 2.01b Fluids Electrolytes Summary TablesDocument4 pagesPEDIA2 2.01b Fluids Electrolytes Summary TablesVon HippoPas encore d'évaluation
- 1) Any Medical Student or GraduateDocument27 pages1) Any Medical Student or GraduateVon HippoPas encore d'évaluation
- Gold 2019 Pocket Guide Final WmsDocument49 pagesGold 2019 Pocket Guide Final WmsFrensi Ayu PrimantariPas encore d'évaluation
- Brainstem Lesions Trans 2019 PDFDocument8 pagesBrainstem Lesions Trans 2019 PDFVon HippoPas encore d'évaluation
- Book: - RecordingDocument8 pagesBook: - RecordingVon HippoPas encore d'évaluation
- Fluid and Electrolytes YMDocument8 pagesFluid and Electrolytes YMVon HippoPas encore d'évaluation
- Clinical Scenario: CPT Case 9 Neonatal SepsisDocument15 pagesClinical Scenario: CPT Case 9 Neonatal SepsisVon HippoPas encore d'évaluation
- Cacioppo Chapter 5Document16 pagesCacioppo Chapter 5Anonymous 7CxwuBUJz3Pas encore d'évaluation
- Hip Fracture Concept MapDocument2 pagesHip Fracture Concept MapPriyal ParikhPas encore d'évaluation
- Natural Therapies Overview Report FinalDocument188 pagesNatural Therapies Overview Report FinalLucas GallindoPas encore d'évaluation
- Medidor de Impedancia de PielDocument5 pagesMedidor de Impedancia de PielmagragirenaPas encore d'évaluation
- Pathologic Basis of Lumbar Radicular Pain: BackgroundDocument8 pagesPathologic Basis of Lumbar Radicular Pain: BackgroundVizaPas encore d'évaluation
- Chelt TherapyDocument2 pagesChelt TherapymatameaPas encore d'évaluation
- "It Was An Emotional Rollercoaster": Kim LyonsDocument1 page"It Was An Emotional Rollercoaster": Kim LyonsditeABCPas encore d'évaluation
- Ekdahl 2010Document8 pagesEkdahl 2010ika kurniawatiPas encore d'évaluation
- Chapter 3 Part of BodyDocument12 pagesChapter 3 Part of BodyYunita AmaralPas encore d'évaluation
- Interferential TherapyDocument9 pagesInterferential TherapyEldar SulejmanovicPas encore d'évaluation
- Application of Finger Gymnastics For Retraining and Refining PianDocument100 pagesApplication of Finger Gymnastics For Retraining and Refining PianJose Ramon Rodriguez Ures100% (3)
- (ACC ENGLISH) ASKEP HiperglikemiaDocument11 pages(ACC ENGLISH) ASKEP HiperglikemiaWenPas encore d'évaluation
- Group 4 - Analgesics Structure SchoolDocument5 pagesGroup 4 - Analgesics Structure Schoolliezel_798041921Pas encore d'évaluation
- MARY KURUS - Psychic Attacks and Protecting YourselfDocument12 pagesMARY KURUS - Psychic Attacks and Protecting YourselfOpusnigruMPas encore d'évaluation
- There Are Different Types of PainDocument2 pagesThere Are Different Types of PainMary Scarlette CenaPas encore d'évaluation
- NCP For IHDDocument19 pagesNCP For IHDMasyitah Farahin100% (2)
- Eim4 V 02 WorksheetDocument1 pageEim4 V 02 WorksheetSamantha LanePas encore d'évaluation
- Adaptive QuizzingDocument166 pagesAdaptive QuizzingHuawei Li100% (1)
- Drug StudyDocument17 pagesDrug StudyChairperson Celine Abaya SiquianPas encore d'évaluation
- Nursing Care Plan: Assessmen T (Cues / Clues) Nursing Diagnosis Rationale Planning Intervention Rationale Evaluatio NDocument7 pagesNursing Care Plan: Assessmen T (Cues / Clues) Nursing Diagnosis Rationale Planning Intervention Rationale Evaluatio NNajla Kaye PerezPas encore d'évaluation
- Physiotherapy Catalogue PDFDocument49 pagesPhysiotherapy Catalogue PDFUMARALEKSANA, CV100% (1)
- RESUMEN POSTERS - ACBS Annual World Conference 13 (Berlín, 2015)Document138 pagesRESUMEN POSTERS - ACBS Annual World Conference 13 (Berlín, 2015)LandoGuillénChávezPas encore d'évaluation
- KaufmanDocument2 pagesKaufmanrbtakemotoPas encore d'évaluation
- VryfomDocument278 pagesVryfomJoni BobiPas encore d'évaluation
- History TakingDocument4 pagesHistory TakingChristopher WuPas encore d'évaluation
- ICD 10 MyalgiaDocument4 pagesICD 10 MyalgiaSuhana AnaPas encore d'évaluation
- Pascas Care Cure by CryingDocument92 pagesPascas Care Cure by CryingfrostssssPas encore d'évaluation
- Anesthetics and Anesthesiology: Effect of Opioid-Free Anaesthesia On Perioperative Period: A ReviewDocument11 pagesAnesthetics and Anesthesiology: Effect of Opioid-Free Anaesthesia On Perioperative Period: A Reviewveranisa suciaPas encore d'évaluation
- Odt20150506 DLDocument70 pagesOdt20150506 DLcody bossPas encore d'évaluation
- Determining Relationships Between Physical Health and Spiritual Experience, Religious Practices, and Congregational Support in A Heterogeneous Medical SampleDocument15 pagesDetermining Relationships Between Physical Health and Spiritual Experience, Religious Practices, and Congregational Support in A Heterogeneous Medical Samplemr_merlinPas encore d'évaluation
- The Obesity Code: Unlocking the Secrets of Weight LossD'EverandThe Obesity Code: Unlocking the Secrets of Weight LossÉvaluation : 4 sur 5 étoiles4/5 (6)
- By the Time You Read This: The Space between Cheslie's Smile and Mental Illness—Her Story in Her Own WordsD'EverandBy the Time You Read This: The Space between Cheslie's Smile and Mental Illness—Her Story in Her Own WordsPas encore d'évaluation
- Think This, Not That: 12 Mindshifts to Breakthrough Limiting Beliefs and Become Who You Were Born to BeD'EverandThink This, Not That: 12 Mindshifts to Breakthrough Limiting Beliefs and Become Who You Were Born to BeÉvaluation : 2 sur 5 étoiles2/5 (1)
- The Age of Magical Overthinking: Notes on Modern IrrationalityD'EverandThe Age of Magical Overthinking: Notes on Modern IrrationalityÉvaluation : 4 sur 5 étoiles4/5 (24)
- The Body Keeps the Score by Bessel Van der Kolk, M.D. - Book Summary: Brain, Mind, and Body in the Healing of TraumaD'EverandThe Body Keeps the Score by Bessel Van der Kolk, M.D. - Book Summary: Brain, Mind, and Body in the Healing of TraumaÉvaluation : 4.5 sur 5 étoiles4.5/5 (266)
- Summary: Outlive: The Science and Art of Longevity by Peter Attia MD, With Bill Gifford: Key Takeaways, Summary & AnalysisD'EverandSummary: Outlive: The Science and Art of Longevity by Peter Attia MD, With Bill Gifford: Key Takeaways, Summary & AnalysisÉvaluation : 4.5 sur 5 étoiles4.5/5 (42)
- Summary: The Psychology of Money: Timeless Lessons on Wealth, Greed, and Happiness by Morgan Housel: Key Takeaways, Summary & Analysis IncludedD'EverandSummary: The Psychology of Money: Timeless Lessons on Wealth, Greed, and Happiness by Morgan Housel: Key Takeaways, Summary & Analysis IncludedÉvaluation : 5 sur 5 étoiles5/5 (80)
- ADHD is Awesome: A Guide to (Mostly) Thriving with ADHDD'EverandADHD is Awesome: A Guide to (Mostly) Thriving with ADHDÉvaluation : 5 sur 5 étoiles5/5 (1)
- Self-Care for Autistic People: 100+ Ways to Recharge, De-Stress, and Unmask!D'EverandSelf-Care for Autistic People: 100+ Ways to Recharge, De-Stress, and Unmask!Évaluation : 5 sur 5 étoiles5/5 (1)
- Raising Mentally Strong Kids: How to Combine the Power of Neuroscience with Love and Logic to Grow Confident, Kind, Responsible, and Resilient Children and Young AdultsD'EverandRaising Mentally Strong Kids: How to Combine the Power of Neuroscience with Love and Logic to Grow Confident, Kind, Responsible, and Resilient Children and Young AdultsÉvaluation : 5 sur 5 étoiles5/5 (1)
- Outlive: The Science and Art of Longevity by Peter Attia: Key Takeaways, Summary & AnalysisD'EverandOutlive: The Science and Art of Longevity by Peter Attia: Key Takeaways, Summary & AnalysisÉvaluation : 4 sur 5 étoiles4/5 (1)
- The Comfort of Crows: A Backyard YearD'EverandThe Comfort of Crows: A Backyard YearÉvaluation : 4.5 sur 5 étoiles4.5/5 (23)
- Dark Psychology & Manipulation: Discover How To Analyze People and Master Human Behaviour Using Emotional Influence Techniques, Body Language Secrets, Covert NLP, Speed Reading, and Hypnosis.D'EverandDark Psychology & Manipulation: Discover How To Analyze People and Master Human Behaviour Using Emotional Influence Techniques, Body Language Secrets, Covert NLP, Speed Reading, and Hypnosis.Évaluation : 4.5 sur 5 étoiles4.5/5 (110)
- Gut: the new and revised Sunday Times bestsellerD'EverandGut: the new and revised Sunday Times bestsellerÉvaluation : 4 sur 5 étoiles4/5 (392)
- Why We Die: The New Science of Aging and the Quest for ImmortalityD'EverandWhy We Die: The New Science of Aging and the Quest for ImmortalityÉvaluation : 4 sur 5 étoiles4/5 (3)
- Raising Good Humans: A Mindful Guide to Breaking the Cycle of Reactive Parenting and Raising Kind, Confident KidsD'EverandRaising Good Humans: A Mindful Guide to Breaking the Cycle of Reactive Parenting and Raising Kind, Confident KidsÉvaluation : 4.5 sur 5 étoiles4.5/5 (169)
- Cult, A Love Story: Ten Years Inside a Canadian Cult and the Subsequent Long Road of RecoveryD'EverandCult, A Love Story: Ten Years Inside a Canadian Cult and the Subsequent Long Road of RecoveryÉvaluation : 4 sur 5 étoiles4/5 (44)
- Mindset by Carol S. Dweck - Book Summary: The New Psychology of SuccessD'EverandMindset by Carol S. Dweck - Book Summary: The New Psychology of SuccessÉvaluation : 4.5 sur 5 étoiles4.5/5 (328)
- The Ritual Effect: From Habit to Ritual, Harness the Surprising Power of Everyday ActionsD'EverandThe Ritual Effect: From Habit to Ritual, Harness the Surprising Power of Everyday ActionsÉvaluation : 3.5 sur 5 étoiles3.5/5 (3)
- When the Body Says No by Gabor Maté: Key Takeaways, Summary & AnalysisD'EverandWhen the Body Says No by Gabor Maté: Key Takeaways, Summary & AnalysisÉvaluation : 3.5 sur 5 étoiles3.5/5 (2)
- Sleep Stories for Adults: Overcome Insomnia and Find a Peaceful AwakeningD'EverandSleep Stories for Adults: Overcome Insomnia and Find a Peaceful AwakeningÉvaluation : 4 sur 5 étoiles4/5 (3)
- Gut: The Inside Story of Our Body's Most Underrated Organ (Revised Edition)D'EverandGut: The Inside Story of Our Body's Most Underrated Organ (Revised Edition)Évaluation : 4 sur 5 étoiles4/5 (378)
- To Explain the World: The Discovery of Modern ScienceD'EverandTo Explain the World: The Discovery of Modern ScienceÉvaluation : 3.5 sur 5 étoiles3.5/5 (51)
- The Marshmallow Test: Mastering Self-ControlD'EverandThe Marshmallow Test: Mastering Self-ControlÉvaluation : 4.5 sur 5 étoiles4.5/5 (58)