Vous aimerez peut-être aussi
- Hearing: Anatomy, Physiology, and Disorders of the Auditory SystemD'EverandHearing: Anatomy, Physiology, and Disorders of the Auditory SystemPas encore d'évaluation
- Rehabilitation of AmputeeDocument17 pagesRehabilitation of AmputeeMohamed Hamani100% (2)
- Quadrilatral and Ischial SocketDocument133 pagesQuadrilatral and Ischial Socketjay prakashPas encore d'évaluation
- Amputation Manual 1Document34 pagesAmputation Manual 1Eldar Sulejmanovic100% (1)
- Complications of Bed RestDocument51 pagesComplications of Bed Restsuderson100% (1)
- Peripheral Nerve DisordersDocument33 pagesPeripheral Nerve Disordersbpt2Pas encore d'évaluation
- Nerve Conduction Velocity: Karunakaran K MPT (Neuro) ., PGDMT Associate Professor, SvcoptDocument30 pagesNerve Conduction Velocity: Karunakaran K MPT (Neuro) ., PGDMT Associate Professor, SvcoptSineka 19170239Pas encore d'évaluation
- Knee Ankle Foot OrthosisDocument35 pagesKnee Ankle Foot OrthosisMaryam KhalidPas encore d'évaluation
- 1533 The Dysphagia Toolbox Validated Assessment Tools For Dysphagia in AdultsDocument33 pages1533 The Dysphagia Toolbox Validated Assessment Tools For Dysphagia in AdultsAlvaro Martinez TorresPas encore d'évaluation
- Post Operative and Pre Prosthetic ManagementDocument38 pagesPost Operative and Pre Prosthetic ManagementTanzeelah RajawPas encore d'évaluation
- Above Knee Amputee Amputee Case StudyDocument4 pagesAbove Knee Amputee Amputee Case StudyPhysiotherapist AliPas encore d'évaluation
- Common Spinal Disorders Explained PDFDocument2 pagesCommon Spinal Disorders Explained PDFTamekaPas encore d'évaluation
- Quiz #2 - Chapters 5 and 6: The Thorax and Chest Wall TemporomandibularDocument3 pagesQuiz #2 - Chapters 5 and 6: The Thorax and Chest Wall TemporomandibularJoan Rae TanPas encore d'évaluation
- RS2480 Amputation 2018Document49 pagesRS2480 Amputation 2018Hung Sarah100% (1)
- Rehabilitation Engineering Fact Sheet PDFDocument2 pagesRehabilitation Engineering Fact Sheet PDFYahya AlkamaliPas encore d'évaluation
- Biomechanics of Peripheral and Spinal Nerve RootsDocument86 pagesBiomechanics of Peripheral and Spinal Nerve RootsJawad HassanPas encore d'évaluation
- Effects of Impairment Based Individual and Socially Oriented Group Therapies On Verb Production in AphasiaDocument19 pagesEffects of Impairment Based Individual and Socially Oriented Group Therapies On Verb Production in AphasiaConcepcion NeulingPas encore d'évaluation
- Blount Disease - ASADocument26 pagesBlount Disease - ASAMulya ImansyahPas encore d'évaluation
- Bronchiectasis Pa Tho Physiology, Presentation and ManagementDocument8 pagesBronchiectasis Pa Tho Physiology, Presentation and ManagementCristhian MellaPas encore d'évaluation
- Chapter 10 - Trigeminal NeuralgiaDocument5 pagesChapter 10 - Trigeminal NeuralgiaMuhammad IkbarPas encore d'évaluation
- ProsthesisDocument13 pagesProsthesisDhruv Aneja100% (2)
- Sensory Motor Approaches: Brunstrom TheoryDocument32 pagesSensory Motor Approaches: Brunstrom TheoryAsaad JawedPas encore d'évaluation
- 4 - Therapeutic Effects of Low Frequency Currents On TissuesIVDocument52 pages4 - Therapeutic Effects of Low Frequency Currents On TissuesIVhuxley2378Pas encore d'évaluation
- Introduction To Functional Electrical StimulationDocument14 pagesIntroduction To Functional Electrical StimulationJia HuiPas encore d'évaluation
- Malignant Otitis ExternaDocument5 pagesMalignant Otitis Externasergeantchai068Pas encore d'évaluation
- Neurological Manifestations of Vascular DementiaDocument5 pagesNeurological Manifestations of Vascular DementiaDumitruAuraPas encore d'évaluation
- Cerebellum: Principally Because Electrical Excitation of The CerebellumDocument42 pagesCerebellum: Principally Because Electrical Excitation of The Cerebellumdr_mksinhaPas encore d'évaluation
- Histology - Epithelial TissuesDocument4 pagesHistology - Epithelial TissuesKrissa OmandamPas encore d'évaluation
- Clinical Exercise PhysiologyDocument44 pagesClinical Exercise Physiologymsimoes29Pas encore d'évaluation
- FES (Functional Electrical Stimulation)Document38 pagesFES (Functional Electrical Stimulation)Nivetha RavikumarPas encore d'évaluation
- Practical Skills On PalpationDocument6 pagesPractical Skills On PalpationsudersonPas encore d'évaluation
- Neuromuscular Electrical Stimulation (NMES)Document55 pagesNeuromuscular Electrical Stimulation (NMES)Dr NehaPas encore d'évaluation
- Clinical Biomechanics of Gait: OutlineDocument7 pagesClinical Biomechanics of Gait: Outlinechacho1971100% (1)
- Management Head Injury in ICUDocument5 pagesManagement Head Injury in ICUIrma KusumaPas encore d'évaluation
- Physio Shacklock 95Document8 pagesPhysio Shacklock 95Raihan HabibPas encore d'évaluation
- Biomechanics HipDocument35 pagesBiomechanics Hipkhyber kmcPas encore d'évaluation
- Cervical PalpationDocument22 pagesCervical Palpationpraveen100% (12)
- Physical Rehabilitation After Breast CancerDocument2 pagesPhysical Rehabilitation After Breast CancerFitra PurnamaPas encore d'évaluation
- Anterior Cruciate Ligament All InsideDocument7 pagesAnterior Cruciate Ligament All InsideVijay KumarPas encore d'évaluation
- Ataxias Neuro Condition DetailedDocument80 pagesAtaxias Neuro Condition DetailedMikail AtiyehPas encore d'évaluation
- Simple Guide Orthopadics Chapter 13 Upper Limb ConditionsDocument20 pagesSimple Guide Orthopadics Chapter 13 Upper Limb ConditionsSurgicalgownPas encore d'évaluation
- Spinal Cord Injury Rehabilitation Webinar 2020 PDFDocument2 pagesSpinal Cord Injury Rehabilitation Webinar 2020 PDFGirijashankar KhuntiaPas encore d'évaluation
- Co-Ordination: Prepared by Ahmed Shawky AliDocument59 pagesCo-Ordination: Prepared by Ahmed Shawky Alivenkata ramakrishnaiahPas encore d'évaluation
- Oculomotor Nerve: Components Main Action SuppliesDocument10 pagesOculomotor Nerve: Components Main Action Suppliesdisha1990Pas encore d'évaluation
- Tx3: Bobath'S Neurodevelopmental Treatment: PT Applications Team DLSMHSI CRS PT Department AY 2018-2019Document4 pagesTx3: Bobath'S Neurodevelopmental Treatment: PT Applications Team DLSMHSI CRS PT Department AY 2018-2019Pauline JaleaPas encore d'évaluation
- The Patho-Mechanics of LBPDocument32 pagesThe Patho-Mechanics of LBPydpPas encore d'évaluation
- Disability Evaluation: Radhika ChintamaniDocument58 pagesDisability Evaluation: Radhika ChintamaniBhavya Amin0% (1)
- DR Jagdish Narayan Assistant Professor Department of PhysiologyDocument75 pagesDR Jagdish Narayan Assistant Professor Department of PhysiologyYordanos GetachewPas encore d'évaluation
- Introduction To MovementsDocument42 pagesIntroduction To MovementsRamalingam KanagarajPas encore d'évaluation
- Lesions of Upper Motor Neurons and Lower Motor NeuronsDocument9 pagesLesions of Upper Motor Neurons and Lower Motor NeuronsAdhitya Rama Jr.Pas encore d'évaluation
- Muscular DystrophyDocument4 pagesMuscular DystrophyEnachi OlgaPas encore d'évaluation
- Eyal Lederman - Process Approach in PTDocument72 pagesEyal Lederman - Process Approach in PTYuldash100% (1)
- Neuromuscular: Cranial NervesDocument30 pagesNeuromuscular: Cranial NerveswanderlastPas encore d'évaluation
- PHT 1261C Tests and Measurements Dr. KaneDocument17 pagesPHT 1261C Tests and Measurements Dr. Kanenico7christian100% (1)
- Neuro Written I TablesDocument6 pagesNeuro Written I TablesSolomon Seth SallforsPas encore d'évaluation
- Week 2 Ethics and Professionalism in Physical TherapyDocument6 pagesWeek 2 Ethics and Professionalism in Physical TherapyfrancePas encore d'évaluation
- Introductio To OrthoticsDocument8 pagesIntroductio To OrthoticsGopi Krishnan100% (1)
- Anatomy AnglesDocument27 pagesAnatomy AnglesKiko KikoPas encore d'évaluation
- 2016 Biomechanics of The HipDocument8 pages2016 Biomechanics of The HipilanPas encore d'évaluation
- Basic Biomechanics of The HipDocument8 pagesBasic Biomechanics of The HipManuel Azael Rodríguez CigalaPas encore d'évaluation
- Ankle TappingDocument4 pagesAnkle TappingSenthilkumar ThiyagarajanPas encore d'évaluation
- Abdominal Stretching ExsDocument1 pageAbdominal Stretching ExsSenthilkumar ThiyagarajanPas encore d'évaluation
- Hand Gliding Exercise After SurgeryDocument10 pagesHand Gliding Exercise After SurgerySenthilkumar ThiyagarajanPas encore d'évaluation
- Ankle TappingDocument4 pagesAnkle TappingSenthilkumar ThiyagarajanPas encore d'évaluation
- Cervical ExerciseDocument1 pageCervical ExerciseSenthilkumar Thiyagarajan100% (1)
- Postromedial Dic ProlapsDocument3 pagesPostromedial Dic ProlapsSenthilkumar Thiyagarajan100% (1)
- Active Cycle Breathing Technique-Easy DemoDocument3 pagesActive Cycle Breathing Technique-Easy DemoSenthilkumar ThiyagarajanPas encore d'évaluation
- Anatomymnemonics PDFDocument28 pagesAnatomymnemonics PDFSenthilkumar ThiyagarajanPas encore d'évaluation
- Abdominal IncisionsDocument9 pagesAbdominal IncisionsSenthilkumar ThiyagarajanPas encore d'évaluation
- Aids To The Examination of Peripheral Nervous SystemDocument67 pagesAids To The Examination of Peripheral Nervous SystemSenthilkumar ThiyagarajanPas encore d'évaluation
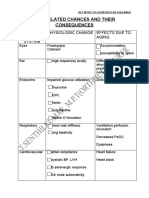
- Age Related Changes and Its Effects in Human Body SystemDocument2 pagesAge Related Changes and Its Effects in Human Body SystemSenthilkumar ThiyagarajanPas encore d'évaluation
- Proprioception & Neuromuscular Control Flyer 2009Document3 pagesProprioception & Neuromuscular Control Flyer 2009Senthilkumar ThiyagarajanPas encore d'évaluation
- C:/Documents and Settings/student/Desktop/physiotherapy Protocol FOR HEMIPLEGIC PDFDocument13 pagesC:/Documents and Settings/student/Desktop/physiotherapy Protocol FOR HEMIPLEGIC PDFSenthilkumar ThiyagarajanPas encore d'évaluation
- Basic Brain Anatomy and Physiology PDFDocument10 pagesBasic Brain Anatomy and Physiology PDFSenthilkumar Thiyagarajan100% (3)
- StretchDocument25 pagesStretchSenthilkumar ThiyagarajanPas encore d'évaluation
- All Orthopedic TestsDocument7 pagesAll Orthopedic Testschandran2679Pas encore d'évaluation
- Above Knee Amputation Exc PDFDocument5 pagesAbove Knee Amputation Exc PDFSenthilkumar ThiyagarajanPas encore d'évaluation
- Joint and Soft Tissue InjectionsDocument13 pagesJoint and Soft Tissue InjectionsSenthilkumar ThiyagarajanPas encore d'évaluation
- Post Natal Exercise PrescriptionDocument8 pagesPost Natal Exercise PrescriptionSenthilkumar ThiyagarajanPas encore d'évaluation
- StretchDocument25 pagesStretchSenthilkumar ThiyagarajanPas encore d'évaluation
- McKenzie Self-Treatments For SciaticaDocument3 pagesMcKenzie Self-Treatments For SciaticaSenthilkumar Thiyagarajan75% (4)
- Free Exercises For The Upper Limb Lower Limb and SpineDocument14 pagesFree Exercises For The Upper Limb Lower Limb and SpineJatin SimbalPas encore d'évaluation
- Orthopedic Assessment For PhysiotherapistDocument3 pagesOrthopedic Assessment For Physiotherapistsenthilkumar76% (21)
- Human Movements and Its Controlling Muscles - For Physiotherapy and Medical StudentsDocument4 pagesHuman Movements and Its Controlling Muscles - For Physiotherapy and Medical StudentssenthilkumarPas encore d'évaluation
- Tourniquet Use at The Boston Marathon Bombing: Lost in TranslationDocument6 pagesTourniquet Use at The Boston Marathon Bombing: Lost in TranslationFabio Ferreira SaPas encore d'évaluation
- Test Bank For Essentials of Assistive Technologies 1st Edition Albert M Cook DownloadDocument5 pagesTest Bank For Essentials of Assistive Technologies 1st Edition Albert M Cook Downloadazurawinifredupaa8mPas encore d'évaluation
- Abdhini Biswas Medical Devices Roll-O1 AssignmentDocument26 pagesAbdhini Biswas Medical Devices Roll-O1 AssignmentAbdhini BiswasPas encore d'évaluation
- September 27, 2019 Strathmore TimesDocument16 pagesSeptember 27, 2019 Strathmore TimesStrathmore TimesPas encore d'évaluation
- Prosthetic Knee SystemsDocument2 pagesProsthetic Knee SystemshppresarioPas encore d'évaluation
- 5842 13364 1 SMDocument40 pages5842 13364 1 SMYanti RosalinaPas encore d'évaluation
- AmputationDocument40 pagesAmputationaeruginoPas encore d'évaluation
- Open FractureDocument106 pagesOpen FractureNizwan ShamPas encore d'évaluation
- Trauma Vaskular - NewDocument51 pagesTrauma Vaskular - NewYoga APas encore d'évaluation
- Falls Sustained During Inpatient Rehabilitation After Lower Limb Amputation Prevalence and PredictorsDocument12 pagesFalls Sustained During Inpatient Rehabilitation After Lower Limb Amputation Prevalence and PredictorsFaeyz OrabiPas encore d'évaluation
- Icrc - War Surgery 2Document640 pagesIcrc - War Surgery 2Florina PopaPas encore d'évaluation
- Critical Hits Rolls by Josef Tham, v2.0 atDocument3 pagesCritical Hits Rolls by Josef Tham, v2.0 atghostvalleyPas encore d'évaluation
- VSR 511Document26 pagesVSR 511DrHemant PanchalPas encore d'évaluation
- Healing With Magnets March2017Document29 pagesHealing With Magnets March2017anon_383546355100% (6)
- Controversies in Lower-Extremity AmputationDocument12 pagesControversies in Lower-Extremity AmputationEGPas encore d'évaluation
- Musculoskeletal MCQDocument12 pagesMusculoskeletal MCQVallesh ShettyPas encore d'évaluation
- A Clinical Study of Diabetic Foot Ulcers and ManagementDocument7 pagesA Clinical Study of Diabetic Foot Ulcers and ManagementIJAR JOURNALPas encore d'évaluation
- A Case Study by Rachael Hargreaves of The OT Practice UKDocument3 pagesA Case Study by Rachael Hargreaves of The OT Practice UKKean Debert SaladagaPas encore d'évaluation
- Van Nes Rotation-Plasty-1Document29 pagesVan Nes Rotation-Plasty-1Alfred Jackson100% (1)
- Amputee Framework GuidelinesDocument34 pagesAmputee Framework GuidelinesRednaxela EnnaPas encore d'évaluation
- Amputation of The Foot PDFDocument29 pagesAmputation of The Foot PDFNyoman MaharmayaPas encore d'évaluation
- 6D - Control of Limb Prostheses - O&P Virtual LibraryDocument22 pages6D - Control of Limb Prostheses - O&P Virtual LibraryBapina Kumar RoutPas encore d'évaluation
- Bibliography of Orthopaedic Problems in Developing CountriesDocument116 pagesBibliography of Orthopaedic Problems in Developing CountriesCristina IliePas encore d'évaluation
- Examination of A Male For Determination of PotencyDocument4 pagesExamination of A Male For Determination of PotencyHarish AgarwalPas encore d'évaluation
- New Disability Assessment Gazzette - 2024Document413 pagesNew Disability Assessment Gazzette - 2024nikkiPas encore d'évaluation
- Hyperbaric Oxygen Therapy For A Pediatric Electrical BurnDocument3 pagesHyperbaric Oxygen Therapy For A Pediatric Electrical Burnsarah iriamanaPas encore d'évaluation
- Dictionary P&O TermsDocument244 pagesDictionary P&O Termsinstrumed_global100% (1)
- Amputation Below KneeDocument1 pageAmputation Below KneeLisnainiMuchlisPas encore d'évaluation
- BedmakingDocument17 pagesBedmakingKlai Arriola75% (4)