Vous aimerez peut-être aussi
- Case Presentation On Pharyngitis2Document10 pagesCase Presentation On Pharyngitis2kamini ChoudharyPas encore d'évaluation
- D CS Pneumonia BBDocument25 pagesD CS Pneumonia BBKshayna 1234Pas encore d'évaluation
- Toxic Multinodular Goiter Physical ExaminationDocument2 pagesToxic Multinodular Goiter Physical ExaminationAngie MandeoyaPas encore d'évaluation
- Case Presentation On Copd: By, Thomas Eipe Pharm D InternDocument32 pagesCase Presentation On Copd: By, Thomas Eipe Pharm D InternThomas EipePas encore d'évaluation
- Patient InformationDocument15 pagesPatient InformationPriyanjali SainiPas encore d'évaluation
- Case Scenerio Nephrotic SyndromeDocument4 pagesCase Scenerio Nephrotic SyndromeEllen AngelPas encore d'évaluation
- Asthma Case StudyDocument39 pagesAsthma Case StudyYzel Vasquez AdavanPas encore d'évaluation
- Case Presentation On Supraventricular TachycardiaDocument64 pagesCase Presentation On Supraventricular TachycardiaHazel AsperaPas encore d'évaluation
- Decompensated Liver DiseaseDocument16 pagesDecompensated Liver Diseasedk.clinicalresearchPas encore d'évaluation
- Case Study SurgeryDocument12 pagesCase Study SurgeryrupaliPas encore d'évaluation
- Case Study On HEAD INJURYDocument11 pagesCase Study On HEAD INJURYanimesh pandaPas encore d'évaluation
- History Taking OBS GYNDocument10 pagesHistory Taking OBS GYNzvkznhsw2tPas encore d'évaluation
- Case Presentation 2Document53 pagesCase Presentation 2Hussain AzharPas encore d'évaluation
- Nursing Case Study - 1 - (Acs)Document32 pagesNursing Case Study - 1 - (Acs)nidhiPas encore d'évaluation
- Drug Name Mechanism of Action Dosage Indication Contraindication Side Effects/ Adverse Effects Nursing ResponsibilitiesDocument4 pagesDrug Name Mechanism of Action Dosage Indication Contraindication Side Effects/ Adverse Effects Nursing ResponsibilitiesKat BausaPas encore d'évaluation
- Broncho Pnuemonia MEDICALDocument9 pagesBroncho Pnuemonia MEDICALArchana SahuPas encore d'évaluation
- Danger Signs in NewbornDocument22 pagesDanger Signs in NewbornAbhirup BosePas encore d'évaluation
- Case Presentation Anahata Kaur CabgDocument31 pagesCase Presentation Anahata Kaur CabgShefali SharmaPas encore d'évaluation
- Case Study Breast CancerDocument20 pagesCase Study Breast Cancersantosh kumarPas encore d'évaluation
- Case Study Stomach CancerDocument2 pagesCase Study Stomach CancerJosePas encore d'évaluation
- Asma CaseDocument42 pagesAsma CasenadienPas encore d'évaluation
- Care Plan On: Submitted To: Submitted byDocument38 pagesCare Plan On: Submitted To: Submitted byMoonPas encore d'évaluation
- Case Presentation On MalariaDocument13 pagesCase Presentation On Malarialavate amol bhimraoPas encore d'évaluation
- Grand ReportsDocument60 pagesGrand ReportsfilchibuffPas encore d'évaluation
- Case Study Liver CirrhosisDocument55 pagesCase Study Liver CirrhosisJoseph Emmanuel CandaPas encore d'évaluation
- Case Study of Renal FailurDocument15 pagesCase Study of Renal FailurYousef Jafar0% (1)
- Case Study - Nephrotic SyndromeDocument42 pagesCase Study - Nephrotic Syndromefarmasi rsud cilincingPas encore d'évaluation
- Case Presentation: by Michael ArmstrongDocument21 pagesCase Presentation: by Michael ArmstrongWirawan Amirul BahriPas encore d'évaluation
- Case Report 2 - Ovarian CystDocument9 pagesCase Report 2 - Ovarian CystA MPas encore d'évaluation
- Therap Case 3Document18 pagesTherap Case 3Safoora RafeeqPas encore d'évaluation
- Toxic Shock Syndrome - PPTX 1-1Document49 pagesToxic Shock Syndrome - PPTX 1-1Mohammed Khedr100% (1)
- Nursing Care Plan EportfolioDocument14 pagesNursing Care Plan Eportfolioapi-279212367Pas encore d'évaluation
- Case Presentation On Chronic Liver Disease: Shreyas M Salimath Pharm D 2 Year REG NO. 21Q0172Document18 pagesCase Presentation On Chronic Liver Disease: Shreyas M Salimath Pharm D 2 Year REG NO. 21Q0172AmalinPas encore d'évaluation
- Pathophysiology of DUBDocument18 pagesPathophysiology of DUBAnna San100% (2)
- TH THDocument29 pagesTH THK RAVI KUMARPas encore d'évaluation
- Case Presentation: Paediatrics: by Tapan Jyoti Saikia 8 Sem Gauhati Medical CollegeDocument22 pagesCase Presentation: Paediatrics: by Tapan Jyoti Saikia 8 Sem Gauhati Medical CollegeArpit Mehta100% (1)
- KamanJan ChloroquineDocument3 pagesKamanJan Chloroquinekimberly_cabertePas encore d'évaluation
- Drug Indication Action Side Effects and Adverse Reaction Nursing ConsiderationDocument8 pagesDrug Indication Action Side Effects and Adverse Reaction Nursing Considerationkier khierPas encore d'évaluation
- Physical Assessment - AnemiaDocument14 pagesPhysical Assessment - AnemiaMerrrks100% (1)
- IUFDDocument33 pagesIUFDIrwin FitriansyahPas encore d'évaluation
- c-7 Case PresentatonDocument11 pagesc-7 Case PresentatonRaja0% (1)
- Peds Case 3Document5 pagesPeds Case 3Mohammed AhmedPas encore d'évaluation
- Toaz - Info Case Study Pneumonia PRDocument41 pagesToaz - Info Case Study Pneumonia PRTrixPas encore d'évaluation
- Doxovent M MedicalDocument38 pagesDoxovent M MedicalkurutalaPas encore d'évaluation
- 3rd Year Precept Pedia Case 4 HydroceleDocument4 pages3rd Year Precept Pedia Case 4 Hydrocelekristel_nicole18yaho100% (1)
- History:: Chief Complaint: History of Present IllnessDocument4 pagesHistory:: Chief Complaint: History of Present IllnessIbrahem Y. NajjarPas encore d'évaluation
- Case Presentation Knee Pain PDFDocument16 pagesCase Presentation Knee Pain PDFIchmatul Hidayah OktaveniPas encore d'évaluation
- ANTENATAL CARE Translate GooglingDocument26 pagesANTENATAL CARE Translate GooglingLutfi ari206100% (2)
- Epilepsy CaseDocument17 pagesEpilepsy CaseSuresh ThanneruPas encore d'évaluation
- Case PresentationDocument24 pagesCase Presentationnaega hoshii'hhPas encore d'évaluation
- CATARACT History Taking and ExaminationDocument28 pagesCATARACT History Taking and ExaminationJosephPas encore d'évaluation
- Management of Patient With Meningitis and Encephalitis: ModeratorDocument71 pagesManagement of Patient With Meningitis and Encephalitis: ModeratorSachin DwivediPas encore d'évaluation
- NCP PPHDocument2 pagesNCP PPHMark Joseph Christian100% (1)
- Asthma Definition:: CausesDocument10 pagesAsthma Definition:: CausesLoly IsrainiPas encore d'évaluation
- CP On Abrutio PlacentaDocument13 pagesCP On Abrutio PlacentaUsha DeviPas encore d'évaluation
- Case PresentationDocument22 pagesCase PresentationVikaPas encore d'évaluation
- Nursing Process 3Document10 pagesNursing Process 3Shubhra Sheoran100% (1)
- DiarrhoeaDocument23 pagesDiarrhoeaPrepladder MedicinePas encore d'évaluation
- Identification DataDocument22 pagesIdentification DataDimpal Choudhary100% (1)
- Peripheral Artery Disease: Nikhil Vaishnav M.Sc. (Nursing)Document70 pagesPeripheral Artery Disease: Nikhil Vaishnav M.Sc. (Nursing)Dimpal ChoudharyPas encore d'évaluation
- Pathophysiology of Pleural EffusionDocument1 pagePathophysiology of Pleural EffusionDimpal ChoudharyPas encore d'évaluation
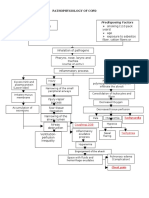
- Streptococcus Pneumonae: Pathophysiology of CopdDocument1 pageStreptococcus Pneumonae: Pathophysiology of CopdDimpal ChoudharyPas encore d'évaluation
- Pathophysiology of PneumoniaDocument4 pagesPathophysiology of PneumoniaDimpal ChoudharyPas encore d'évaluation
- Pulmonary FibrosisDocument4 pagesPulmonary FibrosisDimpal Choudhary100% (2)
- Nursing Assessment Nursing Diagnosis Goal Planning Rationale Implementation Evaluation Subjective DataDocument5 pagesNursing Assessment Nursing Diagnosis Goal Planning Rationale Implementation Evaluation Subjective DataDimpal Choudhary100% (1)
- Nursing Assessment Nursing Diagnosis Goal Planning Rationale Implementation Evaluation Subjective DataDocument4 pagesNursing Assessment Nursing Diagnosis Goal Planning Rationale Implementation Evaluation Subjective DataDimpal ChoudharyPas encore d'évaluation
- Bladder IrrigationDocument5 pagesBladder IrrigationDimpal ChoudharyPas encore d'évaluation
- Lumber Puncture ProcedureDocument8 pagesLumber Puncture ProcedureDimpal ChoudharyPas encore d'évaluation
- Procedure On Lumber PunctureDocument8 pagesProcedure On Lumber PunctureDimpal ChoudharyPas encore d'évaluation
- Congenital Heart DiseaseDocument82 pagesCongenital Heart DiseaseDimpal ChoudharyPas encore d'évaluation
- Uninodular Goitre: One Thyroid Nodule Can Be Either Inactive, or Active (Toxic)Document6 pagesUninodular Goitre: One Thyroid Nodule Can Be Either Inactive, or Active (Toxic)Dimpal ChoudharyPas encore d'évaluation
- Nursing EducationDocument19 pagesNursing EducationDimpal ChoudharyPas encore d'évaluation
- Procedure On Chest PhysiotherapyDocument13 pagesProcedure On Chest PhysiotherapyDimpal ChoudharyPas encore d'évaluation
- Preparation OF Group Work: Netaji Subhash College of NursingDocument7 pagesPreparation OF Group Work: Netaji Subhash College of NursingDimpal ChoudharyPas encore d'évaluation
- Self-Directed LearningDocument18 pagesSelf-Directed LearningDimpal ChoudharyPas encore d'évaluation
- Polycythemia Vera: What Are The Symptoms of Polycythemia?Document10 pagesPolycythemia Vera: What Are The Symptoms of Polycythemia?Dimpal ChoudharyPas encore d'évaluation
- Introduction-:: Time Specific Objective Content Av AidsDocument7 pagesIntroduction-:: Time Specific Objective Content Av AidsDimpal ChoudharyPas encore d'évaluation
- It Is of Two Types Natural Disaster Man - Made DisasterDocument4 pagesIt Is of Two Types Natural Disaster Man - Made DisasterDimpal ChoudharyPas encore d'évaluation
- Care Plan On PneumoniaDocument22 pagesCare Plan On PneumoniaDimpal Choudhary100% (3)
- Chapter Three Foundation of Group Behavior: 1.1. Defining and Classifying Team And/or GroupDocument17 pagesChapter Three Foundation of Group Behavior: 1.1. Defining and Classifying Team And/or GroupMikias DegwalePas encore d'évaluation
- Anterior Open Capsular Shift Rehabilitation Protocol (Accelerated - Overhead Athlete)Document4 pagesAnterior Open Capsular Shift Rehabilitation Protocol (Accelerated - Overhead Athlete)dr_finch511Pas encore d'évaluation
- GRASPSDocument3 pagesGRASPSESTRELLA RAGAYPas encore d'évaluation
- Toaz - Info Module in Ergonomics and Planning Facilities For The Hospitality Industry PRDocument33 pagesToaz - Info Module in Ergonomics and Planning Facilities For The Hospitality Industry PRma celine villoPas encore d'évaluation
- Uttarakhand Round 2 Revised Allotment Dated 29oct 5pmDocument264 pagesUttarakhand Round 2 Revised Allotment Dated 29oct 5pmPrudhvi MadamanchiPas encore d'évaluation
- Case Study Hypertension - EditedDocument8 pagesCase Study Hypertension - EditedJayRenePas encore d'évaluation
- Safety Data Sheet: According To Regulation (EC) No. 1907/2006Document9 pagesSafety Data Sheet: According To Regulation (EC) No. 1907/2006Timothy NathanielPas encore d'évaluation
- Oet 2.0 Listening Task 2: Listening Sub-Test Listening Sub-TestDocument7 pagesOet 2.0 Listening Task 2: Listening Sub-Test Listening Sub-TestKrishna Ramas-MaddiPas encore d'évaluation
- Synopsis OnDocument4 pagesSynopsis OnSatish Waran SPas encore d'évaluation
- Southwestern University Medical Center: Obstetrics Gynecology WardDocument33 pagesSouthwestern University Medical Center: Obstetrics Gynecology WardChresia Schae MondejarPas encore d'évaluation
- Service Marketing Module 1Document27 pagesService Marketing Module 1preethi tmPas encore d'évaluation
- Nonfiction Reading Test Reading: Directions: Read The Following Passage and Answer The Questions That Follow. ReferDocument3 pagesNonfiction Reading Test Reading: Directions: Read The Following Passage and Answer The Questions That Follow. ReferJuan Marcelo Ticona100% (1)
- Quality of Work Life in CamphorDocument79 pagesQuality of Work Life in Camphorshobhit100% (1)
- Annotated Bibliography 1Document2 pagesAnnotated Bibliography 1api-509555528Pas encore d'évaluation
- Studiu 2018Document7 pagesStudiu 2018Catalina CalinPas encore d'évaluation
- Paniyas of WayanadDocument18 pagesPaniyas of WayanadMohammed ArshadPas encore d'évaluation
- LNAT Practice Essays: "The UK Should Codify Its Constitution" DiscussDocument2 pagesLNAT Practice Essays: "The UK Should Codify Its Constitution" DiscussAnisha VPas encore d'évaluation
- Miranda, Elizabeth S. - BSHM3B (GEC107 W4) .Document8 pagesMiranda, Elizabeth S. - BSHM3B (GEC107 W4) .Grace Hermano ManiponPas encore d'évaluation
- A Comparison of Emergence Delirium Scales Following General Anesthesia in ChildrenDocument8 pagesA Comparison of Emergence Delirium Scales Following General Anesthesia in ChildrenNongnapat KettungmunPas encore d'évaluation
- Konsep Dasar Terapi KomplementerDocument52 pagesKonsep Dasar Terapi KomplementerRetno Anggraini100% (1)
- Apple Samsung HuaweiDocument3 pagesApple Samsung HuaweiGround ZeroPas encore d'évaluation
- Whohgnwg85 10 PDFDocument34 pagesWhohgnwg85 10 PDFbabyPas encore d'évaluation
- How Is Type 2 Diabetes Treated - What To Know If You Are Newly DiagnosedDocument2 pagesHow Is Type 2 Diabetes Treated - What To Know If You Are Newly DiagnosedRatnaPrasadNalamPas encore d'évaluation
- Prospect IceDocument233 pagesProspect IceMedical KnowledgePas encore d'évaluation
- Toxic MasculinityDocument4 pagesToxic MasculinitymclarisabarlisPas encore d'évaluation
- Blood PressureDocument154 pagesBlood PressureJanine Anderson100% (1)
- Kimberley Coastal Voyage: Darwin, AustraliaDocument2 pagesKimberley Coastal Voyage: Darwin, AustraliaAustin Viel Lagman MedinaPas encore d'évaluation
- Reflective Writing 2Document4 pagesReflective Writing 2dileepkumar.duhs4817Pas encore d'évaluation
- Module 6 THE HEALTH CARE PROVIDERDocument8 pagesModule 6 THE HEALTH CARE PROVIDERColeen TanPas encore d'évaluation
- TFM 4Document8 pagesTFM 4Miguel de VivarPas encore d'évaluation