Vous aimerez peut-être aussi
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceD'EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceÉvaluation : 4 sur 5 étoiles4/5 (895)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeD'EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeÉvaluation : 4 sur 5 étoiles4/5 (5794)
- Shoe Dog: A Memoir by the Creator of NikeD'EverandShoe Dog: A Memoir by the Creator of NikeÉvaluation : 4.5 sur 5 étoiles4.5/5 (537)
- Grit: The Power of Passion and PerseveranceD'EverandGrit: The Power of Passion and PerseveranceÉvaluation : 4 sur 5 étoiles4/5 (588)
- The Yellow House: A Memoir (2019 National Book Award Winner)D'EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Évaluation : 4 sur 5 étoiles4/5 (98)
- The Little Book of Hygge: Danish Secrets to Happy LivingD'EverandThe Little Book of Hygge: Danish Secrets to Happy LivingÉvaluation : 3.5 sur 5 étoiles3.5/5 (400)
- Never Split the Difference: Negotiating As If Your Life Depended On ItD'EverandNever Split the Difference: Negotiating As If Your Life Depended On ItÉvaluation : 4.5 sur 5 étoiles4.5/5 (838)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureD'EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureÉvaluation : 4.5 sur 5 étoiles4.5/5 (474)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryD'EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryÉvaluation : 3.5 sur 5 étoiles3.5/5 (231)
- The Emperor of All Maladies: A Biography of CancerD'EverandThe Emperor of All Maladies: A Biography of CancerÉvaluation : 4.5 sur 5 étoiles4.5/5 (271)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaD'EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaÉvaluation : 4.5 sur 5 étoiles4.5/5 (266)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersD'EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersÉvaluation : 4.5 sur 5 étoiles4.5/5 (345)
- On Fire: The (Burning) Case for a Green New DealD'EverandOn Fire: The (Burning) Case for a Green New DealÉvaluation : 4 sur 5 étoiles4/5 (74)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyD'EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyÉvaluation : 3.5 sur 5 étoiles3.5/5 (2259)
- Team of Rivals: The Political Genius of Abraham LincolnD'EverandTeam of Rivals: The Political Genius of Abraham LincolnÉvaluation : 4.5 sur 5 étoiles4.5/5 (234)
- The Unwinding: An Inner History of the New AmericaD'EverandThe Unwinding: An Inner History of the New AmericaÉvaluation : 4 sur 5 étoiles4/5 (45)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreD'EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreÉvaluation : 4 sur 5 étoiles4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)D'EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Évaluation : 4.5 sur 5 étoiles4.5/5 (121)
- Her Body and Other Parties: StoriesD'EverandHer Body and Other Parties: StoriesÉvaluation : 4 sur 5 étoiles4/5 (821)
- Short Answer: Essentials of Anatomy and Physiology, 9e (Marieb) Chapter 11 The Cardiovascular SystemDocument23 pagesShort Answer: Essentials of Anatomy and Physiology, 9e (Marieb) Chapter 11 The Cardiovascular SystemRafael CastilloPas encore d'évaluation
- Catheter Replacement of The Needle in Percutaneous Arteriography A New TechniqueDocument10 pagesCatheter Replacement of The Needle in Percutaneous Arteriography A New TechniqueMarioLaVedPas encore d'évaluation
- Nursing Care Plan and Drug StudyDocument4 pagesNursing Care Plan and Drug StudyEllaPas encore d'évaluation
- Global Heart 2013 - Legacy of The Framingham Heart Study. Rationale, Design, Initial Findings, and ImplicationsDocument7 pagesGlobal Heart 2013 - Legacy of The Framingham Heart Study. Rationale, Design, Initial Findings, and ImplicationsCharlie CharcapePas encore d'évaluation
- Concepts of Preload and AfterloadDocument2 pagesConcepts of Preload and AfterloadShar RiveraPas encore d'évaluation
- 2021 AHA ASA Guideline For The Prevention of Stroke in Patients With Stroke and TIA Clinical UpdateDocument43 pages2021 AHA ASA Guideline For The Prevention of Stroke in Patients With Stroke and TIA Clinical UpdateLê Thị HươngPas encore d'évaluation
- Basic Coronary Anatomy - Paul Fefer, MD.Document57 pagesBasic Coronary Anatomy - Paul Fefer, MD.enzomontresolPas encore d'évaluation
- Coronary Artery Disease (Cad)Document4 pagesCoronary Artery Disease (Cad)Freddy PanjaitanPas encore d'évaluation
- Specimen QP - Paper 1 Edexcel (A) Biology AS-LevelDocument22 pagesSpecimen QP - Paper 1 Edexcel (A) Biology AS-LeveljanaPas encore d'évaluation
- Pulmonary CirculationDocument5 pagesPulmonary CirculationGPearce204Pas encore d'évaluation
- Atherosklerosis, Artheriosklerosis Dan Kelainan VaskulerDocument66 pagesAtherosklerosis, Artheriosklerosis Dan Kelainan VaskulerOlivia Chandra DeviPas encore d'évaluation
- Patho A 1. 5 Hemodynamic Disorders (Bongat, 2015)Document12 pagesPatho A 1. 5 Hemodynamic Disorders (Bongat, 2015)Grant GarcesPas encore d'évaluation
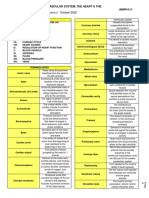
- 1.08 - The Cardiovascular System, The Heart & The Blood VesselsDocument9 pages1.08 - The Cardiovascular System, The Heart & The Blood Vessels13PLAN, SENTH RUEN, APas encore d'évaluation
- LA Myxoma Case PresentationDocument34 pagesLA Myxoma Case PresentationWiwik Puji LestariPas encore d'évaluation
- Monro-Kellie 2.0: The Dynamic Vascular and Venous Pathophysiological Components of Intracranial PressureDocument13 pagesMonro-Kellie 2.0: The Dynamic Vascular and Venous Pathophysiological Components of Intracranial PressureLeandro NogueiraPas encore d'évaluation
- NCP For HypertensionDocument6 pagesNCP For HypertensionJaic Ealston D. Tampus0% (2)
- Renal Blood Flow RegulationDocument3 pagesRenal Blood Flow RegulationTawhid ZihadPas encore d'évaluation
- 2008-2016 Anatomy 2Document20 pages2008-2016 Anatomy 2sayed aashiqPas encore d'évaluation
- Patologi Bedah Sistem Kardiovaskuler Dan RespirasiDocument65 pagesPatologi Bedah Sistem Kardiovaskuler Dan RespirasiMuhammad IqbalPas encore d'évaluation
- Concept Map 1Document3 pagesConcept Map 1Rubie Ann TillorPas encore d'évaluation
- Primul Meu HolterDocument12 pagesPrimul Meu Holterheraasku7194Pas encore d'évaluation
- UCSF ED US Protocol LE Venous - FinalDocument8 pagesUCSF ED US Protocol LE Venous - FinalMANGPas encore d'évaluation
- PowerpointDocument12 pagesPowerpointapi-585922320Pas encore d'évaluation
- Atlas of CT Angiography Normal and Pathologic FindingsDocument464 pagesAtlas of CT Angiography Normal and Pathologic FindingsMariluzArango100% (1)
- Acute Pulmonary Edema - Nitrate or Diuretic Dr. Heny Martini, SPJP (K) PDFDocument50 pagesAcute Pulmonary Edema - Nitrate or Diuretic Dr. Heny Martini, SPJP (K) PDFmgoez077Pas encore d'évaluation
- CXR ABC by DR ShamolDocument139 pagesCXR ABC by DR Shamolazar103100% (3)
- Craniocervical Arterial VariationsDocument171 pagesCraniocervical Arterial VariationsMircea JunbeiPas encore d'évaluation
- Slide Deck ACS Referral Forum - DR Adhitia MIni Simposium ACSDocument20 pagesSlide Deck ACS Referral Forum - DR Adhitia MIni Simposium ACSsyahrial fazaPas encore d'évaluation
- P17F06.036.01 - Occlutech Patient Brochure PDA PDFDocument2 pagesP17F06.036.01 - Occlutech Patient Brochure PDA PDFHandyka Vb GPas encore d'évaluation
- 1 Cardiovascular SystemDocument37 pages1 Cardiovascular SystemEldevincey Macabata100% (1)