Vous aimerez peut-être aussi
- Reading Sub-Test: Part ADocument17 pagesReading Sub-Test: Part AVijayalakshmi Narayanaswami78% (9)
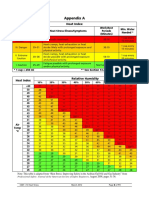
- Heat Index ChartDocument1 pageHeat Index ChartAnvarsha Sharafudheen100% (1)
- Icmr Specimen Referral Form For Covid-19 (Sars-Cov2) : Section A - Patient DetailsDocument2 pagesIcmr Specimen Referral Form For Covid-19 (Sars-Cov2) : Section A - Patient DetailsPcrPas encore d'évaluation
- Icmr Specimen Referral Form For Covid-19 (Sars-Cov2) : (If Yes, Attach Prescription If No, Test Cannot Be Conducted)Document2 pagesIcmr Specimen Referral Form For Covid-19 (Sars-Cov2) : (If Yes, Attach Prescription If No, Test Cannot Be Conducted)narayanasmrithiPas encore d'évaluation
- Tsubo Vital Points For Oriental TherapyDocument251 pagesTsubo Vital Points For Oriental Therapyeiztao100% (32)
- Review: Job Search About Us Candidate Zone Sign OutDocument7 pagesReview: Job Search About Us Candidate Zone Sign OutMd MujtabaPas encore d'évaluation
- Stuart Bloom (Editor), George Webster (Editor), Daniel Marks (Editor) - Oxford Handbook of Gastroenterology & Hepatology (Oxford Medical Handbooks) - Oxford University Press (2021)Document1 146 pagesStuart Bloom (Editor), George Webster (Editor), Daniel Marks (Editor) - Oxford Handbook of Gastroenterology & Hepatology (Oxford Medical Handbooks) - Oxford University Press (2021)aliakbar178Pas encore d'évaluation
- Anatomy of Dermo-Epidermal Junction and Its Applied AspectDocument56 pagesAnatomy of Dermo-Epidermal Junction and Its Applied AspectSiddharth DashPas encore d'évaluation
- Icmr Specimen Referral Form For Covid-19 (Sars-Cov2)Document2 pagesIcmr Specimen Referral Form For Covid-19 (Sars-Cov2)Divin MatthewPas encore d'évaluation
- Icmr Specimen Referral Form For Covid-19 (Sars-Cov2) : Section A - Patient DetailsDocument2 pagesIcmr Specimen Referral Form For Covid-19 (Sars-Cov2) : Section A - Patient DetailsDEE QC CHittoorPas encore d'évaluation
- Icmr Specimen Referral Form For Covid-19 (Sars-Cov2) : Section A - Patient DetailsDocument2 pagesIcmr Specimen Referral Form For Covid-19 (Sars-Cov2) : Section A - Patient Detailszeeshan_iraniPas encore d'évaluation
- SRF ICMR Kerala - PDF (New) PDFDocument2 pagesSRF ICMR Kerala - PDF (New) PDFRenjithPas encore d'évaluation
- Icmr Specimen Referral Form For Covid-19 (Sars-Cov2) : Section A - Patient DetailsDocument4 pagesIcmr Specimen Referral Form For Covid-19 (Sars-Cov2) : Section A - Patient DetailsNag Sai NarahariPas encore d'évaluation
- Icmr Specimen Referral Form For Covid-19 (Sars Cov2) : Section A - Patient DetailsDocument2 pagesIcmr Specimen Referral Form For Covid-19 (Sars Cov2) : Section A - Patient Detailseldridatech pvt ltdPas encore d'évaluation
- Form 44Document3 pagesForm 44Aditya AryaPas encore d'évaluation
- Revised SRF Form 26052021 1Document3 pagesRevised SRF Form 26052021 1Venkat PrasannaPas encore d'évaluation
- Revised SRF Form 22032021 NewDocument3 pagesRevised SRF Form 22032021 NewBiswajeet DasPas encore d'évaluation
- Section B - Medical Information: TEST RESULT (To Be Filled by Covid-19 Testing Lab Facility)Document1 pageSection B - Medical Information: TEST RESULT (To Be Filled by Covid-19 Testing Lab Facility)Kiran BasilPas encore d'évaluation
- Confidential: Medical History and Personal Particulars of Students Joining at IIT MadrasDocument4 pagesConfidential: Medical History and Personal Particulars of Students Joining at IIT MadrasNehaPas encore d'évaluation
- Icmr Specimen Referral Form For Covid-19 (Sars-Cov2) : (If Yes, Attach Prescription If No, Test Cannot Be Conducted)Document2 pagesIcmr Specimen Referral Form For Covid-19 (Sars-Cov2) : (If Yes, Attach Prescription If No, Test Cannot Be Conducted)Lakshay JunejaPas encore d'évaluation
- Icmr Specimen Referral Form For Covid-19 (Sars-Cov2) : (If Yes, Attach Prescription If No, Test Cannot Be Conducted)Document3 pagesIcmr Specimen Referral Form For Covid-19 (Sars-Cov2) : (If Yes, Attach Prescription If No, Test Cannot Be Conducted)aishwaryaPas encore d'évaluation
- Icmr Specimen Referral Form For Covid-19 (Sars-Cov2) : (If Yes, Attach Prescription If No, Test Cannot Be Conducted)Document3 pagesIcmr Specimen Referral Form For Covid-19 (Sars-Cov2) : (If Yes, Attach Prescription If No, Test Cannot Be Conducted)ARSLANPas encore d'évaluation
- Icmr Specimen Referral Form For Covid-19 (Sars-Cov2) : (If Yes, Attach Prescription If No, Test Cannot Be Conducted)Document3 pagesIcmr Specimen Referral Form For Covid-19 (Sars-Cov2) : (If Yes, Attach Prescription If No, Test Cannot Be Conducted)annapurna samalPas encore d'évaluation
- Icmr Specimen Referral Form For Covid-19 (Sars-Cov2) : (If Yes, Attach Prescription If No, Test Cannot Be Conducted)Document2 pagesIcmr Specimen Referral Form For Covid-19 (Sars-Cov2) : (If Yes, Attach Prescription If No, Test Cannot Be Conducted)Aapki saheliPas encore d'évaluation
- Icmr Specimen Referral Form For Covid-19 (Sars-Cov2) : (If Yes, Attach Prescription If No, Test Cannot Be Conducted)Document3 pagesIcmr Specimen Referral Form For Covid-19 (Sars-Cov2) : (If Yes, Attach Prescription If No, Test Cannot Be Conducted)roniee rPas encore d'évaluation
- ICMR Revised SRF For Covid TestDocument2 pagesICMR Revised SRF For Covid TestDEVIKA PHULEPas encore d'évaluation
- Icmr Specimen Referral Form For Covid-19 (Sars-Cov2) : (If Yes, Attach Prescription If No, Test Cannot Be Conducted)Document3 pagesIcmr Specimen Referral Form For Covid-19 (Sars-Cov2) : (If Yes, Attach Prescription If No, Test Cannot Be Conducted)Anilkumar m rPas encore d'évaluation
- Icmr Specimen Referral Form For Covid-19 (Sars-Cov2) : (If Yes, Attach Prescription If No, Test Cannot Be Conducted)Document2 pagesIcmr Specimen Referral Form For Covid-19 (Sars-Cov2) : (If Yes, Attach Prescription If No, Test Cannot Be Conducted)Rahul KumarPas encore d'évaluation
- Icmr Specimen Referral Form For Covid-19 (Sars-Cov2) : (If Yes, Attach Prescription If No, Test Cannot Be Conducted)Document2 pagesIcmr Specimen Referral Form For Covid-19 (Sars-Cov2) : (If Yes, Attach Prescription If No, Test Cannot Be Conducted)Madhusmita MishraPas encore d'évaluation
- Icmr Specimen Referral Form For Covid-19 (Sars-Cov2) : (If Yes, Attach Prescription If No, Test Cannot Be Conducted)Document2 pagesIcmr Specimen Referral Form For Covid-19 (Sars-Cov2) : (If Yes, Attach Prescription If No, Test Cannot Be Conducted)Harbrinder GurmPas encore d'évaluation
- Icmr Specimen Referral Form For Covid-19 (Sars-Cov2) : (If Yes, Attach Prescription If No, Test Cannot Be Conducted)Document3 pagesIcmr Specimen Referral Form For Covid-19 (Sars-Cov2) : (If Yes, Attach Prescription If No, Test Cannot Be Conducted)Pravat TiadiPas encore d'évaluation
- Icmr Specimen Referral Form For Covid-19 (Sars-Cov2) : (If Yes, Attach Prescription If No, Test Cannot Be Conducted)Document3 pagesIcmr Specimen Referral Form For Covid-19 (Sars-Cov2) : (If Yes, Attach Prescription If No, Test Cannot Be Conducted)Satyasarathi DhalPas encore d'évaluation
- Icmr Specimen Referral Form For Covid-19 (Sars-Cov2) : (If Yes, Attach Prescription If No, Test Cannot Be Conducted)Document3 pagesIcmr Specimen Referral Form For Covid-19 (Sars-Cov2) : (If Yes, Attach Prescription If No, Test Cannot Be Conducted)Rohit KarhadePas encore d'évaluation
- ReportDocument2 pagesReportRahul V SPas encore d'évaluation
- Icmr Specimen Referral Form For Covid-19 (Sars-Cov2) : (If Yes, Attach Prescription If No, Test Cannot Be Conducted)Document2 pagesIcmr Specimen Referral Form For Covid-19 (Sars-Cov2) : (If Yes, Attach Prescription If No, Test Cannot Be Conducted)gopimicroPas encore d'évaluation
- Icmr Specimen Referral Form For Covid-19 (Sars-Cov2) : (If Yes, Attach Prescription If No, Test Cannot Be Conducted)Document2 pagesIcmr Specimen Referral Form For Covid-19 (Sars-Cov2) : (If Yes, Attach Prescription If No, Test Cannot Be Conducted)DevPas encore d'évaluation
- ADR AEFI Reporting FormDocument1 pageADR AEFI Reporting Formgulafsha1Pas encore d'évaluation
- Icmr Specimen Referral Form For Covid-19 (Sars-Cov2) : (If Yes, Attach Prescription If No, Test Cannot Be Conducted)Document2 pagesIcmr Specimen Referral Form For Covid-19 (Sars-Cov2) : (If Yes, Attach Prescription If No, Test Cannot Be Conducted)Madhusmita MishraPas encore d'évaluation
- Icmr Specimen Referral Form For Covid-19 (Sars-Cov2) : (If Yes, Attach Prescription If No, Test Cannot Be Conducted)Document3 pagesIcmr Specimen Referral Form For Covid-19 (Sars-Cov2) : (If Yes, Attach Prescription If No, Test Cannot Be Conducted)likhitPas encore d'évaluation
- Icmr Specimen Referral Form For Covid-19 (Sars-Cov2) : (If Yes, Attach Prescription If No, Test Cannot Be Conducted)Document2 pagesIcmr Specimen Referral Form For Covid-19 (Sars-Cov2) : (If Yes, Attach Prescription If No, Test Cannot Be Conducted)Bharat BhushanPas encore d'évaluation
- Icmr Specimen Referral Form For Covid-19 (Sars-Cov2) : (If Yes, Attach Prescription If No, Test Cannot Be Conducted)Document3 pagesIcmr Specimen Referral Form For Covid-19 (Sars-Cov2) : (If Yes, Attach Prescription If No, Test Cannot Be Conducted)Shashi SagarPas encore d'évaluation
- Icmr Specimen Referral Form For Covid-19 (Sars-Cov2) : (If Yes, Attach Prescription If No, Test Cannot Be Conducted)Document3 pagesIcmr Specimen Referral Form For Covid-19 (Sars-Cov2) : (If Yes, Attach Prescription If No, Test Cannot Be Conducted)Aakansha GuptaPas encore d'évaluation
- Icmr Specimen Referral Form For Covid Icmr Specimen Referral Form For Covid-19 (Sars-Cov2) Cov2)Document2 pagesIcmr Specimen Referral Form For Covid Icmr Specimen Referral Form For Covid-19 (Sars-Cov2) Cov2)SolivagantPas encore d'évaluation
- Icmr Specimen Referral Form For Covid-19 (Sars-Cov2) : (If Yes, Attach Prescription If No, Test Cannot Be Conducted)Document3 pagesIcmr Specimen Referral Form For Covid-19 (Sars-Cov2) : (If Yes, Attach Prescription If No, Test Cannot Be Conducted)Mohammed Shakeel khudusPas encore d'évaluation
- Icmr Specimen Referral Form For Covid-19 (Sars-Cov2) : (If Yes, Attach Prescription If No, Test Cannot Be Conducted)Document3 pagesIcmr Specimen Referral Form For Covid-19 (Sars-Cov2) : (If Yes, Attach Prescription If No, Test Cannot Be Conducted)Lavanya LakshmiPas encore d'évaluation
- Icmr Specimen Referral Form For Covid-19 (Sars-Cov2) : (If Yes, Attach Prescription If No, Test Cannot Be Conducted)Document3 pagesIcmr Specimen Referral Form For Covid-19 (Sars-Cov2) : (If Yes, Attach Prescription If No, Test Cannot Be Conducted)forged godPas encore d'évaluation
- Icmr Specimen Referral Form For Covid-19 (Sars-Cov2) : (If Yes, Attach Prescription If No, Test Cannot Be Conducted)Document2 pagesIcmr Specimen Referral Form For Covid-19 (Sars-Cov2) : (If Yes, Attach Prescription If No, Test Cannot Be Conducted)Sashibhusan NayakPas encore d'évaluation
- Icmr Specimen Referral Form For Covid-19 (Sars-Cov2) : (If Yes, Attach Prescription If No, Test Cannot Be Conducted)Document2 pagesIcmr Specimen Referral Form For Covid-19 (Sars-Cov2) : (If Yes, Attach Prescription If No, Test Cannot Be Conducted)umera shah aliPas encore d'évaluation
- Icmr Specimen Referral Form For Covid-19 (Sars-Cov2) : (If Yes, Attach Prescription If No, Test Cannot Be Conducted)Document3 pagesIcmr Specimen Referral Form For Covid-19 (Sars-Cov2) : (If Yes, Attach Prescription If No, Test Cannot Be Conducted)SgPas encore d'évaluation
- Provisional RegistrationDocument9 pagesProvisional RegistrationabuprettyPas encore d'évaluation
- Icmr Specimen Referral Form For Covid-19 (Sars-Cov2) : (If Yes, Attach Prescription If No, Test Cannot Be Conducted)Document2 pagesIcmr Specimen Referral Form For Covid-19 (Sars-Cov2) : (If Yes, Attach Prescription If No, Test Cannot Be Conducted)udayanPas encore d'évaluation
- Icmr Specimen Referral Form For Covid-19 (Sars-Cov2) : (If Yes, Attach Prescription If No, Test Cannot Be Conducted)Document2 pagesIcmr Specimen Referral Form For Covid-19 (Sars-Cov2) : (If Yes, Attach Prescription If No, Test Cannot Be Conducted)ShakirShafiPas encore d'évaluation
- Targeted Patient Safety QuestionnairesDocument27 pagesTargeted Patient Safety QuestionnairesAafreen KhairPas encore d'évaluation
- CbNAAT New FormDocument1 pageCbNAAT New FormDipendra PoudelPas encore d'évaluation
- Typhoid Special Surveillance FormDocument2 pagesTyphoid Special Surveillance FormJess MaglunobPas encore d'évaluation
- Icmr Specimen Referral Form For Covid-19 (Sars-Cov2) : (If Yes, Attach Prescription If No, Test Cannot Be Conducted)Document2 pagesIcmr Specimen Referral Form For Covid-19 (Sars-Cov2) : (If Yes, Attach Prescription If No, Test Cannot Be Conducted)Sufyan UmarPas encore d'évaluation
- Medical CertificateDocument4 pagesMedical CertificateRishi ScifreakPas encore d'évaluation
- Claim FormDocument5 pagesClaim FormppghoshinPas encore d'évaluation
- Icmr Specimen Referral Form For Covid-19 (Sars-Cov2) : (These Fields To Be Filled For All Patients Including Foreigners)Document2 pagesIcmr Specimen Referral Form For Covid-19 (Sars-Cov2) : (These Fields To Be Filled For All Patients Including Foreigners)rakeshPas encore d'évaluation
- Icmr Specimen Referral Form For Covid-19 (Sars-Cov2) : F/Vdc/Msp/14-CtrfDocument2 pagesIcmr Specimen Referral Form For Covid-19 (Sars-Cov2) : F/Vdc/Msp/14-CtrftariqPas encore d'évaluation
- UIIC Claim FormDocument4 pagesUIIC Claim FormDevang TailorPas encore d'évaluation
- Sample Id: Sample Id: 34046605 Icmr Specimen Referral Form Icmr Specimen Referral Form For For Covid-19 (Sars-Cov2) Covid-19 (Sars-Cov2)Document2 pagesSample Id: Sample Id: 34046605 Icmr Specimen Referral Form Icmr Specimen Referral Form For For Covid-19 (Sars-Cov2) Covid-19 (Sars-Cov2)S4 HanaPas encore d'évaluation
- Acute Coronary Syndrome - Antithrombotic Therapy and Secondary PreventionD'EverandAcute Coronary Syndrome - Antithrombotic Therapy and Secondary PreventionPas encore d'évaluation
- The Addiction Counselor's Documentation Sourcebook: The Complete Paperwork Resource for Treating Clients with AddictionsD'EverandThe Addiction Counselor's Documentation Sourcebook: The Complete Paperwork Resource for Treating Clients with AddictionsPas encore d'évaluation
- Interstitial Lung Diseases2Document186 pagesInterstitial Lung Diseases2Mohamed HefnyPas encore d'évaluation
- Research CompletedDocument95 pagesResearch Completedtes beletePas encore d'évaluation
- Human Performance and LimitationsDocument243 pagesHuman Performance and LimitationsListiyani Ismail100% (2)
- DRUGS (Topotecan)Document2 pagesDRUGS (Topotecan)BARRISTERFLOWERSEAURCHIN6Pas encore d'évaluation
- Acog PidDocument3 pagesAcog PidKevin JonathanPas encore d'évaluation
- Lyme Disease Lab Testing ExplanationDocument2 pagesLyme Disease Lab Testing ExplanationAlina PirvPas encore d'évaluation
- Health History Genogram Template V2Document2 pagesHealth History Genogram Template V2Anna Mae AbuanPas encore d'évaluation
- Crush Step 1 ErrataDocument8 pagesCrush Step 1 ErrataShirkeInc100% (1)
- 40 2019 Nausea and VomitingDocument12 pages40 2019 Nausea and Vomitingfeny kusumadewiPas encore d'évaluation
- CXR Made EasyDocument14 pagesCXR Made Easyjaimejm100% (1)
- Tut 202 2018 S1Document23 pagesTut 202 2018 S1Feroza AngamiaPas encore d'évaluation
- Letter To ParentsDocument2 pagesLetter To ParentsAbdul AhadPas encore d'évaluation
- COVID-19 Pandemic, Also Known As The Coronavirus Pandemic, Is ADocument15 pagesCOVID-19 Pandemic, Also Known As The Coronavirus Pandemic, Is ACristinaPas encore d'évaluation
- May Sumotuwethfrsa May Is The Fifth Month of The Year in The Julian and Gregorian Calendars and TheDocument18 pagesMay Sumotuwethfrsa May Is The Fifth Month of The Year in The Julian and Gregorian Calendars and TheRadovan SpiridonovPas encore d'évaluation
- Lary SprayDocument7 pagesLary SprayMedley SinkhaiPas encore d'évaluation
- Labor Law 2 - Deoferio Vs IntelDocument2 pagesLabor Law 2 - Deoferio Vs Inteljason caballeroPas encore d'évaluation
- Food SafetyDocument64 pagesFood SafetyKayeee Si100% (1)
- Euthanasia Reading Comprehension2Document2 pagesEuthanasia Reading Comprehension2Angel O Cordoba RromPas encore d'évaluation
- Clinical Trial Details (PDF Generation Date:-Thu, 01 Apr 2021 00:30:26 GMT)Document4 pagesClinical Trial Details (PDF Generation Date:-Thu, 01 Apr 2021 00:30:26 GMT)Aman TyagiPas encore d'évaluation
- Antibiotic Treatment For Newborns With Congenital Syphilis (Review)Document47 pagesAntibiotic Treatment For Newborns With Congenital Syphilis (Review)link_wolfloboPas encore d'évaluation
- Hepatitis A y Hepatitis EDocument9 pagesHepatitis A y Hepatitis ESMIBA MedicinaPas encore d'évaluation
- Allergic Reactions To Vaccines - UpToDateDocument32 pagesAllergic Reactions To Vaccines - UpToDateKohinoorKohinoorPas encore d'évaluation
- Pediatric Nursing: PilliteriDocument16 pagesPediatric Nursing: PilliteriLeiPas encore d'évaluation
- Quantum Resonance Magnetic Analyzer - Arnulfo Yu Laniba TestDocument87 pagesQuantum Resonance Magnetic Analyzer - Arnulfo Yu Laniba TestArnulfo Yu Laniba100% (3)