Vous aimerez peut-être aussi
- Cognitive and Behavioral Interventions in the Schools: Integrating Theory and Research into PracticeD'EverandCognitive and Behavioral Interventions in the Schools: Integrating Theory and Research into PracticeRosemary FlanaganPas encore d'évaluation
- SleepFoundation SleepDiaryDocument1 pageSleepFoundation SleepDiaryJowel HossainPas encore d'évaluation
- Comprehensive Handbook of Clinical Health PsychologyD'EverandComprehensive Handbook of Clinical Health PsychologyBret A BoyerPas encore d'évaluation
- Brain Health Assessment: Brain Type Brain Fit ScoreDocument5 pagesBrain Health Assessment: Brain Type Brain Fit ScorekinetokidPas encore d'évaluation
- Expressions of the Mind in Words: Writings by a 9 year old kidD'EverandExpressions of the Mind in Words: Writings by a 9 year old kidPas encore d'évaluation
- The Sleep Phenotypes of Attention Deficit Hyperactivity Disorder: The Role of Arousal During Sleep and Implications For TreatmentDocument7 pagesThe Sleep Phenotypes of Attention Deficit Hyperactivity Disorder: The Role of Arousal During Sleep and Implications For TreatmentPierluigi CongedoPas encore d'évaluation
- Teaching Factors That Enhance Learning Among High School Students Diagnosed With Autism Spectrum DisorderDocument13 pagesTeaching Factors That Enhance Learning Among High School Students Diagnosed With Autism Spectrum DisorderAlejandra ParedesPas encore d'évaluation
- Twenty Things To Know About Deep Brain Stimulation, 1E (2015) (PDF) (UnitedVRG)Document297 pagesTwenty Things To Know About Deep Brain Stimulation, 1E (2015) (PDF) (UnitedVRG)amir11601Pas encore d'évaluation
- 100 Day Kit Version 2 0Document104 pages100 Day Kit Version 2 0Mario QuinteroPas encore d'évaluation
- Psychiatric Nonadherence A Solutions-Based Approach by Victor Fornari, Ida DancygerDocument228 pagesPsychiatric Nonadherence A Solutions-Based Approach by Victor Fornari, Ida DancygerJuan IgnacioPas encore d'évaluation
- Guidline Threatment For of Alcohol Use DisorderDocument226 pagesGuidline Threatment For of Alcohol Use Disorderafifberlian100% (1)
- Stuart KDocument247 pagesStuart KZan PhyoPas encore d'évaluation
- Journal of ADHD: & Related DisordersDocument69 pagesJournal of ADHD: & Related DisordersElison J PanggaloPas encore d'évaluation
- National Sleep Foundation's Sleep Time Duration Recommendations Methodology and Results Summary Hirshkowitz2015Document4 pagesNational Sleep Foundation's Sleep Time Duration Recommendations Methodology and Results Summary Hirshkowitz2015Andaz MortinPas encore d'évaluation
- EnxiklopediDocument997 pagesEnxiklopediwilmanurilla17Pas encore d'évaluation
- Disorganized Children, A Guide For Parents and ProfessionalsDocument343 pagesDisorganized Children, A Guide For Parents and ProfessionalsDaltry GáratePas encore d'évaluation
- Reading Test - SchizophreniaDocument9 pagesReading Test - SchizophreniaOlive GroupPas encore d'évaluation
- Understanding ADHD in Girls and Women - Joanne SteerDocument330 pagesUnderstanding ADHD in Girls and Women - Joanne SteerMagyari JuditPas encore d'évaluation
- What Is Permissive ParentingDocument12 pagesWhat Is Permissive Parenting5KevPas encore d'évaluation
- As Characteristics and TraitsDocument5 pagesAs Characteristics and Traitsandrei crisnicPas encore d'évaluation
- Effects of Stretching On Jump Performance - A Systematic Review of PDFDocument241 pagesEffects of Stretching On Jump Performance - A Systematic Review of PDFEric GalianoPas encore d'évaluation
- Mechanisms of Change in Prolonged Exposure Therapy For PTSD-Implications For Clinical PracticeDocument9 pagesMechanisms of Change in Prolonged Exposure Therapy For PTSD-Implications For Clinical PracticeKelly GCPas encore d'évaluation
- ADHD and HypersensitivityDocument5 pagesADHD and HypersensitivityJonathan PeeblesPas encore d'évaluation
- Choate, Laura Hensley - Swimming Upstream - Parenting Girls For Resilience in A Toxic Culture-Oxford University Press (2015)Document305 pagesChoate, Laura Hensley - Swimming Upstream - Parenting Girls For Resilience in A Toxic Culture-Oxford University Press (2015)Claudia HoreanuPas encore d'évaluation
- Survival StrategiesDocument8 pagesSurvival StrategiesDr Jitender SinghPas encore d'évaluation
- Arlene Istar Lev - Transgender Emergence - Therapeutic Guidelines For Working With Gender-Variant People and Their Families-Haworth Press (2004)Document501 pagesArlene Istar Lev - Transgender Emergence - Therapeutic Guidelines For Working With Gender-Variant People and Their Families-Haworth Press (2004)Joana GómezPas encore d'évaluation
- ADHD MythsDocument1 pageADHD Mythsoohbaby617Pas encore d'évaluation
- Normal Sleep PDFDocument54 pagesNormal Sleep PDFGeraldine TaveraPas encore d'évaluation
- Abas 3 Chapter 4Document12 pagesAbas 3 Chapter 4GF David SalasPas encore d'évaluation
- Sleep Hygiene Children Handout PDFDocument2 pagesSleep Hygiene Children Handout PDFVingki DesgianPas encore d'évaluation
- Autism Spectrum Disorders - From Genotypes To Phenotypes PDFDocument95 pagesAutism Spectrum Disorders - From Genotypes To Phenotypes PDFMariaAndreaPas encore d'évaluation
- 3991 CZ Neurobiology of Anxiety AbsDocument3 pages3991 CZ Neurobiology of Anxiety AbsMADHU GIRI 2170094Pas encore d'évaluation
- Psychiatric Care in Severe ObesityDocument351 pagesPsychiatric Care in Severe ObesityAlejandro Flores VelascoPas encore d'évaluation
- Jones Et Al 2016 IntersexDocument274 pagesJones Et Al 2016 IntersexPaulina EzerPas encore d'évaluation
- Conversation StartersDocument4 pagesConversation StartersRazan GhalayiniPas encore d'évaluation
- The ADHD Diagnosis GuideDocument13 pagesThe ADHD Diagnosis GuideArunima KapoorPas encore d'évaluation
- Bipolar Children-Cutting-Edge Controversy Insights and ResearchDocument176 pagesBipolar Children-Cutting-Edge Controversy Insights and Researchdariaevelin100% (1)
- 117 How To Breathe Correctly For Optimal Health Mood Learning & Performance Huberman Lab PodcastDocument51 pages117 How To Breathe Correctly For Optimal Health Mood Learning & Performance Huberman Lab Podcastwaheed khanPas encore d'évaluation
- L. William Ross-Child M.L.C. - The Silent Struggle - Taking Charge of ADHD in Adults, The Complete Guide To Accept Yourself, Embrace Neurodiversity, Master Your Moods, Improve Relationships, Stay OrgaDocument134 pagesL. William Ross-Child M.L.C. - The Silent Struggle - Taking Charge of ADHD in Adults, The Complete Guide To Accept Yourself, Embrace Neurodiversity, Master Your Moods, Improve Relationships, Stay Orga8v6275csj8Pas encore d'évaluation
- AsfdafsdDocument125 pagesAsfdafsdfrankmalcovPas encore d'évaluation
- Males and Eating Disorders: William HarrymanDocument14 pagesMales and Eating Disorders: William HarrymanWilliam HarrymanPas encore d'évaluation
- Managing Depression, Growing Older - A Guide For Professionals and Carers (PDFDrive)Document300 pagesManaging Depression, Growing Older - A Guide For Professionals and Carers (PDFDrive)Dermot HegartyPas encore d'évaluation
- Positive and Negative Reinforcement Handout 1Document1 pagePositive and Negative Reinforcement Handout 1Ивона Шујак100% (1)
- 2015 Book TranslationalApproachesToAutis PDFDocument222 pages2015 Book TranslationalApproachesToAutis PDFCarolina FalconPas encore d'évaluation
- GENSLER - 2012 - Autism Spectrum Disorder in DSM-VDocument11 pagesGENSLER - 2012 - Autism Spectrum Disorder in DSM-VLoratadinaPas encore d'évaluation
- Explore Treatment - How d0 We Know The Medication Is WorkingDocument9 pagesExplore Treatment - How d0 We Know The Medication Is WorkingNoel VillanuevaPas encore d'évaluation
- How Neurodiverse People Are Like Hunter-GatherersDocument3 pagesHow Neurodiverse People Are Like Hunter-Gatherersandreas.hoferPas encore d'évaluation
- NIH SleepDocument160 pagesNIH Sleepanomika100% (1)
- Learning Styles and AutismDocument2 pagesLearning Styles and AutismMelita BezjakPas encore d'évaluation
- The Little Book of Child and Adolescent DevelopmentDocument249 pagesThe Little Book of Child and Adolescent Developmentzane deguiaPas encore d'évaluation
- Guía de TOCDocument96 pagesGuía de TOCkarlunchoPas encore d'évaluation
- Six Super Skills For Executive FunctioningDocument178 pagesSix Super Skills For Executive Functioningsupervisão ABA construirPas encore d'évaluation
- Sheehan Anxiety ScaleDocument2 pagesSheehan Anxiety ScaleSisy AnandaPas encore d'évaluation
- Psychology TypesDocument10 pagesPsychology TypesFiza IshtiaqPas encore d'évaluation
- Bully-Proof Your Kid EngDocument14 pagesBully-Proof Your Kid EngJustynaBorowskaPas encore d'évaluation
- Mental Models The Most Effective Techniques To Go From Negative Thinking To Critical Thinking. How To Revamp Your Inner Self, - (Dr. Kevin Carol Miyake) (Z-Library)Document105 pagesMental Models The Most Effective Techniques To Go From Negative Thinking To Critical Thinking. How To Revamp Your Inner Self, - (Dr. Kevin Carol Miyake) (Z-Library)Rucsandra MurzeaPas encore d'évaluation
- Understanding Bipolar Disorder The Essential Family Guide (BPD) (Aimee Daramus)Document151 pagesUnderstanding Bipolar Disorder The Essential Family Guide (BPD) (Aimee Daramus)Tanvi Gupta100% (1)
- 12 Proven Steps For Overcoming Addictions COVER EbookDocument52 pages12 Proven Steps For Overcoming Addictions COVER Ebooknobertrotich12Pas encore d'évaluation
- Guia General para Sobrevivir en El TDAHDocument11 pagesGuia General para Sobrevivir en El TDAHRenzo Villanueva GomezPas encore d'évaluation
- Gifted Underachievers Spiderorganizer HandoutDocument1 pageGifted Underachievers Spiderorganizer Handoutapi-261821900Pas encore d'évaluation
- MCG 2009 03 Raman 200954 SDC1Document14 pagesMCG 2009 03 Raman 200954 SDC1raanja2Pas encore d'évaluation
- Nutrition Therapy For Cardiovascular DiseaseDocument3 pagesNutrition Therapy For Cardiovascular DiseaseSanny RamosPas encore d'évaluation
- EXERCISE 2 - Menu Planning - Food Guide PyramiDocument2 pagesEXERCISE 2 - Menu Planning - Food Guide PyramiFranz goPas encore d'évaluation
- Nutritional Assessment FormulasDocument28 pagesNutritional Assessment Formulas2begeniusPas encore d'évaluation
- A Cross-Sectional Comparison of The Whole Blood Fatty Acid Profile and Omega-3 Index of Male Vegan ADocument10 pagesA Cross-Sectional Comparison of The Whole Blood Fatty Acid Profile and Omega-3 Index of Male Vegan AAndrés Felipe Gutiérrez RodríguezPas encore d'évaluation
- Vaping Final DraftDocument4 pagesVaping Final Draftapi-386991730Pas encore d'évaluation
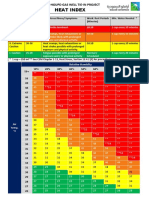
- Aramco Heat Index A4Document1 pageAramco Heat Index A4DLPS HSEPas encore d'évaluation
- Week7 EimDocument11 pagesWeek7 EimJessy LimiacPas encore d'évaluation
- ICDSDocument28 pagesICDSमयंक सिंहPas encore d'évaluation
- Diet in Pregnancy and LactationDocument8 pagesDiet in Pregnancy and LactationSumeet GuptaPas encore d'évaluation
- Community Nutrition QuizDocument3 pagesCommunity Nutrition QuizAli Aufar HutasuhutPas encore d'évaluation
- Burke (2007) Nutritional Strategies For The MarathonDocument5 pagesBurke (2007) Nutritional Strategies For The MarathonMario Pérez100% (1)
- RecyclingDocument4 pagesRecyclingShaneika Davidson-FrancisPas encore d'évaluation
- PAT B. Inggris Kelas 5Document115 pagesPAT B. Inggris Kelas 5aiunPas encore d'évaluation
- Effects of Smoking On Family LifeDocument3 pagesEffects of Smoking On Family LifeDeepPas encore d'évaluation
- Stress and AdaptationDocument15 pagesStress and AdaptationbindiyaPas encore d'évaluation
- 10 Myths About Losing WeightDocument25 pages10 Myths About Losing WeightMrModi mohamed100% (5)
- TsoDocument256 pagesTsoMatthew Edwards92% (12)
- Determinan Pemberian ASI Eksklusif Di Sleman: Determinants of Exclusive Breastfeeding in SlemanDocument6 pagesDeterminan Pemberian ASI Eksklusif Di Sleman: Determinants of Exclusive Breastfeeding in SlemanRia UtamiPas encore d'évaluation
- ASPIRE Sport Science Research Publications Sept 2013Document25 pagesASPIRE Sport Science Research Publications Sept 2013pdelcampo1991Pas encore d'évaluation
- Cancer QuizDocument3 pagesCancer QuizOsama AtifPas encore d'évaluation
- MMA - 1 Week Workout PlanDocument3 pagesMMA - 1 Week Workout PlannehapanditayinPas encore d'évaluation
- Destroying Fat ThibaudeuDocument31 pagesDestroying Fat ThibaudeuOrlando Paez Cortazar100% (1)
- 1 of 36 © Boardworks LTD 2006Document36 pages1 of 36 © Boardworks LTD 2006Mariam El KhatibPas encore d'évaluation
- Ramadan and Football: Sports ScienceDocument4 pagesRamadan and Football: Sports ScienceCherbiti Mohammed AminePas encore d'évaluation
- Community MedicineDocument4 pagesCommunity MedicineEthan HuntPas encore d'évaluation
- Physical Fitness: Ma'am Crisele Iris B. HidocosDocument21 pagesPhysical Fitness: Ma'am Crisele Iris B. HidocosCrisele HidocosPas encore d'évaluation
- Fundamentals in Food Science TechnologyDocument2 pagesFundamentals in Food Science TechnologyJenny BelarminoPas encore d'évaluation
- Who Aap Database May2016Document24 pagesWho Aap Database May2016Shreya ChhabraPas encore d'évaluation
- Health7 Q2 Mod5EatingDisorder v2Document26 pagesHealth7 Q2 Mod5EatingDisorder v2Dhezerie Anne PosadasPas encore d'évaluation
- The Comfort of Crows: A Backyard YearD'EverandThe Comfort of Crows: A Backyard YearÉvaluation : 4.5 sur 5 étoiles4.5/5 (23)
- The Obesity Code: Unlocking the Secrets of Weight LossD'EverandThe Obesity Code: Unlocking the Secrets of Weight LossÉvaluation : 4 sur 5 étoiles4/5 (6)
- Why We Die: The New Science of Aging and the Quest for ImmortalityD'EverandWhy We Die: The New Science of Aging and the Quest for ImmortalityÉvaluation : 4.5 sur 5 étoiles4.5/5 (6)
- Summary: Outlive: The Science and Art of Longevity by Peter Attia MD, With Bill Gifford: Key Takeaways, Summary & AnalysisD'EverandSummary: Outlive: The Science and Art of Longevity by Peter Attia MD, With Bill Gifford: Key Takeaways, Summary & AnalysisÉvaluation : 4.5 sur 5 étoiles4.5/5 (44)
- To Explain the World: The Discovery of Modern ScienceD'EverandTo Explain the World: The Discovery of Modern ScienceÉvaluation : 3.5 sur 5 étoiles3.5/5 (51)
- Dark Matter and the Dinosaurs: The Astounding Interconnectedness of the UniverseD'EverandDark Matter and the Dinosaurs: The Astounding Interconnectedness of the UniverseÉvaluation : 3.5 sur 5 étoiles3.5/5 (69)
- Sugar Crush: How to Reduce Inflammation, Reverse Nerve Damage, and Reclaim Good HealthD'EverandSugar Crush: How to Reduce Inflammation, Reverse Nerve Damage, and Reclaim Good HealthÉvaluation : 4 sur 5 étoiles4/5 (6)
- Summary: Limitless: Upgrade Your Brain, Learn Anything Faster, and Unlock Your Exceptional Life By Jim Kwik: Key Takeaways, Summary and AnalysisD'EverandSummary: Limitless: Upgrade Your Brain, Learn Anything Faster, and Unlock Your Exceptional Life By Jim Kwik: Key Takeaways, Summary and AnalysisÉvaluation : 5 sur 5 étoiles5/5 (8)
- Lessons for Survival: Mothering Against “the Apocalypse”D'EverandLessons for Survival: Mothering Against “the Apocalypse”Évaluation : 5 sur 5 étoiles5/5 (2)
- When the Body Says No by Gabor Maté: Key Takeaways, Summary & AnalysisD'EverandWhen the Body Says No by Gabor Maté: Key Takeaways, Summary & AnalysisÉvaluation : 3.5 sur 5 étoiles3.5/5 (2)
- The Marshmallow Test: Mastering Self-ControlD'EverandThe Marshmallow Test: Mastering Self-ControlÉvaluation : 4.5 sur 5 étoiles4.5/5 (60)
- 10% Human: How Your Body's Microbes Hold the Key to Health and HappinessD'Everand10% Human: How Your Body's Microbes Hold the Key to Health and HappinessÉvaluation : 4 sur 5 étoiles4/5 (33)
- Under Alien Skies: A Sightseer's Guide to the UniverseD'EverandUnder Alien Skies: A Sightseer's Guide to the UniverseÉvaluation : 4.5 sur 5 étoiles4.5/5 (17)
- The Story of Philosophy: The Lives and Opinions of the Greater PhilosophersD'EverandThe Story of Philosophy: The Lives and Opinions of the Greater PhilosophersPas encore d'évaluation
- Alex & Me: How a Scientist and a Parrot Discovered a Hidden World of Animal Intelligence—and Formed a Deep Bond in the ProcessD'EverandAlex & Me: How a Scientist and a Parrot Discovered a Hidden World of Animal Intelligence—and Formed a Deep Bond in the ProcessPas encore d'évaluation
- Critical Care: A New Nurse Faces Death, Life, and Everything in BetweenD'EverandCritical Care: A New Nurse Faces Death, Life, and Everything in BetweenÉvaluation : 3.5 sur 5 étoiles3.5/5 (159)
- A Brief History of Intelligence: Evolution, AI, and the Five Breakthroughs That Made Our BrainsD'EverandA Brief History of Intelligence: Evolution, AI, and the Five Breakthroughs That Made Our BrainsÉvaluation : 4.5 sur 5 étoiles4.5/5 (6)
- Return of the God Hypothesis: Three Scientific Discoveries That Reveal the Mind Behind the UniverseD'EverandReturn of the God Hypothesis: Three Scientific Discoveries That Reveal the Mind Behind the UniverseÉvaluation : 4.5 sur 5 étoiles4.5/5 (52)
- Sully: The Untold Story Behind the Miracle on the HudsonD'EverandSully: The Untold Story Behind the Miracle on the HudsonÉvaluation : 4 sur 5 étoiles4/5 (103)
- Periodic Tales: A Cultural History of the Elements, from Arsenic to ZincD'EverandPeriodic Tales: A Cultural History of the Elements, from Arsenic to ZincÉvaluation : 3.5 sur 5 étoiles3.5/5 (137)
- Knocking on Heaven's Door: How Physics and Scientific Thinking Illuminate the Universe and the Modern WorldD'EverandKnocking on Heaven's Door: How Physics and Scientific Thinking Illuminate the Universe and the Modern WorldÉvaluation : 3.5 sur 5 étoiles3.5/5 (64)