Vous aimerez peut-être aussi
- Improve Patient Safety by Reducing Medication ErrorsDocument95 pagesImprove Patient Safety by Reducing Medication Errorsdev5683Pas encore d'évaluation
- Intestinal Stomas - AKTDocument49 pagesIntestinal Stomas - AKTTammie YoungPas encore d'évaluation
- Large Bowel Obstruction by Nic MDocument42 pagesLarge Bowel Obstruction by Nic MRisky OpponentPas encore d'évaluation
- 21 GMS Bedah JantungDocument140 pages21 GMS Bedah JantungNuravif SetianingrumPas encore d'évaluation
- PolicyDocument55 pagesPolicyBanePas encore d'évaluation
- Bowel AnastomosisDocument30 pagesBowel AnastomosismrashaiedehPas encore d'évaluation
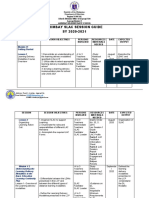
- Arimbay Slac Session Guide SY 2020-2021Document6 pagesArimbay Slac Session Guide SY 2020-2021Jen ApinadoPas encore d'évaluation
- Portal Hypertension SurgeryDocument6 pagesPortal Hypertension SurgeryjackSNMMCPas encore d'évaluation
- Jurnal CA TyroidDocument4 pagesJurnal CA TyroidErvina ZelfiPas encore d'évaluation
- Case Presentation:: DR - Amra Farrukh PG.T Su.IDocument75 pagesCase Presentation:: DR - Amra Farrukh PG.T Su.IpeeconPas encore d'évaluation
- Hepatocellular Carcinoma: Review ArticleDocument13 pagesHepatocellular Carcinoma: Review ArticleAnnagiulia Gramenzi100% (2)
- Midwifery Competencies and ConceptsDocument10 pagesMidwifery Competencies and Conceptsannu panchalPas encore d'évaluation
- Acute Limb Ischemic: Divisi Bedah Vaskular Melfrits R Siwabessy, MDDocument26 pagesAcute Limb Ischemic: Divisi Bedah Vaskular Melfrits R Siwabessy, MDMelfrits SiwabessyPas encore d'évaluation
- Case Study CholecytitisDocument3 pagesCase Study CholecytitisLucero HyacinthPas encore d'évaluation
- Preparation and Indications for ColonoscopyDocument14 pagesPreparation and Indications for Colonoscopyyaba100% (1)
- Chole SysDocument8 pagesChole SysKas MulyadiPas encore d'évaluation
- Sejarah Dan Perkembangan Ilmu Bedah September 2017Document18 pagesSejarah Dan Perkembangan Ilmu Bedah September 2017Arief Fakhrizal100% (1)
- Isthmocele Uterin: A Propos de Quatre CasDocument7 pagesIsthmocele Uterin: A Propos de Quatre CasIJAR JOURNALPas encore d'évaluation
- Gastric Perforation in The Newborn: Ai-Xuan Le Holterman, M.DDocument23 pagesGastric Perforation in The Newborn: Ai-Xuan Le Holterman, M.Dpldhy2004Pas encore d'évaluation
- Colorectal Screening AlgorithmDocument12 pagesColorectal Screening Algorithmsavvy_as_98Pas encore d'évaluation
- Benign and Malignant Lesion of Lower GIDocument45 pagesBenign and Malignant Lesion of Lower GIAhmad Alzu3bePas encore d'évaluation
- Rise of Modern Surgery OrigiDocument46 pagesRise of Modern Surgery OrigiPriyanka KaranamPas encore d'évaluation
- Schwartz2002 PDFDocument7 pagesSchwartz2002 PDFnova sorayaPas encore d'évaluation
- Management of The Pancreatic Remnant During Whipple OperationDocument4 pagesManagement of The Pancreatic Remnant During Whipple OperationYacine Tarik Aizel100% (1)
- Subtotal Cholecystectomy-''Fenestrating'' Vs ''Reconstituting'' Subtypes and The Prevention of Bile Duct Injury - Definition of The Optimal Procedure In  Difficult Operative ConditionsDocument8 pagesSubtotal Cholecystectomy-''Fenestrating'' Vs ''Reconstituting'' Subtypes and The Prevention of Bile Duct Injury - Definition of The Optimal Procedure In  Difficult Operative ConditionsBolivar Isea100% (1)
- Surgery Critical View - StrasbergDocument7 pagesSurgery Critical View - Strasbergjoseaugustorojas9414Pas encore d'évaluation
- Safe Laparoscopic Cholecystectomy: Presenter: DR Anand Ujjwal SinghDocument58 pagesSafe Laparoscopic Cholecystectomy: Presenter: DR Anand Ujjwal SinghUmer KhanPas encore d'évaluation
- Clinical Diognosis ColorectalDocument2 pagesClinical Diognosis ColorectalRizal Sven VollfiedPas encore d'évaluation
- Bacterial Translocation in The GutDocument29 pagesBacterial Translocation in The GutdonkeyendutPas encore d'évaluation
- Updated review of diagnosis and treatment of cystic hepatic lesionsDocument8 pagesUpdated review of diagnosis and treatment of cystic hepatic lesionsMayerlin CalvachePas encore d'évaluation
- Paper Presentation On Trichobezoars A Hairy Cause of Intestinal ObstructionDocument14 pagesPaper Presentation On Trichobezoars A Hairy Cause of Intestinal ObstructionAimanPas encore d'évaluation
- Anatomy of The AxillarDocument43 pagesAnatomy of The AxillarJustine NyangaresiPas encore d'évaluation
- GEN GallBladderInstrumentsADocument10 pagesGEN GallBladderInstrumentsANeo Rodriguez AlvaradoPas encore d'évaluation
- Faculty of Medicine NR - Ii Department of Surgery NR - Ii: Diseases of The Biliary TractDocument40 pagesFaculty of Medicine NR - Ii Department of Surgery NR - Ii: Diseases of The Biliary TractGalina LozovanuPas encore d'évaluation
- Abdominal Wall Extraskeletal Ewing Sarcoma - Case ReportDocument3 pagesAbdominal Wall Extraskeletal Ewing Sarcoma - Case ReportInternational Organization of Scientific Research (IOSR)Pas encore d'évaluation
- Dukes' Classification of Rectal CancerDocument3 pagesDukes' Classification of Rectal CancerDeba P SarmaPas encore d'évaluation
- Short Bowel SyndromeDocument64 pagesShort Bowel Syndromeeztouch12Pas encore d'évaluation
- Jurnal Fistolotomi Vs FistulektomiDocument8 pagesJurnal Fistolotomi Vs FistulektomiAndriati Nadhila100% (1)
- Bladder Substitution and Urinary DiversionDocument58 pagesBladder Substitution and Urinary DiversionlifespotPas encore d'évaluation
- Early Breast Cancer TherapyDocument20 pagesEarly Breast Cancer TherapyIpseet MishraPas encore d'évaluation
- HirschprungDocument13 pagesHirschprungfitra hayatiPas encore d'évaluation
- Gynecology and ObstetricsDocument125 pagesGynecology and Obstetricsapi-3712326100% (4)
- The Age of AIDS Study Guide Part 1 (KEY)Document4 pagesThe Age of AIDS Study Guide Part 1 (KEY)owls_110250% (2)
- Bladder PDFDocument117 pagesBladder PDFimranqazi11Pas encore d'évaluation
- Systemic Therapies of CRC: Johan KurniandaDocument56 pagesSystemic Therapies of CRC: Johan KurniandaANISA RACHMITA ARIANTI 2020Pas encore d'évaluation
- Guidelines For The Management of Hiatal HerniaDocument42 pagesGuidelines For The Management of Hiatal HerniaKarina Montecinos GodinezPas encore d'évaluation
- The Liver: Dr. I Made Naris Pujawan, M.Biomed, SP - PADocument19 pagesThe Liver: Dr. I Made Naris Pujawan, M.Biomed, SP - PAAnonymous D29e00Pas encore d'évaluation
- CraniotomyDocument20 pagesCraniotomyhemihemaPas encore d'évaluation
- Diaphragma InjuryDocument18 pagesDiaphragma InjuryAhmedPas encore d'évaluation
- Beautiful Mind and Shutter IslandDocument6 pagesBeautiful Mind and Shutter IslandlynnmalicPas encore d'évaluation
- Biotechnology: December 2015Document27 pagesBiotechnology: December 2015Lovely LeninPas encore d'évaluation
- According To CSS Conducted By, in Partnership With The University of Maryland Conducted in 200 CountriesDocument3 pagesAccording To CSS Conducted By, in Partnership With The University of Maryland Conducted in 200 CountriesShipra BaruaPas encore d'évaluation
- Comparative Study Between Open Fistulectomy and Ligation of Intersphincteric Fistulas Tract (LIFT) Procedure For Uncomplicated Perianal FistulaDocument7 pagesComparative Study Between Open Fistulectomy and Ligation of Intersphincteric Fistulas Tract (LIFT) Procedure For Uncomplicated Perianal FistulaInternational Journal of Innovative Science and Research TechnologyPas encore d'évaluation
- KillipsDocument12 pagesKillipsNhorlyn Adante SoltesPas encore d'évaluation
- Primary Biliary CirrhosisDocument8 pagesPrimary Biliary CirrhosisAhmed TeebiPas encore d'évaluation
- U04 Fxs of Humeral ShaftDocument88 pagesU04 Fxs of Humeral Shaftadrian_mogosPas encore d'évaluation
- Courvoisier LawDocument1 pageCourvoisier LawSonny SeputraPas encore d'évaluation
- Blunt Adominal TraumaDocument14 pagesBlunt Adominal TraumaMuhammad Bima AkbarPas encore d'évaluation
- The Age of AIDS Stydy Guide Part 1Document4 pagesThe Age of AIDS Stydy Guide Part 1owls_1102100% (1)
- The SAGES Safe Cholecystectomy ProgramDocument4 pagesThe SAGES Safe Cholecystectomy ProgramMikael AngelooPas encore d'évaluation
- Subtotal Cholecystectomye"Fenestrating" Vs "Reconstituting" Subtypes and The Prevention of Bile Duct Injury: Definition of The Optimal Procedure in Difficult Operative ConditionsDocument8 pagesSubtotal Cholecystectomye"Fenestrating" Vs "Reconstituting" Subtypes and The Prevention of Bile Duct Injury: Definition of The Optimal Procedure in Difficult Operative ConditionsAny MafraPas encore d'évaluation
- Colcistectomia FenestradaDocument8 pagesColcistectomia FenestradaLuis David AguileraPas encore d'évaluation
- Safe Cholecystectomy CCXDocument6 pagesSafe Cholecystectomy CCXDr Ankit SharmaPas encore d'évaluation
- Difficult Acute Cholecystitis: Treatment and Technical IssuesD'EverandDifficult Acute Cholecystitis: Treatment and Technical IssuesPas encore d'évaluation
- Bedrikovetski 2020Document10 pagesBedrikovetski 2020Charles CardosoPas encore d'évaluation
- Methods of Colostomy Construction - No Effect On Parastomal Hernia Rate Results From Stoma-const-A Randomized Controlled TrialDocument8 pagesMethods of Colostomy Construction - No Effect On Parastomal Hernia Rate Results From Stoma-const-A Randomized Controlled TrialCharles CardosoPas encore d'évaluation
- Perspective: Mediterranean Biomedical JournalsDocument10 pagesPerspective: Mediterranean Biomedical JournalsCharles CardosoPas encore d'évaluation
- Methods of Colostomy Construction No Effect On.6Document8 pagesMethods of Colostomy Construction No Effect On.6Charles CardosoPas encore d'évaluation
- Dekker 2008Document6 pagesDekker 2008Charles CardosoPas encore d'évaluation
- Critical View - Strasberg PDFDocument7 pagesCritical View - Strasberg PDFLeslyAgredaNavarroPas encore d'évaluation
- Male, Masculinities Methodologies and MethodsDocument40 pagesMale, Masculinities Methodologies and MethodsMarco Rojas VPas encore d'évaluation
- Pilot II: Technical Data SheetDocument4 pagesPilot II: Technical Data SheetSafinahPas encore d'évaluation
- Borror State Street PermitDocument2 pagesBorror State Street PermitMike SmithPas encore d'évaluation
- Surgical Intern Manual (For Pre-Intern) QEHDocument10 pagesSurgical Intern Manual (For Pre-Intern) QEHChris Jardine LiPas encore d'évaluation
- Fearless Approach BlueprintDocument23 pagesFearless Approach Blueprintaryanbharadwaj12Pas encore d'évaluation
- COS4840 - Chapter 05Document30 pagesCOS4840 - Chapter 05Surya EtikaPas encore d'évaluation
- 952-Article Text-3024-1-10-20221113Document13 pages952-Article Text-3024-1-10-20221113Audi GaluhPas encore d'évaluation
- Zygomatic ImplantsDocument3 pagesZygomatic ImplantsDeb SPas encore d'évaluation
- SALIVIO BSN 1-5 - Rest and Sleep InfographicsDocument1 pageSALIVIO BSN 1-5 - Rest and Sleep InfographicsNikki SalivioPas encore d'évaluation
- The Role of Social Worker in Community Development: ArticleDocument4 pagesThe Role of Social Worker in Community Development: ArticleTushar GautamPas encore d'évaluation
- Kelly's Panel Hospital: Hospital Name Address Tel No Kuala LumpurDocument9 pagesKelly's Panel Hospital: Hospital Name Address Tel No Kuala LumpurSEAN LAIPas encore d'évaluation
- Integrating Food Sensitive Planning and Urban Design Into Urban Governance ActionsDocument22 pagesIntegrating Food Sensitive Planning and Urban Design Into Urban Governance ActionsAurelia chandraPas encore d'évaluation
- PsikopatologiDocument25 pagesPsikopatologiShella Thea WibawaPas encore d'évaluation
- Carlosa Es Localized Child Protection PolicyDocument9 pagesCarlosa Es Localized Child Protection PolicymonalisaPas encore d'évaluation
- MCN SF Chapter 18 QuizDocument4 pagesMCN SF Chapter 18 QuizKathleen AngPas encore d'évaluation
- Security Assessment &recommendation: PurposeDocument3 pagesSecurity Assessment &recommendation: PurposeEricka W.Pas encore d'évaluation
- Kualitas Menu, Pola Menu, Ketersediaan Energi Dan Zat Gizi Pada Menu Makan Sahur Dan Berbuka Puasa Selama Ramadhan Untuk Penghuni AsramaDocument11 pagesKualitas Menu, Pola Menu, Ketersediaan Energi Dan Zat Gizi Pada Menu Makan Sahur Dan Berbuka Puasa Selama Ramadhan Untuk Penghuni Asramarizky NugrohoPas encore d'évaluation
- Atomic Energy Central School student highlights benefits of water, sanitation & hygieneDocument8 pagesAtomic Energy Central School student highlights benefits of water, sanitation & hygieneNirakjPas encore d'évaluation
- Lesson on Recreation and Leisure ActivitiesDocument5 pagesLesson on Recreation and Leisure Activitiesruth lopezPas encore d'évaluation
- St. Paul College of Ilocos SurDocument5 pagesSt. Paul College of Ilocos SurCharina AubreyPas encore d'évaluation
- Medical For Athletes 1Document2 pagesMedical For Athletes 1carmina duldulaoPas encore d'évaluation
- Department of Education: Tagana-An National High SchoolDocument2 pagesDepartment of Education: Tagana-An National High SchoolGinevieve GibertasPas encore d'évaluation
- Ticket To Class - SLS Scenario 32 - Arthur HarrisDocument3 pagesTicket To Class - SLS Scenario 32 - Arthur HarrisLisa HoheiselPas encore d'évaluation
- The School Canteen Follows Guidelines On Operational Management Set by The Department of Education Through DepEd Order NoDocument3 pagesThe School Canteen Follows Guidelines On Operational Management Set by The Department of Education Through DepEd Order NoChristian Lloyd Latayan64% (14)
- CDC1 Bookofreadings1Document74 pagesCDC1 Bookofreadings1Sylvester ViholmPas encore d'évaluation
- E-Palaro-Form-2018-2020 (1) TAMADocument257 pagesE-Palaro-Form-2018-2020 (1) TAMALadyAngelIgnacioValgunaPas encore d'évaluation