Vous aimerez peut-être aussi
- Clinical Examination - Aids To The Examination of The Peripheral Nervous SystemDocument66 pagesClinical Examination - Aids To The Examination of The Peripheral Nervous Systemsarahecahill100% (3)
- Aids To The Examination of The Peripheral Nervous System 4th Edition 2000Document67 pagesAids To The Examination of The Peripheral Nervous System 4th Edition 2000Dwi Andriyani NimanPas encore d'évaluation
- Essential Clinically Applied Anatomy of the Peripheral Nervous System in the Head and NeckD'EverandEssential Clinically Applied Anatomy of the Peripheral Nervous System in the Head and NeckPas encore d'évaluation
- Electromyography in CNS Disorders: Central EMGD'EverandElectromyography in CNS Disorders: Central EMGBhagwan T. ShahaniPas encore d'évaluation
- Anatomy, Imaging and Surgery of The Intracranial Dural Venous SinusesDocument255 pagesAnatomy, Imaging and Surgery of The Intracranial Dural Venous SinusesmuelmiharPas encore d'évaluation
- Somatic Dysfunction in FM PDFDocument25 pagesSomatic Dysfunction in FM PDFHailey0% (1)
- Headache and Facial Pain (What Do I Do Now), 2nd Edition (Lawrence Newman, Morris Levin, Rashmi Halker Etc.) (Z-Library)Document233 pagesHeadache and Facial Pain (What Do I Do Now), 2nd Edition (Lawrence Newman, Morris Levin, Rashmi Halker Etc.) (Z-Library)ALZAHRA AlkhutariPas encore d'évaluation
- Interventional Spine Procedures A Case-Based Approach PDFDocument215 pagesInterventional Spine Procedures A Case-Based Approach PDFdrhms2000100% (2)
- Osteopathic Medicine RecallDocument186 pagesOsteopathic Medicine RecallDaniel Lopes100% (1)
- Vestibular DisorderDocument417 pagesVestibular DisorderDEEKSHA ABROLPas encore d'évaluation
- Anatomi PelvisDocument44 pagesAnatomi Pelvisari naPas encore d'évaluation
- Modern Concepts of Peripheral Nerve RepairDocument144 pagesModern Concepts of Peripheral Nerve RepairRazvannusPas encore d'évaluation
- Bogduk 2009Document3 pagesBogduk 2009Borys100% (1)
- Practical Skills On PalpationDocument6 pagesPractical Skills On PalpationsudersonPas encore d'évaluation
- Atlas of Anatomy of The Peripheral NervesDocument346 pagesAtlas of Anatomy of The Peripheral Nervesfasferreira8880% (5)
- 044307402XPeripheral RarDocument165 pages044307402XPeripheral RarmahenderPas encore d'évaluation
- Needle EMG Muscle IdentificationDocument13 pagesNeedle EMG Muscle Identificationemilio9fernandez9gat100% (1)
- Brain and Bannisters Clinical Neurology Oxford Medical Publications by Roger Bannister PDFDocument7 pagesBrain and Bannisters Clinical Neurology Oxford Medical Publications by Roger Bannister PDFBennat RajPas encore d'évaluation
- Methods For Assessing Leg Length DiscrepancyDocument13 pagesMethods For Assessing Leg Length DiscrepancyKanika SinhaPas encore d'évaluation
- Tech RGNL 1 Nerve Conduction Studies KatirjiDocument52 pagesTech RGNL 1 Nerve Conduction Studies KatirjiSinduja Jayaraj100% (1)
- (Douglas W. Zochodne) Neurobiology of Peripheral NDocument318 pages(Douglas W. Zochodne) Neurobiology of Peripheral NImmer Armendáriz BetancourtPas encore d'évaluation
- Measurement and Scales Used in PhysiotherapyDocument38 pagesMeasurement and Scales Used in PhysiotherapyAnurag BhuyanPas encore d'évaluation
- Peripheral Vs Central Vestibular DisordersDocument2 pagesPeripheral Vs Central Vestibular DisordersraraPas encore d'évaluation
- Mark Dutton - Manual Therapy of The Spine - An Integrated Approach-Appleton & Lange (2001)Document626 pagesMark Dutton - Manual Therapy of The Spine - An Integrated Approach-Appleton & Lange (2001)Suhani Mihai100% (1)
- Lumbopelvic Stability: SyllabusDocument13 pagesLumbopelvic Stability: Syllabusrapannika100% (3)
- Essential Musculoskeletal MRI - A Primer For The Clinician (PDFDrive)Document270 pagesEssential Musculoskeletal MRI - A Primer For The Clinician (PDFDrive)Thamiris RosaPas encore d'évaluation
- Orthopaedic NeurologyDocument134 pagesOrthopaedic NeurologyRaymond Parung100% (1)
- Women's Health Diploma ProgramDocument3 pagesWomen's Health Diploma ProgramMahmoud Abo AlfaPas encore d'évaluation
- Functional Neurology For Practitioners of Manual Medicine Ebook - Randy W. BeckDocument5 pagesFunctional Neurology For Practitioners of Manual Medicine Ebook - Randy W. Beckbufanago0% (2)
- An Osteopathic Approach To Children - Jane Elizabeth Carreiro DODocument4 pagesAn Osteopathic Approach To Children - Jane Elizabeth Carreiro DOdekeguryPas encore d'évaluation
- Sample Emg/Ncv Report - Normal StudyDocument5 pagesSample Emg/Ncv Report - Normal StudyPhysiotherapist AliPas encore d'évaluation
- Internal Derangements of Joints PDFDocument2 335 pagesInternal Derangements of Joints PDFCarmen FandiñoPas encore d'évaluation
- Nerve Pathways - Functions, Lesions and AdhesionsDocument33 pagesNerve Pathways - Functions, Lesions and Adhesionshajra habibPas encore d'évaluation
- PDF Document PDFDocument8 pagesPDF Document PDFDhruv AgrawalPas encore d'évaluation
- Essentials of Skeletal Radiology (2 Vol. Set)Document4 pagesEssentials of Skeletal Radiology (2 Vol. Set)gufaxite0% (1)
- Red Flags II. A Guide To Solving Serious Pathology of The Spine-Churchill Livingstone (2009)Document240 pagesRed Flags II. A Guide To Solving Serious Pathology of The Spine-Churchill Livingstone (2009)Oana MozaPas encore d'évaluation
- ACFrOgCQoS 8vusEkJ5naUqf0VaiLqAOGXIBMd9DGkNkrYbScqPgbzgpsPpIMAv1RXhsxOnjPh34IDbAypkIW udLxG6DcvF6bb5lf aXqRBjiJvDAyXfdTMdvNozVsDocument1 200 pagesACFrOgCQoS 8vusEkJ5naUqf0VaiLqAOGXIBMd9DGkNkrYbScqPgbzgpsPpIMAv1RXhsxOnjPh34IDbAypkIW udLxG6DcvF6bb5lf aXqRBjiJvDAyXfdTMdvNozVsMarlon Pereira100% (3)
- Neural Mobilizationw10Document33 pagesNeural Mobilizationw10manjukumard2007Pas encore d'évaluation
- ElectromyographyDocument15 pagesElectromyographyAnonymous -Pas encore d'évaluation
- Brain and Bannisters Clinical Neurology Oxford Medical Publications by Roger Bannister PDFDocument7 pagesBrain and Bannisters Clinical Neurology Oxford Medical Publications by Roger Bannister PDFBennat RajPas encore d'évaluation
- Muscular Dystrophy BookDocument425 pagesMuscular Dystrophy Booklakshmipathi TPas encore d'évaluation
- Eyal Lederman - Process Approach in PTDocument72 pagesEyal Lederman - Process Approach in PTYuldash100% (1)
- Turocy Strain Counterstrain PATS06Document46 pagesTurocy Strain Counterstrain PATS06Yap Grace K Xiulin100% (2)
- Course Material - Manual TherapyDocument196 pagesCourse Material - Manual Therapypuntocom111100% (1)
- Advances in Spinal Stabilization PDFDocument333 pagesAdvances in Spinal Stabilization PDFMateo CortesPas encore d'évaluation
- The Pettibon Spinal Biomechanics SystemDocument67 pagesThe Pettibon Spinal Biomechanics Systemcristian darabanPas encore d'évaluation
- Thoracic Spine and Ribs PDFDocument334 pagesThoracic Spine and Ribs PDFSurender DhillonPas encore d'évaluation
- Clinical Neurophysiology of The Vestibular System (001-057) PDFDocument57 pagesClinical Neurophysiology of The Vestibular System (001-057) PDFAriel CarterPas encore d'évaluation
- Basic Principles of Peripheral Nerve DisordersDocument288 pagesBasic Principles of Peripheral Nerve DisordersJosé Ramírez100% (1)
- Neuromuscular ImagingDocument432 pagesNeuromuscular ImagingLeticiaElizabethEchevarria100% (2)
- 1473 The Bohemian ThrustDocument8 pages1473 The Bohemian ThrustRichard TonsingPas encore d'évaluation
- MSK Us ProtocolsDocument40 pagesMSK Us Protocolsjamir59Pas encore d'évaluation
- Approaches To Therapeutic Exercise and Activity For NeurologicalDocument69 pagesApproaches To Therapeutic Exercise and Activity For NeurologicalPedro M. BorgesPas encore d'évaluation
- Yasser El Miedany Musculoskeletal Ultrasound Guided RegenerativeDocument554 pagesYasser El Miedany Musculoskeletal Ultrasound Guided RegenerativeMarielly EllerPas encore d'évaluation
- Chiropractic Green Books - V09 - 1923Document582 pagesChiropractic Green Books - V09 - 1923Fabio DiasPas encore d'évaluation
- Spine PhenotypesD'EverandSpine PhenotypesDino SamartzisPas encore d'évaluation
- Interactions between the Craniomandibular System and Cervical Spine: The influence of an unilateral change of occlusion on the upper cervical range of motionD'EverandInteractions between the Craniomandibular System and Cervical Spine: The influence of an unilateral change of occlusion on the upper cervical range of motionPas encore d'évaluation
- Movements and Orthopedic Tests: quick, easy, and reliableD'EverandMovements and Orthopedic Tests: quick, easy, and reliablePas encore d'évaluation
- Orthopaedic Management in Cerebral Palsy, 2nd EditionD'EverandOrthopaedic Management in Cerebral Palsy, 2nd EditionHelen Meeks HorstmannÉvaluation : 3 sur 5 étoiles3/5 (2)
- Ankle TappingDocument4 pagesAnkle TappingSenthilkumar ThiyagarajanPas encore d'évaluation
- Ankle TappingDocument4 pagesAnkle TappingSenthilkumar ThiyagarajanPas encore d'évaluation
- Cervical ExerciseDocument1 pageCervical ExerciseSenthilkumar Thiyagarajan100% (1)
- Abdominal IncisionsDocument9 pagesAbdominal IncisionsSenthilkumar ThiyagarajanPas encore d'évaluation
- Anatomymnemonics PDFDocument28 pagesAnatomymnemonics PDFSenthilkumar ThiyagarajanPas encore d'évaluation
- Abdominal Stretching ExsDocument1 pageAbdominal Stretching ExsSenthilkumar ThiyagarajanPas encore d'évaluation
- Hand Gliding Exercise After SurgeryDocument10 pagesHand Gliding Exercise After SurgerySenthilkumar ThiyagarajanPas encore d'évaluation
- Proprioception & Neuromuscular Control Flyer 2009Document3 pagesProprioception & Neuromuscular Control Flyer 2009Senthilkumar ThiyagarajanPas encore d'évaluation
- Postromedial Dic ProlapsDocument3 pagesPostromedial Dic ProlapsSenthilkumar Thiyagarajan100% (1)
- Active Cycle Breathing Technique-Easy DemoDocument3 pagesActive Cycle Breathing Technique-Easy DemoSenthilkumar ThiyagarajanPas encore d'évaluation
- Above Knee Amputation Good One PDFDocument9 pagesAbove Knee Amputation Good One PDFSenthilkumar Thiyagarajan100% (1)
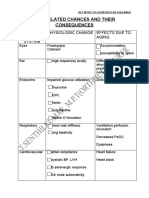
- Age Related Changes and Its Effects in Human Body SystemDocument2 pagesAge Related Changes and Its Effects in Human Body SystemSenthilkumar ThiyagarajanPas encore d'évaluation
- StretchDocument25 pagesStretchSenthilkumar ThiyagarajanPas encore d'évaluation
- StretchDocument25 pagesStretchSenthilkumar ThiyagarajanPas encore d'évaluation
- C:/Documents and Settings/student/Desktop/physiotherapy Protocol FOR HEMIPLEGIC PDFDocument13 pagesC:/Documents and Settings/student/Desktop/physiotherapy Protocol FOR HEMIPLEGIC PDFSenthilkumar ThiyagarajanPas encore d'évaluation
- Human Movements and Its Controlling Muscles - For Physiotherapy and Medical StudentsDocument4 pagesHuman Movements and Its Controlling Muscles - For Physiotherapy and Medical StudentssenthilkumarPas encore d'évaluation
- Basic Brain Anatomy and Physiology PDFDocument10 pagesBasic Brain Anatomy and Physiology PDFSenthilkumar Thiyagarajan100% (3)
- Post Natal Exercise PrescriptionDocument8 pagesPost Natal Exercise PrescriptionSenthilkumar ThiyagarajanPas encore d'évaluation
- Free Exercises For The Upper Limb Lower Limb and SpineDocument14 pagesFree Exercises For The Upper Limb Lower Limb and SpineJatin SimbalPas encore d'évaluation
- Joint and Soft Tissue InjectionsDocument13 pagesJoint and Soft Tissue InjectionsSenthilkumar ThiyagarajanPas encore d'évaluation
- Above Knee Amputation Exc PDFDocument5 pagesAbove Knee Amputation Exc PDFSenthilkumar ThiyagarajanPas encore d'évaluation
- Common Orthopedic TestsDocument7 pagesCommon Orthopedic Testschandran2679Pas encore d'évaluation
- McKenzie Self-Treatments For SciaticaDocument3 pagesMcKenzie Self-Treatments For SciaticaSenthilkumar Thiyagarajan75% (4)
- Orthopedic Assessment For PhysiotherapistDocument3 pagesOrthopedic Assessment For Physiotherapistsenthilkumar76% (21)