Vous aimerez peut-être aussi
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeD'EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeÉvaluation : 4 sur 5 étoiles4/5 (5794)
- The Little Book of Hygge: Danish Secrets to Happy LivingD'EverandThe Little Book of Hygge: Danish Secrets to Happy LivingÉvaluation : 3.5 sur 5 étoiles3.5/5 (400)
- Shoe Dog: A Memoir by the Creator of NikeD'EverandShoe Dog: A Memoir by the Creator of NikeÉvaluation : 4.5 sur 5 étoiles4.5/5 (537)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceD'EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceÉvaluation : 4 sur 5 étoiles4/5 (895)
- The Yellow House: A Memoir (2019 National Book Award Winner)D'EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Évaluation : 4 sur 5 étoiles4/5 (98)
- The Emperor of All Maladies: A Biography of CancerD'EverandThe Emperor of All Maladies: A Biography of CancerÉvaluation : 4.5 sur 5 étoiles4.5/5 (271)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryD'EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryÉvaluation : 3.5 sur 5 étoiles3.5/5 (231)
- Never Split the Difference: Negotiating As If Your Life Depended On ItD'EverandNever Split the Difference: Negotiating As If Your Life Depended On ItÉvaluation : 4.5 sur 5 étoiles4.5/5 (838)
- Grit: The Power of Passion and PerseveranceD'EverandGrit: The Power of Passion and PerseveranceÉvaluation : 4 sur 5 étoiles4/5 (588)
- On Fire: The (Burning) Case for a Green New DealD'EverandOn Fire: The (Burning) Case for a Green New DealÉvaluation : 4 sur 5 étoiles4/5 (73)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureD'EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureÉvaluation : 4.5 sur 5 étoiles4.5/5 (474)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaD'EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaÉvaluation : 4.5 sur 5 étoiles4.5/5 (266)
- The Unwinding: An Inner History of the New AmericaD'EverandThe Unwinding: An Inner History of the New AmericaÉvaluation : 4 sur 5 étoiles4/5 (45)
- Team of Rivals: The Political Genius of Abraham LincolnD'EverandTeam of Rivals: The Political Genius of Abraham LincolnÉvaluation : 4.5 sur 5 étoiles4.5/5 (234)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyD'EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyÉvaluation : 3.5 sur 5 étoiles3.5/5 (2259)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreD'EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreÉvaluation : 4 sur 5 étoiles4/5 (1090)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersD'EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersÉvaluation : 4.5 sur 5 étoiles4.5/5 (344)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)D'EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Évaluation : 4.5 sur 5 étoiles4.5/5 (121)
- Her Body and Other Parties: StoriesD'EverandHer Body and Other Parties: StoriesÉvaluation : 4 sur 5 étoiles4/5 (821)
- ACLS-Study-Guide-2011 MADE EASYDocument2 pagesACLS-Study-Guide-2011 MADE EASYFrances Albaña TevesPas encore d'évaluation
- Nephrotic Syndrome: Jaiganesh.M, M.D (General Medicine) Asst. Professor, S.M.C.HDocument60 pagesNephrotic Syndrome: Jaiganesh.M, M.D (General Medicine) Asst. Professor, S.M.C.HJaiganesh MuruganandamPas encore d'évaluation
- 2022 AHA - ACC - HFSA Heart Failure GuidelinesDocument19 pages2022 AHA - ACC - HFSA Heart Failure GuidelinesGabriel VargasPas encore d'évaluation
- iGA Iforia-ProMRI Mul 393471-J 2017-11-24 EsDocument76 pagesiGA Iforia-ProMRI Mul 393471-J 2017-11-24 EsMartin ArrietaPas encore d'évaluation
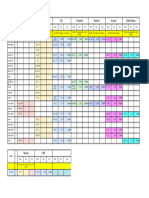
- CMC-Time Table 1st Year MBBS 150620Document1 pageCMC-Time Table 1st Year MBBS 150620KhanPas encore d'évaluation
- Form Mcu JantungDocument5 pagesForm Mcu JantungKomite Medik RS Permata CibuburPas encore d'évaluation
- Ekg Strip NotesDocument13 pagesEkg Strip NotesNick Loizzo100% (2)
- Harrington Brochure 2010Document16 pagesHarrington Brochure 2010tigerlele8356Pas encore d'évaluation
- Care of Patient With TPM Slide PresentationDocument16 pagesCare of Patient With TPM Slide PresentationirzehronPas encore d'évaluation
- Final patho-HCVDDocument2 pagesFinal patho-HCVDAlvin RamirezPas encore d'évaluation
- AAA - Nelsons 20th Summary Part 2Document122 pagesAAA - Nelsons 20th Summary Part 2Jessica MarianoPas encore d'évaluation
- Pearls in CardiologyDocument65 pagesPearls in CardiologyAmber MerrittPas encore d'évaluation
- Flujogramas Europa 2010 Poster RCPDocument9 pagesFlujogramas Europa 2010 Poster RCPMinina Delka MedinaPas encore d'évaluation
- CVS ExamDocument35 pagesCVS Examtravis efraimPas encore d'évaluation
- Or-DR Tally FinalDocument1 pageOr-DR Tally FinalMarvinPas encore d'évaluation
- ACLS Drug Therapy RevisedDocument4 pagesACLS Drug Therapy RevisedpaveethrahPas encore d'évaluation
- OptoxicologypresentationDocument64 pagesOptoxicologypresentationWalaa YousefPas encore d'évaluation
- 7-Cardiology and Respiratory MedicineDocument373 pages7-Cardiology and Respiratory Medicinethisar100% (6)
- Medical Residency Typical Interview QuestionsDocument3 pagesMedical Residency Typical Interview Questionskalpeshgp75% (4)
- End-Stage Renal DiseaseDocument7 pagesEnd-Stage Renal Diseasemarvin de castroPas encore d'évaluation
- 2020 ESC Guidelines For The Management of Adult Congenital Heart Disease (Previously Grown-Up Congenital Heart Disease)Document84 pages2020 ESC Guidelines For The Management of Adult Congenital Heart Disease (Previously Grown-Up Congenital Heart Disease)Liliana BrochadoPas encore d'évaluation
- Valvular Heart DiseaseDocument27 pagesValvular Heart DiseaseOwen J. WiesePas encore d'évaluation
- Cronic Heart Failure - EscDocument55 pagesCronic Heart Failure - EscRisti Graharti100% (1)
- ESC Guidelines For The Management of Acute Myocardial Infarction in Patients Presenting With ST-segment ElevationDocument51 pagesESC Guidelines For The Management of Acute Myocardial Infarction in Patients Presenting With ST-segment Elevationclara amentaPas encore d'évaluation
- Coronary Angiography: A Continuing Education ProgramDocument71 pagesCoronary Angiography: A Continuing Education ProgramVincha R LuqmanPas encore d'évaluation
- DXR Case 2 (Arthur Ingram)Document10 pagesDXR Case 2 (Arthur Ingram)Aloah12234675% (4)
- Congenital Heart DiseasesDocument14 pagesCongenital Heart DiseasesEulane Ferrer100% (1)
- ACLSDocument46 pagesACLSYeoh Hong Shin100% (3)
- Angina Pectoris Pharmacological and Acupuncture TherapyDocument5 pagesAngina Pectoris Pharmacological and Acupuncture TherapyEditor IJTSRDPas encore d'évaluation
- Supraventricular TachycardiaDocument9 pagesSupraventricular TachycardiaclubsanatatePas encore d'évaluation