Vous aimerez peut-être aussi
- The True Story of the "Miracle on the Hudson"D'EverandThe True Story of the "Miracle on the Hudson"Pas encore d'évaluation
- NTSB BAC 060430 Probable CauseDocument2 pagesNTSB BAC 060430 Probable CausebombardierwatchPas encore d'évaluation
- NTSB LJ 090317 Probable CauseDocument2 pagesNTSB LJ 090317 Probable CausebombardierwatchPas encore d'évaluation
- NTSB LJ 061226 Probable CauseDocument2 pagesNTSB LJ 061226 Probable CausebombardierwatchPas encore d'évaluation
- NTSB BAC 081214 Probable CauseDocument2 pagesNTSB BAC 081214 Probable CausebombardierwatchPas encore d'évaluation
- NTSB LJ 990701 Probable CauseDocument3 pagesNTSB LJ 990701 Probable CausebombardierwatchPas encore d'évaluation
- NTSB BAC 060209 Probable CauseDocument2 pagesNTSB BAC 060209 Probable CausebombardierwatchPas encore d'évaluation
- NTSB BAC 030507 Probable CauseDocument2 pagesNTSB BAC 030507 Probable CausebombardierwatchPas encore d'évaluation
- NTSB BAC 100224 Probable CauseDocument2 pagesNTSB BAC 100224 Probable CausebombardierwatchPas encore d'évaluation
- NTSB LJ 060715 Probable CauseDocument2 pagesNTSB LJ 060715 Probable CausebombardierwatchPas encore d'évaluation
- NTSB LJ 990128 Probable CauseDocument2 pagesNTSB LJ 990128 Probable CausebombardierwatchPas encore d'évaluation
- NTSB LJ 071017 Probable CauseDocument2 pagesNTSB LJ 071017 Probable CausebombardierwatchPas encore d'évaluation
- NTSB LJ 010114 Probable CauseDocument3 pagesNTSB LJ 010114 Probable CausebombardierwatchPas encore d'évaluation
- NTSB LJ 040713 Probable CauseDocument2 pagesNTSB LJ 040713 Probable CausebombardierwatchPas encore d'évaluation
- NTSB BAC 070412 Probable CauseDocument2 pagesNTSB BAC 070412 Probable CausebombardierwatchPas encore d'évaluation
- NTSB BAC 050309 Probable CauseDocument2 pagesNTSB BAC 050309 Probable CausebombardierwatchPas encore d'évaluation
- NTSB LJ 990330 Probable CauseDocument2 pagesNTSB LJ 990330 Probable CausebombardierwatchPas encore d'évaluation
- NTSB BAC 050829 Probable CauseDocument2 pagesNTSB BAC 050829 Probable CausebombardierwatchPas encore d'évaluation
- NTSB LJ 040130 Probable CauseDocument2 pagesNTSB LJ 040130 Probable CausebombardierwatchPas encore d'évaluation
- NTSB LJ 070823 Probable CauseDocument2 pagesNTSB LJ 070823 Probable CausebombardierwatchPas encore d'évaluation
- NTSB BAC 031202 Probable CauseDocument2 pagesNTSB BAC 031202 Probable CausebombardierwatchPas encore d'évaluation
- NTSB BAC 080113 Probable CauseDocument2 pagesNTSB BAC 080113 Probable CausebombardierwatchPas encore d'évaluation
- NTSB LJ 020830 Probable CauseDocument3 pagesNTSB LJ 020830 Probable CausebombardierwatchPas encore d'évaluation
- NTSB BAC 051026 Probable CauseDocument2 pagesNTSB BAC 051026 Probable CausebombardierwatchPas encore d'évaluation
- NTSB BAC 071216 Probable CauseDocument2 pagesNTSB BAC 071216 Probable CausebombardierwatchPas encore d'évaluation
- NTSB LJ 080221 Probable CauseDocument2 pagesNTSB LJ 080221 Probable CausebombardierwatchPas encore d'évaluation
- NTSB BAC 021024 Probable CauseDocument2 pagesNTSB BAC 021024 Probable CausebombardierwatchPas encore d'évaluation
- NTSB LJ 080919 Probable CauseDocument2 pagesNTSB LJ 080919 Probable CausebombardierwatchPas encore d'évaluation
- Metro LinerDocument318 pagesMetro Linergobo3000100% (1)
- NTSB BAC 001023 Probable CauseDocument2 pagesNTSB BAC 001023 Probable CausebombardierwatchPas encore d'évaluation
- NTSB BAC Final 990816 - Probable CauseDocument2 pagesNTSB BAC Final 990816 - Probable CausebombardierwatchPas encore d'évaluation
- NTSB BAC 041027 Probable CauseDocument2 pagesNTSB BAC 041027 Probable CausebombardierwatchPas encore d'évaluation
- NTSB LJ 030804 Probable CauseDocument3 pagesNTSB LJ 030804 Probable CausebombardierwatchPas encore d'évaluation
- NTSB BAC 080130 Probable CauseDocument2 pagesNTSB BAC 080130 Probable CausebombardierwatchPas encore d'évaluation
- NTSB BAC 061031 Probable CauseDocument2 pagesNTSB BAC 061031 Probable CausebombardierwatchPas encore d'évaluation
- NTSB LJ 980523 Probable CauseDocument2 pagesNTSB LJ 980523 Probable CausebombardierwatchPas encore d'évaluation
- NTSB BAC 020309 Probable CauseDocument2 pagesNTSB BAC 020309 Probable CausebombardierwatchPas encore d'évaluation
- NTSB LJ 050715 Probable CauseDocument2 pagesNTSB LJ 050715 Probable CausebombardierwatchPas encore d'évaluation
- NTSB BAC 050311 Probable CauseDocument3 pagesNTSB BAC 050311 Probable CausebombardierwatchPas encore d'évaluation
- NTSB BAC 040721 Probable CauseDocument2 pagesNTSB BAC 040721 Probable CausebombardierwatchPas encore d'évaluation
- NTSB LJ 010824 Probable CauseDocument2 pagesNTSB LJ 010824 Probable CausebombardierwatchPas encore d'évaluation
- NTSB BAC 061210 Probable CauseDocument2 pagesNTSB BAC 061210 Probable CausebombardierwatchPas encore d'évaluation
- NTSB BAC 070412 FactualDocument9 pagesNTSB BAC 070412 FactualbombardierwatchPas encore d'évaluation
- NTSB BAC 050521 Probable CauseDocument2 pagesNTSB BAC 050521 Probable CausebombardierwatchPas encore d'évaluation
- NTSB LJ 051026 FactualDocument1 pageNTSB LJ 051026 FactualbombardierwatchPas encore d'évaluation
- Preliminary Report of The Fatal Thomson Plane CrashDocument5 pagesPreliminary Report of The Fatal Thomson Plane CrashMatthew EnfingerPas encore d'évaluation
- Report - CEN20LA172 - 101247 - 7232022 83407 AMDocument7 pagesReport - CEN20LA172 - 101247 - 7232022 83407 AMFiron FironPas encore d'évaluation
- NTSB LJ 010607 Probable CauseDocument2 pagesNTSB LJ 010607 Probable CausebombardierwatchPas encore d'évaluation
- NTSB BAC 100119 FactualDocument10 pagesNTSB BAC 100119 FactualbombardierwatchPas encore d'évaluation
- NTSB BAC 980309 Probable CauseDocument2 pagesNTSB BAC 980309 Probable CausebombardierwatchPas encore d'évaluation
- NTSB BAC 070131 Probable CauseDocument2 pagesNTSB BAC 070131 Probable CausebombardierwatchPas encore d'évaluation
- National Transportation Safety Board Aviation Accident Data SummaryDocument3 pagesNational Transportation Safety Board Aviation Accident Data SummarytigriochelitoPas encore d'évaluation
- Runway Excursion Citation Mustang 31aug2019Document6 pagesRunway Excursion Citation Mustang 31aug2019Ramiro MuriasPas encore d'évaluation
- NTSB LJ 991025 Probable CauseDocument2 pagesNTSB LJ 991025 Probable CausebombardierwatchPas encore d'évaluation
- NTSB LJ 000312 FactualDocument6 pagesNTSB LJ 000312 FactualbombardierwatchPas encore d'évaluation
- NTSB LJ 000405 Probable CauseDocument2 pagesNTSB LJ 000405 Probable CausebombardierwatchPas encore d'évaluation
- NTSB BAC 050521 FactualDocument1 pageNTSB BAC 050521 FactualbombardierwatchPas encore d'évaluation
- Report - ERA20CA073 - 100793 - 6 - 14 - 2022 1 - 40 - 47 AMDocument5 pagesReport - ERA20CA073 - 100793 - 6 - 14 - 2022 1 - 40 - 47 AMaeroridhPas encore d'évaluation
- Report - CEN20CA350 - 101824 - 9102022 31100 AMDocument5 pagesReport - CEN20CA350 - 101824 - 9102022 31100 AMFiron FironPas encore d'évaluation
- Report - WPR20CA132 - 101212 - 7232022 83714 AMDocument5 pagesReport - WPR20CA132 - 101212 - 7232022 83714 AMKhan RihanPas encore d'évaluation
- IOTC AIR, LLC v. BOMBARDIER INC. Et Al DocketDocument1 pageIOTC AIR, LLC v. BOMBARDIER INC. Et Al DocketbombardierwatchPas encore d'évaluation
- Bombardier Recreational Products Inc. Recalls Snowmobiles Due To Crash and Fire HazardsDocument3 pagesBombardier Recreational Products Inc. Recalls Snowmobiles Due To Crash and Fire HazardsbombardierwatchPas encore d'évaluation
- CPSC, Bombardier Recreational Products Inc. Announce Recall of All-Terrain VehiclesDocument3 pagesCPSC, Bombardier Recreational Products Inc. Announce Recall of All-Terrain VehiclesbombardierwatchPas encore d'évaluation
- BRP Recalls Snowmobiles Due To Explosion HazardDocument4 pagesBRP Recalls Snowmobiles Due To Explosion HazardbombardierwatchPas encore d'évaluation
- CPSC, Bombardier Recreational Products Inc. Announce Recall of SnowmobilesDocument5 pagesCPSC, Bombardier Recreational Products Inc. Announce Recall of SnowmobilesbombardierwatchPas encore d'évaluation
- CPSC, Bombardier Recreational Products Inc., and Deere & Company Announce Recall of ATVsDocument5 pagesCPSC, Bombardier Recreational Products Inc., and Deere & Company Announce Recall of ATVsbombardierwatchPas encore d'évaluation
- CPSC, Bombardier Recreational Products Inc. Announce Recall of Ratchet Winch Kits, Sold As Accessory For SnowmobilesDocument2 pagesCPSC, Bombardier Recreational Products Inc. Announce Recall of Ratchet Winch Kits, Sold As Accessory For SnowmobilesbombardierwatchPas encore d'évaluation
- SPARTZ, KATHLEEN v. BRP US INC DocketDocument1 pageSPARTZ, KATHLEEN v. BRP US INC DocketbombardierwatchPas encore d'évaluation
- STEWART, ANASTASIA THERESA Et Al v. SUNJET AVIATDKN INC, Et Al DocketDocument60 pagesSTEWART, ANASTASIA THERESA Et Al v. SUNJET AVIATDKN INC, Et Al DocketbombardierwatchPas encore d'évaluation
- BULMAN v. BOMBARDIER, INC., Et Al 2nd DocketDocument6 pagesBULMAN v. BOMBARDIER, INC., Et Al 2nd DocketbombardierwatchPas encore d'évaluation
- PESANTE v. BOMBARDIER TRANSPORTATION ComplaintDocument13 pagesPESANTE v. BOMBARDIER TRANSPORTATION ComplaintbombardierwatchPas encore d'évaluation
- FRALEY, DIXIE LEIGH Et Al vs. SUNJET AVIATION INC, Et Al DocketDocument47 pagesFRALEY, DIXIE LEIGH Et Al vs. SUNJET AVIATION INC, Et Al DocketbombardierwatchPas encore d'évaluation
- SWINGLE v. EPPS AIR SERVICE, Et Al Bombardier ResponseDocument11 pagesSWINGLE v. EPPS AIR SERVICE, Et Al Bombardier ResponsebombardierwatchPas encore d'évaluation
- SWINGLE v. EPPS AIR SERVICE, Et Al DocketDocument2 pagesSWINGLE v. EPPS AIR SERVICE, Et Al DocketbombardierwatchPas encore d'évaluation
- Incoterms 2000Document25 pagesIncoterms 2000Praygod ManasePas encore d'évaluation
- Permco 2100 Series Engineering Model Designation & Part Number Code BookDocument27 pagesPermco 2100 Series Engineering Model Designation & Part Number Code BookMistysPartsPas encore d'évaluation
- Commercial Invoice/Packing ListDocument2 pagesCommercial Invoice/Packing ListVu Duc QuangPas encore d'évaluation
- Concrete Construction EquipmentDocument25 pagesConcrete Construction EquipmentAYUSH PARAJULIPas encore d'évaluation
- Garuda Boarding PassDocument1 pageGaruda Boarding PassRaditya JuliantoroPas encore d'évaluation
- Manual Ansul LvsDocument74 pagesManual Ansul LvsMichael IturraPas encore d'évaluation
- 1108 TicketDocument2 pages1108 TicketAnonymous TPVfFif6TOPas encore d'évaluation
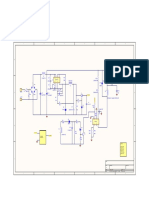
- Schematic For LED Driver IC BP2851Document1 pageSchematic For LED Driver IC BP2851ztxPas encore d'évaluation
- Intermech Bbrfbrvip CNG Compressors 55 450 KW 75 600 HP Tcm1143-3540245Document13 pagesIntermech Bbrfbrvip CNG Compressors 55 450 KW 75 600 HP Tcm1143-3540245Chakravarthy BharathPas encore d'évaluation
- Report On Tactical UrbanismDocument21 pagesReport On Tactical UrbanismIan Ricardo AlbaPas encore d'évaluation
- Worksheet 1 in EAPPDocument2 pagesWorksheet 1 in EAPPStephanie AlcorizaPas encore d'évaluation
- Cooling System Report (Automotive Tech.)Document5 pagesCooling System Report (Automotive Tech.)Mohamed AhmedPas encore d'évaluation
- Pedido LFDocument81 pagesPedido LFgonzalo rodriguezPas encore d'évaluation
- (General) (Time Allowed - 3 Hours) Total Marks 100 India Morning Paper N.B. - (1) Attempt SIX Questions ONLYDocument2 pages(General) (Time Allowed - 3 Hours) Total Marks 100 India Morning Paper N.B. - (1) Attempt SIX Questions ONLYThiet PhamPas encore d'évaluation
- Ergo Guide ABSDocument74 pagesErgo Guide ABScvhar87Pas encore d'évaluation
- Clement Asuliwonno 2011Document90 pagesClement Asuliwonno 2011Edmund PaulPas encore d'évaluation
- Aerodrome PPT 4.2Document109 pagesAerodrome PPT 4.2John Client Aclan RanisPas encore d'évaluation
- Medollar Math7 PDFDocument2 pagesMedollar Math7 PDFBetchang AquinoPas encore d'évaluation
- DNV-OS-C301 (Stability & Watertight Integrity)Document27 pagesDNV-OS-C301 (Stability & Watertight Integrity)tidus00_3Pas encore d'évaluation
- Warehouse LogisticsDocument12 pagesWarehouse LogisticsarzusafranPas encore d'évaluation
- Bridgestone-Manual 2018 PDFDocument119 pagesBridgestone-Manual 2018 PDFEmily Simpson100% (1)
- Seamanship (Rigging) : BendsDocument85 pagesSeamanship (Rigging) : BendsMohan KhavnekarPas encore d'évaluation
- Transport Hotel BandaraDocument2 pagesTransport Hotel Bandaraandika juliyantoPas encore d'évaluation
- Chassis Engineering CatalogDocument48 pagesChassis Engineering Catalogjoelsanchezcamacho100% (1)
- Soạn Đề Ilearn 7 Giữa KìDocument6 pagesSoạn Đề Ilearn 7 Giữa Kìgiasutaihue1Pas encore d'évaluation
- Mercruiser Technical DataDocument45 pagesMercruiser Technical Datajose antonio MelladoPas encore d'évaluation
- Drum Handling EquDocument20 pagesDrum Handling EquMohd HattaPas encore d'évaluation
- SIR System o Bolsas de AireDocument17 pagesSIR System o Bolsas de AireJesus Maria LizarzabalPas encore d'évaluation
- Sustainablilty Report 15 16Document110 pagesSustainablilty Report 15 16wuguohaoPas encore d'évaluation
- The Art of Fear: Why Conquering Fear Won't Work and What to Do InsteadD'EverandThe Art of Fear: Why Conquering Fear Won't Work and What to Do InsteadÉvaluation : 4 sur 5 étoiles4/5 (10)
- Higher Love: Climbing and Skiing the Seven SummitsD'EverandHigher Love: Climbing and Skiing the Seven SummitsÉvaluation : 5 sur 5 étoiles5/5 (6)
- The Darkest White: A Mountain Legend and the Avalanche That Took HimD'EverandThe Darkest White: A Mountain Legend and the Avalanche That Took HimÉvaluation : 4 sur 5 étoiles4/5 (1)
- Strong Is the New Beautiful: Embrace Your Natural Beauty, Eat Clean, and Harness Your PowerD'EverandStrong Is the New Beautiful: Embrace Your Natural Beauty, Eat Clean, and Harness Your PowerÉvaluation : 4 sur 5 étoiles4/5 (5)
- Training for the Uphill Athlete: A Manual for Mountain Runners and Ski MountaineersD'EverandTraining for the Uphill Athlete: A Manual for Mountain Runners and Ski MountaineersÉvaluation : 5 sur 5 étoiles5/5 (13)
- Strong is the New Beautiful: Embrace Your Natural Beauty, Eat Clean, and Harness Your PowerD'EverandStrong is the New Beautiful: Embrace Your Natural Beauty, Eat Clean, and Harness Your PowerÉvaluation : 4 sur 5 étoiles4/5 (22)
- Climb to Conquer: The Untold Story of WWII's 10th Mountain Division Ski TroopsD'EverandClimb to Conquer: The Untold Story of WWII's 10th Mountain Division Ski TroopsÉvaluation : 5 sur 5 étoiles5/5 (1)
- Marián Hossa: My Journey from Trencín to the Hall of FameD'EverandMarián Hossa: My Journey from Trencín to the Hall of FamePas encore d'évaluation
- Winterdance: The Fine Madness of Running the IditarodD'EverandWinterdance: The Fine Madness of Running the IditarodÉvaluation : 4.5 sur 5 étoiles4.5/5 (279)
- Training for the Uphill Athlete: A Manual for Mountain Runners and Ski MountaineersD'EverandTraining for the Uphill Athlete: A Manual for Mountain Runners and Ski MountaineersÉvaluation : 4.5 sur 5 étoiles4.5/5 (8)
- Everything the Instructors Never Told You About Mogul SkiingD'EverandEverything the Instructors Never Told You About Mogul SkiingÉvaluation : 3 sur 5 étoiles3/5 (1)
- The Art of Fear: Why Conquering Fear Won't Work and What to Do InsteadD'EverandThe Art of Fear: Why Conquering Fear Won't Work and What to Do InsteadÉvaluation : 3.5 sur 5 étoiles3.5/5 (6)
- Hockey: Hockey Made Easy: Beginner and Expert Strategies For Becoming A Better Hockey PlayerD'EverandHockey: Hockey Made Easy: Beginner and Expert Strategies For Becoming A Better Hockey PlayerPas encore d'évaluation
- Skiing into the Bright Open: My Solo Journey to the South PoleD'EverandSkiing into the Bright Open: My Solo Journey to the South PolePas encore d'évaluation
- Two Planks and a Passion: The Dramatic History of SkiingD'EverandTwo Planks and a Passion: The Dramatic History of SkiingPas encore d'évaluation
- Frostbike: The Joy, Pain and Numbness of Winter CyclingD'EverandFrostbike: The Joy, Pain and Numbness of Winter CyclingÉvaluation : 4 sur 5 étoiles4/5 (3)
- Unbound: A Story of Snow and Self-DiscoveryD'EverandUnbound: A Story of Snow and Self-DiscoveryÉvaluation : 3.5 sur 5 étoiles3.5/5 (7)
- Mistake-Free Golf: First Aid for Your Golfing BrainD'EverandMistake-Free Golf: First Aid for Your Golfing BrainÉvaluation : 4 sur 5 étoiles4/5 (1)
- Backcountry Avalanche Safety: A Guide to Managing Avalanche Risk - 4th EditionD'EverandBackcountry Avalanche Safety: A Guide to Managing Avalanche Risk - 4th EditionPas encore d'évaluation