Vous aimerez peut-être aussi
- Application 2011 2012Document12 pagesApplication 2011 2012dbreynaePas encore d'évaluation
- Deben High School 2009-10 ProspectusDocument16 pagesDeben High School 2009-10 Prospectusold_debenhighPas encore d'évaluation
- Resume MasterDocument3 pagesResume Masterapi-340262567Pas encore d'évaluation
- Handbook: 2499 Main Street Klamath Falls, OR 97601 541-882-4151 Welcome!Document14 pagesHandbook: 2499 Main Street Klamath Falls, OR 97601 541-882-4151 Welcome!api-326416336Pas encore d'évaluation
- First Grade Syllabus 2016Document4 pagesFirst Grade Syllabus 2016api-463065693Pas encore d'évaluation
- 3rd Grade PPT 2019-2020 6Document39 pages3rd Grade PPT 2019-2020 6api-467171764Pas encore d'évaluation
- Lexi Cyphers Resume 2016Document1 pageLexi Cyphers Resume 2016api-285382578Pas encore d'évaluation
- Nicole Whelan Resume-GcuDocument2 pagesNicole Whelan Resume-Gcuapi-434580279Pas encore d'évaluation
- MM - 23 Sept 2011 pdf1Document6 pagesMM - 23 Sept 2011 pdf1api-22065138Pas encore d'évaluation
- LeConte Newsletter Oct 2011Document7 pagesLeConte Newsletter Oct 2011pazchannelsPas encore d'évaluation
- Madison Slater ResumeDocument4 pagesMadison Slater Resumeapi-447690352Pas encore d'évaluation
- Duff-Newsome SchoolDocument25 pagesDuff-Newsome Schoolapi-251807548Pas encore d'évaluation
- Principal's Message: The Eagle FlyerDocument3 pagesPrincipal's Message: The Eagle Flyerapi-262365902Pas encore d'évaluation
- Hhs Continue To SoarDocument17 pagesHhs Continue To SoartochumaruPas encore d'évaluation
- Jan 25 ThnewsletterDocument4 pagesJan 25 Thnewsletterapi-108443703Pas encore d'évaluation
- Report To The Community - GoodDocument1 pageReport To The Community - GoodCFBISDPas encore d'évaluation
- School Information Booklet 2008-2009Document19 pagesSchool Information Booklet 2008-2009brogPas encore d'évaluation
- Elementary Disclosure Document Sharley Bradley ELP First Grade 2019-2020 Hawthorne Elementary, Room 6Document6 pagesElementary Disclosure Document Sharley Bradley ELP First Grade 2019-2020 Hawthorne Elementary, Room 6api-234404321Pas encore d'évaluation
- Welcome To Mrs. Kirk's Fifth Grade Class!: Teaching PhilosophyDocument5 pagesWelcome To Mrs. Kirk's Fifth Grade Class!: Teaching Philosophyapi-287198374Pas encore d'évaluation
- E Goshen 12Document2 pagesE Goshen 12api-238851254Pas encore d'évaluation
- Luta Resume 2018Document2 pagesLuta Resume 2018api-254493596Pas encore d'évaluation
- Resume 1Document3 pagesResume 1api-392152664Pas encore d'évaluation
- Neiliezhu Memorial SchoolDocument6 pagesNeiliezhu Memorial SchooltetenoPas encore d'évaluation
- REC Newsletter February 2016Document12 pagesREC Newsletter February 2016Reynella East CollegePas encore d'évaluation
- pkppcd2017 PPT 2 1Document47 pagespkppcd2017 PPT 2 1api-267626110Pas encore d'évaluation
- EHMS HandbookDocument7 pagesEHMS HandbookjoezanottoPas encore d'évaluation
- Resume 04012019Document2 pagesResume 04012019api-456586610Pas encore d'évaluation
- Ithaca South Elementary: Principal's Greeting/MessageDocument6 pagesIthaca South Elementary: Principal's Greeting/Messageapi-7665481Pas encore d'évaluation
- PPP Handbook 2019-2020Document14 pagesPPP Handbook 2019-2020api-277939196Pas encore d'évaluation
- Mmdec 15Document3 pagesMmdec 15api-290923568Pas encore d'évaluation
- Payton Burrows ResumeDocument2 pagesPayton Burrows ResumePayton BurrowsPas encore d'évaluation
- Ms. Thompson's Second Grade: Welcome Parents!Document30 pagesMs. Thompson's Second Grade: Welcome Parents!rthmpsn6Pas encore d'évaluation
- School Profile For InternsDocument1 pageSchool Profile For InternsSheila BanuelosPas encore d'évaluation
- Resume 2022Document2 pagesResume 2022api-310907782Pas encore d'évaluation
- Halam: Prospectus 2014/ 2015Document22 pagesHalam: Prospectus 2014/ 2015nauman123Pas encore d'évaluation
- Catherine ConnellyteachresumeDocument3 pagesCatherine Connellyteachresumeapi-270342111Pas encore d'évaluation
- Teaching Resume 2013editedDocument3 pagesTeaching Resume 2013editedapi-242131540Pas encore d'évaluation
- School Based Budget Project-LockardDocument19 pagesSchool Based Budget Project-Lockardapi-367519610Pas encore d'évaluation
- Thursday Thoughts: Freaky Friday DiscoDocument6 pagesThursday Thoughts: Freaky Friday DiscoLaunchpsPas encore d'évaluation
- Huygens Ashley Resume 5Document2 pagesHuygens Ashley Resume 5api-254334803Pas encore d'évaluation
- Principal'S Report: Important DatesDocument5 pagesPrincipal'S Report: Important DatesernsteinsPas encore d'évaluation
- Roberts ResumeDocument2 pagesRoberts Resumeapi-236436423Pas encore d'évaluation
- WCE Newsletter May 2011Document9 pagesWCE Newsletter May 2011Lori CowanPas encore d'évaluation
- SrSec AlamanacDocument62 pagesSrSec AlamanacPranshu Singh AhlawatPas encore d'évaluation
- Home-School AgreementDocument2 pagesHome-School Agreementisleworthsyon100% (1)
- Resume Teacher WebsiteDocument2 pagesResume Teacher Websiteapi-300485143Pas encore d'évaluation
- Atoka Elementary School's 5 Grade Classroom Rules, Policies, & Procedures 2016-2017Document5 pagesAtoka Elementary School's 5 Grade Classroom Rules, Policies, & Procedures 2016-2017api-351301719Pas encore d'évaluation
- Teaching Work Sample 1Document80 pagesTeaching Work Sample 1api-295202117Pas encore d'évaluation
- Principally Speaking - Mrs. Megan Ashworth: Parent CommunicationDocument8 pagesPrincipally Speaking - Mrs. Megan Ashworth: Parent CommunicationmorabeccaPas encore d'évaluation
- Resume KelliodellDocument4 pagesResume Kelliodellapi-270420075Pas encore d'évaluation
- Rolling Hills Catholic School HomeworkDocument8 pagesRolling Hills Catholic School Homeworkfemaf0nanen3100% (1)
- PaulstephanietarkingtonDocument4 pagesPaulstephanietarkingtonapi-287623259Pas encore d'évaluation
- Sept 2016 Parent BulletinDocument8 pagesSept 2016 Parent Bulletinapi-253599405Pas encore d'évaluation
- Child Friendly School Feedback FormDocument9 pagesChild Friendly School Feedback FormWALOPas encore d'évaluation
- Resurrection School Handbook 2018-2019Document43 pagesResurrection School Handbook 2018-2019Joe KeithPas encore d'évaluation
- CV Example 2014Document3 pagesCV Example 2014Anonymous qYLCNiaCPas encore d'évaluation
- Curriculum Night Second GradeDocument27 pagesCurriculum Night Second Gradeapi-328550972Pas encore d'évaluation
- Lunch Menu AprilDocument1 pageLunch Menu AprildbreynaePas encore d'évaluation
- Color Codes July 2012 August 2012 September 2012 October 2012Document5 pagesColor Codes July 2012 August 2012 September 2012 October 2012dbreynaePas encore d'évaluation
- June Lunch 2012Document1 pageJune Lunch 2012dbreynaePas encore d'évaluation
- May Lunch MenuDocument1 pageMay Lunch MenudbreynaePas encore d'évaluation
- Lunch Menu March 2012Document1 pageLunch Menu March 2012dbreynaePas encore d'évaluation
- Hope Staff 2011-12Document1 pageHope Staff 2011-12dbreynaePas encore d'évaluation
- Hope Staff 2011-12Document1 pageHope Staff 2011-12dbreynaePas encore d'évaluation
- Lunch Menu Feb 2012Document1 pageLunch Menu Feb 2012dbreynaePas encore d'évaluation
- September Lunch MenuDocument1 pageSeptember Lunch MenudbreynaePas encore d'évaluation
- Hope August Lunch MenuDocument1 pageHope August Lunch MenudbreynaePas encore d'évaluation
- Nov. Lunch MenuDocument1 pageNov. Lunch MenudbreynaePas encore d'évaluation
- Lunch Menu MarchDocument1 pageLunch Menu MarchdbreynaePas encore d'évaluation
- Lunch Menu FebDocument1 pageLunch Menu FebdbreynaePas encore d'évaluation
- Lunch Menu Jan 2012Document1 pageLunch Menu Jan 2012dbreynaePas encore d'évaluation
- Lunch Menu JuneDocument1 pageLunch Menu JunedbreynaePas encore d'évaluation
- May Lunch MenuDocument1 pageMay Lunch MenudbreynaePas encore d'évaluation
- September Lunch MenuDocument1 pageSeptember Lunch MenudbreynaePas encore d'évaluation
- School Calendar 2009-2010 2010-2011Document2 pagesSchool Calendar 2009-2010 2010-2011dbreynaePas encore d'évaluation
- Application 2010 2011Document9 pagesApplication 2010 2011dbreynaePas encore d'évaluation
- Lunch MenuDocument1 pageLunch MenudbreynaePas encore d'évaluation
- February Lunch MenuDocument1 pageFebruary Lunch MenudbreynaePas encore d'évaluation
- October Lunch MenuDocument1 pageOctober Lunch MenudbreynaePas encore d'évaluation
- Philosophy of Education Solved MCQ's With PDF Download (Set-2)Document10 pagesPhilosophy of Education Solved MCQ's With PDF Download (Set-2)Nilam ThatoiPas encore d'évaluation
- Full Download Book Inclusion in Action PDFDocument41 pagesFull Download Book Inclusion in Action PDFtommy.peacock526100% (17)
- Lesson Plan English ExampleDocument3 pagesLesson Plan English ExampleperakashPas encore d'évaluation
- Functional VocabularyDocument179 pagesFunctional VocabularyEmily Thomas50% (2)
- Curriculum Vitae (CV) : 1. Name: 2. Date of Birth: 3. EducationDocument4 pagesCurriculum Vitae (CV) : 1. Name: 2. Date of Birth: 3. EducationSanjaya Bikram ShahPas encore d'évaluation
- Activity Sheet InHS9Document14 pagesActivity Sheet InHS9Jerodette Ann Ocop OcenaPas encore d'évaluation
- Tugas Final Bahasa Inggris - Anisa SusiantiDocument2 pagesTugas Final Bahasa Inggris - Anisa SusiantiAnisa SusiantiPas encore d'évaluation
- Chapter 1 - Module 3Document9 pagesChapter 1 - Module 3Kendall NievaPas encore d'évaluation
- CARB Complaint - Fiona McGuinness Letter Use of Client InformationDocument1 pageCARB Complaint - Fiona McGuinness Letter Use of Client InformationIntegrityPas encore d'évaluation
- Math IaDocument10 pagesMath Iaapi-448713420Pas encore d'évaluation
- Instructional Planning - Educational PsychologyDocument14 pagesInstructional Planning - Educational PsychologyDesales BuerPas encore d'évaluation
- Action Plan in EnglishDocument2 pagesAction Plan in EnglishJon Vader83% (6)
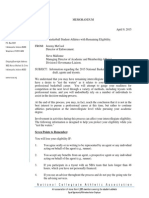
- Ncaa MemorandumDocument6 pagesNcaa MemorandumrabineitorPas encore d'évaluation
- Fillable-AAF 014Document2 pagesFillable-AAF 014JEULO D. MADRIAGAPas encore d'évaluation
- DACUM ProcessDocument72 pagesDACUM Processjvarga.db4878Pas encore d'évaluation
- Agile Processes in Software Engineering and Extreme ProgrammingDocument311 pagesAgile Processes in Software Engineering and Extreme Programmingalfonso lopez alquisirez100% (1)
- Students Self AssessmentDocument5 pagesStudents Self AssessmentAnusha PSPas encore d'évaluation
- Individual Worksheet Accomplishment (Week 4)Document2 pagesIndividual Worksheet Accomplishment (Week 4)Patrick EdrosoloPas encore d'évaluation
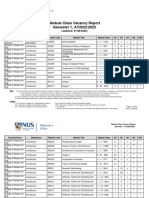
- VacancyRpt R3 2223S1Document273 pagesVacancyRpt R3 2223S1Lim ShawnPas encore d'évaluation
- Curtis Dowlearn Scholarship Fund Donor LetterDocument2 pagesCurtis Dowlearn Scholarship Fund Donor LetterScott Villarreal-DowlearnPas encore d'évaluation
- Learning Plan: Lesson No: 2 Lesson Title: Gender and Socialization Let's Hit TheseDocument8 pagesLearning Plan: Lesson No: 2 Lesson Title: Gender and Socialization Let's Hit TheseAllan IgbuhayPas encore d'évaluation
- 01CASE 1 PBW Thats The WayDocument11 pages01CASE 1 PBW Thats The WayHitesh DhingraPas encore d'évaluation
- District Enhancement Training of School Heads On Instructional Leadership in The New NormalDocument7 pagesDistrict Enhancement Training of School Heads On Instructional Leadership in The New NormalLINDO LECERAPas encore d'évaluation
- Autobiography EssayDocument7 pagesAutobiography Essayapi-533899699Pas encore d'évaluation
- Lesson Plan English 10Document6 pagesLesson Plan English 10Butch RejusoPas encore d'évaluation
- Activity Guide and Evaluation Rubric - Unit 1 - Phase 2 - Skills For TeachersDocument8 pagesActivity Guide and Evaluation Rubric - Unit 1 - Phase 2 - Skills For TeachersHeder MartinezPas encore d'évaluation
- Melc DLL Eng 8 Week 4 Q4 DoneDocument8 pagesMelc DLL Eng 8 Week 4 Q4 DoneNoella Janeel BrotonelPas encore d'évaluation
- Volleyball Lesson Plan 4-29-15Document7 pagesVolleyball Lesson Plan 4-29-15api-267398125Pas encore d'évaluation
- Rachel Dow March 2019Document1 pageRachel Dow March 2019api-414910309Pas encore d'évaluation
- FPA-13 Exam Prep Guide BetaDocument6 pagesFPA-13 Exam Prep Guide Betaradqudah0% (1)