Vous aimerez peut-être aussi
- Patient Assestment PDFDocument12 pagesPatient Assestment PDFAnonymous 85pLrRPas encore d'évaluation
- Fall Risk Assessment FormDocument3 pagesFall Risk Assessment FormMichael Silva100% (1)
- AbbreviationDocument19 pagesAbbreviationJayson NatividadPas encore d'évaluation
- Screening Head To Toe Physical ExaminationDocument16 pagesScreening Head To Toe Physical ExaminationJay Mar Mendoza BabatePas encore d'évaluation
- HO - Burns Environmental EmergenciesDocument7 pagesHO - Burns Environmental EmergenciesSteven Paul DaclesPas encore d'évaluation
- Grady EMS Drug List 2017 FINALDocument20 pagesGrady EMS Drug List 2017 FINALThomas LeachPas encore d'évaluation
- Suggested Order For History and Physical Examination DocumentationDocument2 pagesSuggested Order For History and Physical Examination DocumentationNicole BrassingtonPas encore d'évaluation
- Neurological AssessmentDocument7 pagesNeurological AssessmentErika NicaPas encore d'évaluation
- May 1-7 Assessment of Neurologic FunctionDocument59 pagesMay 1-7 Assessment of Neurologic FunctionSherlyn PedidaPas encore d'évaluation
- Physical AssessmentDocument29 pagesPhysical AssessmentTheSweetpea501100% (1)
- Emergency Trauma CareDocument49 pagesEmergency Trauma Careandrei neagPas encore d'évaluation
- Health HistoryDocument19 pagesHealth HistoryAngelene Caliva100% (1)
- Preoperative Assessment in Diabetic PatientsDocument2 pagesPreoperative Assessment in Diabetic PatientsShilpa Pradhan100% (1)
- Nursing Care PlanDocument6 pagesNursing Care PlanChesca MejiaPas encore d'évaluation
- Tinitti Balance Assessment ToolDocument2 pagesTinitti Balance Assessment Toolcpradheep100% (2)
- Head To Toe AssesmentDocument4 pagesHead To Toe AssesmentYemaya84100% (1)
- Burns CH 25 n-7Document7 pagesBurns CH 25 n-7Jessica VargasPas encore d'évaluation
- BLS SummaryDocument2 pagesBLS Summaryreyes markPas encore d'évaluation
- History Taking Physical ExamininationDocument41 pagesHistory Taking Physical ExamininationAya AmerPas encore d'évaluation
- Cardio-Pulmonary Resuscitation (CPR)Document18 pagesCardio-Pulmonary Resuscitation (CPR)Savita HanamsagarPas encore d'évaluation
- Documentation Guideline: Wound Assessment &treatment Flow Sheet (WATFS) Portrait Version With PSLS#Document6 pagesDocumentation Guideline: Wound Assessment &treatment Flow Sheet (WATFS) Portrait Version With PSLS#eva arna abrarPas encore d'évaluation
- Nursing Education Department: Patient AssessmentDocument34 pagesNursing Education Department: Patient AssessmentSitti Mardiya SariolPas encore d'évaluation
- Nursing Dummy ChartDocument4 pagesNursing Dummy Chartis_aradanasPas encore d'évaluation
- 1008 1400 ACLS - StudyGuide Print PDFDocument54 pages1008 1400 ACLS - StudyGuide Print PDFWaqar HassanPas encore d'évaluation
- Juvenile Rheumatoid Arthritis: Dorothy W. Wortmann, MDDocument38 pagesJuvenile Rheumatoid Arthritis: Dorothy W. Wortmann, MDLavi GoyalPas encore d'évaluation
- NEIL Trauma AssessmentDocument3 pagesNEIL Trauma AssessmentNeil BrunoPas encore d'évaluation
- Emt Patient AssessDocument54 pagesEmt Patient AssessMdp NoorkasihPas encore d'évaluation
- West Visayas State University: Nursing ProcessDocument4 pagesWest Visayas State University: Nursing ProcessPhylum Chordata100% (1)
- Acls LectureDocument15 pagesAcls LectureVincent BautistaPas encore d'évaluation
- Activity 1 Assessment of Patients With Cardiovascular Disorders PDFDocument1 pageActivity 1 Assessment of Patients With Cardiovascular Disorders PDFJarda DacuagPas encore d'évaluation
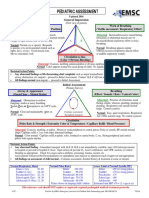
- Pediatric Assessment: General ImpressionDocument2 pagesPediatric Assessment: General ImpressionAghnia Nafila100% (1)
- 04 - Soft Tissue InjuriesDocument13 pages04 - Soft Tissue InjuriesCielo GriñoPas encore d'évaluation
- TraumaBurn ClinicalGuidelines Final PDFDocument34 pagesTraumaBurn ClinicalGuidelines Final PDFJuan Antonio GarcíaPas encore d'évaluation
- Assessment of The Peripheral Vascular SystemDocument11 pagesAssessment of The Peripheral Vascular SystempatziePas encore d'évaluation
- Physical Examination Form: Medications AllergiesDocument4 pagesPhysical Examination Form: Medications AllergiesIris Ann PhillipsPas encore d'évaluation
- Concussion PPT June 20101Document36 pagesConcussion PPT June 20101CiiFitriPas encore d'évaluation
- Simple Triage and Rapid TreatmentDocument9 pagesSimple Triage and Rapid TreatmentGung IndrayanaPas encore d'évaluation
- Hip FractureDocument3 pagesHip Fracturenursing concept mapsPas encore d'évaluation
- Physical Assessment Write-UpDocument10 pagesPhysical Assessment Write-UpkathypinzonPas encore d'évaluation
- Head Injury: Manali H. Solanki F.Y. M.Sc. Nursing J G College of NursingDocument31 pagesHead Injury: Manali H. Solanki F.Y. M.Sc. Nursing J G College of NursingWaqar AhmedPas encore d'évaluation
- NursingCare PlanDocument8 pagesNursingCare PlanSunSearra Kennedy RuffinPas encore d'évaluation
- Nurs 641 Case Study PresentationDocument12 pagesNurs 641 Case Study Presentationapi-251235373Pas encore d'évaluation
- Harris Regional ICU Daily Sedation Vacation GuidelinesDocument1 pageHarris Regional ICU Daily Sedation Vacation GuidelinesFebri Yudha Adhi KurniawanPas encore d'évaluation
- Profession Practice AssignmentDocument10 pagesProfession Practice AssignmentAssiduous Facetious100% (1)
- Vitals Pocket ChartDocument4 pagesVitals Pocket ChartAli MullaPas encore d'évaluation
- Anaphylactic ShockDocument39 pagesAnaphylactic Shockerwindorinaldo100% (1)
- Post-ACLS Megacode Flashcards - QuizletDocument9 pagesPost-ACLS Megacode Flashcards - QuizletMaya LaPradePas encore d'évaluation
- PBL PgamboaDocument6 pagesPBL PgamboaLeanne Princess GamboaPas encore d'évaluation
- Physical ExaminationDocument117 pagesPhysical Examinationsasmita nayakPas encore d'évaluation
- Neurological Assessment: Alice E. Davis, PH.D., RNDocument6 pagesNeurological Assessment: Alice E. Davis, PH.D., RNdhekuh100% (2)
- AirwayDocument25 pagesAirwayKURIMAONGPas encore d'évaluation
- General Appearance: Ital SignDocument4 pagesGeneral Appearance: Ital SignLiza Estrabo100% (1)
- Bls ProviderDocument2 pagesBls ProvidermonickamsPas encore d'évaluation
- A Simple Guide to Hypovolemia, Diagnosis, Treatment and Related ConditionsD'EverandA Simple Guide to Hypovolemia, Diagnosis, Treatment and Related ConditionsPas encore d'évaluation
- COMPREHENSIVE NURSING ACHIEVEMENT TEST (RN): Passbooks Study GuideD'EverandCOMPREHENSIVE NURSING ACHIEVEMENT TEST (RN): Passbooks Study GuidePas encore d'évaluation
- Management of Tuberculosis: A guide for clinicians (eBook edition)D'EverandManagement of Tuberculosis: A guide for clinicians (eBook edition)Pas encore d'évaluation
- A Simple Guide to Abdominal Aortic Aneurysm, Diagnosis, Treatment and Related ConditionsD'EverandA Simple Guide to Abdominal Aortic Aneurysm, Diagnosis, Treatment and Related ConditionsPas encore d'évaluation