Vous aimerez peut-être aussi
- Kids’ Puzzle Book, Grades 1 - 5: Volume 22D'EverandKids’ Puzzle Book, Grades 1 - 5: Volume 22Évaluation : 3.5 sur 5 étoiles3.5/5 (2)
- Mollie - Schmidt LorDocument1 pageMollie - Schmidt Lorapi-480337333Pas encore d'évaluation
- DIGM3351 VelasquezJackie Yearbook Final-1Document7 pagesDIGM3351 VelasquezJackie Yearbook Final-1Jackeline VelasquezPas encore d'évaluation
- Sale Catalog - Memorial Day Spectacular SaleDocument104 pagesSale Catalog - Memorial Day Spectacular SaleHolstein PlazaPas encore d'évaluation
- Greene County Zoning Inspectors Contact ListDocument1 pageGreene County Zoning Inspectors Contact ListThomas Scott JonesPas encore d'évaluation
- Youth Group DirectoryDocument4 pagesYouth Group DirectoryJon KwonPas encore d'évaluation
- Counseling BreakdownDocument1 pageCounseling Breakdownapi-520034936Pas encore d'évaluation
- ScheduleDocument2 pagesSchedulecraigtuckey123Pas encore d'évaluation
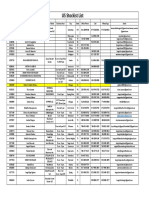
- 150 Vending LeadsDocument8 pages150 Vending Leadscalllucy066Pas encore d'évaluation
- BC Resource Van Visit Flyer NovemberDocument1 pageBC Resource Van Visit Flyer NovemberfamilycentralPas encore d'évaluation
- CERT MEMS CADRE AND CADET LEADERS ROSTERDocument1 pageCERT MEMS CADRE AND CADET LEADERS ROSTERMarkey LemonsPas encore d'évaluation
- HRWF November 2010 Redwood AlertDocument8 pagesHRWF November 2010 Redwood AlertHUMBOLDT REPUBLICAN WOMEN FEDERATEDPas encore d'évaluation
- ReferencesDocument1 pageReferencesapi-288983001Pas encore d'évaluation
- USA Stockist ListDocument1 pageUSA Stockist ListHalima HassanouPas encore d'évaluation
- Malla de AlambreDocument1 pageMalla de AlambreodrarekPas encore d'évaluation
- Escape22: Fall 2009 Escape Leaders/Small GroupsDocument1 pageEscape22: Fall 2009 Escape Leaders/Small Groupsapi-26122632Pas encore d'évaluation
- R6pec 20 - 21Document1 pageR6pec 20 - 21Dwayne JohnsonPas encore d'évaluation
- Resume OgDocument2 pagesResume Ogapi-453152760Pas encore d'évaluation
- March 2011 T BoardDocument2 pagesMarch 2011 T BoardTachaeonPas encore d'évaluation
- Back of Photo AlbumDocument1 pageBack of Photo AlbumBeckyOgannPas encore d'évaluation
- BC Van Schedule June 2010Document1 pageBC Van Schedule June 2010familycentralPas encore d'évaluation
- Part-Time Tutors Contact List for Broward County Virtual and In-Person LocationsDocument10 pagesPart-Time Tutors Contact List for Broward County Virtual and In-Person LocationsGabriel AlvesPas encore d'évaluation
- Escape22: We Are Not A Ministry With Small Groups, We Are A Ministry of Small Groups!Document1 pageEscape22: We Are Not A Ministry With Small Groups, We Are A Ministry of Small Groups!api-26122632Pas encore d'évaluation
- My NetworkDocument1 pageMy Networkapi-352678479Pas encore d'évaluation
- Time Sheet and ContactDocument2 pagesTime Sheet and Contactdbeebe0Pas encore d'évaluation
- April 2024 Community Food Calendar-B W Small FontDocument1 pageApril 2024 Community Food Calendar-B W Small Fontapi-316958482Pas encore d'évaluation
- District and Community Contact InformationDocument3 pagesDistrict and Community Contact Informationapi-543728028Pas encore d'évaluation
- 1112 CalendarDocument2 pages1112 Calendarmmiller7571Pas encore d'évaluation
- 2023-24 Ahs Ptsa Board - 2023-2024 Board and CommitteesDocument1 page2023-24 Ahs Ptsa Board - 2023-2024 Board and Committeesapi-356690518Pas encore d'évaluation
- Norterra Newsletter June 13-5Document2 pagesNorterra Newsletter June 13-5bpickering1Pas encore d'évaluation
- Sunday Worship Celebrations Sugar Grove Church: SGC Ministry Team Senior Open HousesDocument2 pagesSunday Worship Celebrations Sugar Grove Church: SGC Ministry Team Senior Open HousessugargrovechurchPas encore d'évaluation
- Braintree School 2017-18 CalendarDocument1 pageBraintree School 2017-18 CalendarDanLibonPas encore d'évaluation
- Social Studies InstructorsDocument3 pagesSocial Studies Instructorsapi-3708150Pas encore d'évaluation
- Delwood February 2017 FinalDocument12 pagesDelwood February 2017 Finalapi-247918245Pas encore d'évaluation
- Moecomdws District Cub Scout Pack ContactsDocument1 pageMoecomdws District Cub Scout Pack ContactsmoecomdwsPas encore d'évaluation
- 307-670-0757 300 W. Sinclair Gillette, WY 82718 Gillette College Gillette, WY 2015-17Document1 page307-670-0757 300 W. Sinclair Gillette, WY 82718 Gillette College Gillette, WY 2015-17api-356595508Pas encore d'évaluation
- Sigma Phi Epsilon: Kent's First Non Pledging Non Hazing Social Fraternity What Do You Want To Be A Part Of?Document1 pageSigma Phi Epsilon: Kent's First Non Pledging Non Hazing Social Fraternity What Do You Want To Be A Part Of?api-54584319Pas encore d'évaluation
- Escape22 Leaders DirectoryDocument1 pageEscape22 Leaders Directoryapi-26122632Pas encore d'évaluation
- Camp Type LegendDocument6 pagesCamp Type LegendViens DiviPas encore d'évaluation
- BC Resource Van Schedule MayDocument1 pageBC Resource Van Schedule MayfamilycentralPas encore d'évaluation
- SJVP Coop Procurent Manual 17-18Document26 pagesSJVP Coop Procurent Manual 17-18api-389555310Pas encore d'évaluation
- Troop 1894: Natalie Isabella EmiliaDocument1 pageTroop 1894: Natalie Isabella Emiliaapi-26216526Pas encore d'évaluation
- A Peek at Mrs. Zakharia's Week May 1 - 5: ST THDocument1 pageA Peek at Mrs. Zakharia's Week May 1 - 5: ST THNermeen ZakhariaPas encore d'évaluation
- Hsin-Yi, Tseng: ObjectiveDocument1 pageHsin-Yi, Tseng: Objectivecindy450117Pas encore d'évaluation
- Description: Tags: 2007-SchoolsDocument52 pagesDescription: Tags: 2007-Schoolsanon-451985Pas encore d'évaluation
- Description: Tags: Escgrants04Document5 pagesDescription: Tags: Escgrants04anon-283412Pas encore d'évaluation
- Fine Arts Private Tutor ListDocument6 pagesFine Arts Private Tutor Listapi-326384100Pas encore d'évaluation
- 螢幕截圖 2021-04-13 下午4.30.57Document4 pages螢幕截圖 2021-04-13 下午4.30.57Cherry WongPas encore d'évaluation
- NTBHA-Provider-Directory-English-REV-1-12-2023Document6 pagesNTBHA-Provider-Directory-English-REV-1-12-2023gc0117196Pas encore d'évaluation
- References GaDocument1 pageReferences Gaapi-534570687Pas encore d'évaluation
- ReferencesheetDocument1 pageReferencesheetapi-348403751Pas encore d'évaluation
- Isd Cy Team Contact Lists - Saint John To SussexDocument3 pagesIsd Cy Team Contact Lists - Saint John To Sussexapi-313161746Pas encore d'évaluation
- OMPOA Directory (Revised) (5.1) 01.21.2022Document3 pagesOMPOA Directory (Revised) (5.1) 01.21.2022dianePas encore d'évaluation
- Weekly Update 10-21-13Document3 pagesWeekly Update 10-21-13njtomlinsonPas encore d'évaluation
- June SatsangDetails 2022Document5 pagesJune SatsangDetails 2022smrithi MohanPas encore d'évaluation
- 8a Silver Wolves Virtual 11Document1 page8a Silver Wolves Virtual 11api-448405953Pas encore d'évaluation
- Queen and Nuc Certificate 2021Document9 pagesQueen and Nuc Certificate 2021Daniel MillerPas encore d'évaluation
- Roster 17-18Document2 pagesRoster 17-18api-273354845Pas encore d'évaluation
- Norterra Newsletter Oct 13-4Document2 pagesNorterra Newsletter Oct 13-4bpickering1Pas encore d'évaluation
- Draft Agenda: Board of County CommissionersDocument5 pagesDraft Agenda: Board of County CommissionersMichael AllenPas encore d'évaluation
- Gulf COVID Profile Report 2.10.21Document2 pagesGulf COVID Profile Report 2.10.21Michael AllenPas encore d'évaluation
- Draft Agenda: Board of County CommissionersDocument5 pagesDraft Agenda: Board of County CommissionersMichael Allen0% (1)
- Nov. 1, 2021 BOCC Draft Agenda OutlineDocument5 pagesNov. 1, 2021 BOCC Draft Agenda OutlineMichael AllenPas encore d'évaluation
- Franklin COVID Profile Report 09.18.20Document2 pagesFranklin COVID Profile Report 09.18.20manager2738Pas encore d'évaluation
- April 5, 2021 BOCC Draft Agenda OutlineDocument5 pagesApril 5, 2021 BOCC Draft Agenda OutlineMichael AllenPas encore d'évaluation
- COVID19 Update Franklin Gulf 8.13.21Document5 pagesCOVID19 Update Franklin Gulf 8.13.21Michael AllenPas encore d'évaluation
- Gulf County Meeting InfoDocument8 pagesGulf County Meeting InfoMichael AllenPas encore d'évaluation
- Oct. 4, 2021 BOCC Draft Agenda OutlineDocument6 pagesOct. 4, 2021 BOCC Draft Agenda OutlineMichael AllenPas encore d'évaluation
- March 22, 2021 Draft Agenda OutlineDocument5 pagesMarch 22, 2021 Draft Agenda OutlineMichael AllenPas encore d'évaluation
- Aug. 16, 2021 BOCC Draft Agenda OutlineDocument5 pagesAug. 16, 2021 BOCC Draft Agenda OutlineMichael AllenPas encore d'évaluation
- 02.12.21 Covid19 UpdateDocument2 pages02.12.21 Covid19 UpdateMichael AllenPas encore d'évaluation
- COVID19 Update Franklin Gulf 8.13.21Document5 pagesCOVID19 Update Franklin Gulf 8.13.21Michael AllenPas encore d'évaluation
- Aug. 2, 2021 BOCC Draft Agenda OutlineDocument5 pagesAug. 2, 2021 BOCC Draft Agenda OutlineMichael AllenPas encore d'évaluation
- March 2021 PDFDocument2 pagesMarch 2021 PDFMichael Allen100% (1)
- March 1, 2021 Draft Agenda OutlineDocument4 pagesMarch 1, 2021 Draft Agenda OutlineMichael AllenPas encore d'évaluation
- Feb. 1, 2021 Draft Agenda OutlineDocument4 pagesFeb. 1, 2021 Draft Agenda OutlineMichael AllenPas encore d'évaluation
- 02.12.21 Covid19 UpdateDocument2 pages02.12.21 Covid19 UpdateMichael AllenPas encore d'évaluation
- Jan. 19, 2021 Draft Agenda OutlineDocument4 pagesJan. 19, 2021 Draft Agenda OutlineMichael AllenPas encore d'évaluation
- 1-19-21 CRA Agenda CleanDocument4 pages1-19-21 CRA Agenda CleanMichael AllenPas encore d'évaluation
- Feb. 16, 2021 BOCC Draft Agenda OutlineDocument5 pagesFeb. 16, 2021 BOCC Draft Agenda OutlineMichael AllenPas encore d'évaluation
- Franklin COVID Profile Report 09.18.20Document2 pagesFranklin COVID Profile Report 09.18.20manager2738Pas encore d'évaluation
- Feb 2021 PDFDocument2 pagesFeb 2021 PDFMichael AllenPas encore d'évaluation
- January 2021 PDFDocument2 pagesJanuary 2021 PDFMichael AllenPas encore d'évaluation
- Gulf County Sheriff's Office Law Enforcement Summary July 6, 2020 - July 12, 2020Document2 pagesGulf County Sheriff's Office Law Enforcement Summary July 6, 2020 - July 12, 2020Michael AllenPas encore d'évaluation
- July 16 2020 Carrabelle P&Z AgendaDocument2 pagesJuly 16 2020 Carrabelle P&Z AgendaMichael AllenPas encore d'évaluation
- 07.13.2020 Franklin County COVID-19 UpdateDocument7 pages07.13.2020 Franklin County COVID-19 UpdateMichael AllenPas encore d'évaluation
- 07.10.2020 Franklin County COVID-19 UpdateDocument7 pages07.10.2020 Franklin County COVID-19 UpdateMichael AllenPas encore d'évaluation
- 7.13.20 Gulf COVID-19 UpdateDocument7 pages7.13.20 Gulf COVID-19 UpdateMichael AllenPas encore d'évaluation
- 6.24.20 Gulf County Covid-19 Daily UpdateDocument6 pages6.24.20 Gulf County Covid-19 Daily UpdateMichael AllenPas encore d'évaluation
- 19720en PDFDocument228 pages19720en PDFFransiskus Samuel RenaldiPas encore d'évaluation
- A CBRM Succession Planning For Board MembersDocument8 pagesA CBRM Succession Planning For Board MembersedrialdePas encore d'évaluation
- PAM-New Edition PDFDocument182 pagesPAM-New Edition PDFLalith RohanaPas encore d'évaluation
- Hospital MaintenanceDocument370 pagesHospital Maintenanceshahar397100% (2)
- VHT Situation AnalysisDocument246 pagesVHT Situation AnalysisKenneth BuyinzaPas encore d'évaluation
- Community Action For Health in Universal Health CareDocument35 pagesCommunity Action For Health in Universal Health CaresubharakhalPas encore d'évaluation
- Kenisha Lorvinsky - The Final Paper - 2809608Document19 pagesKenisha Lorvinsky - The Final Paper - 2809608api-502512624Pas encore d'évaluation
- St. Mary's University assesses quality healthcare delivery and customer satisfactionDocument60 pagesSt. Mary's University assesses quality healthcare delivery and customer satisfactionMICHAELPas encore d'évaluation
- Systems Thinking: Strengthening The Philippine Health SystemDocument13 pagesSystems Thinking: Strengthening The Philippine Health SystemRue LeePas encore d'évaluation
- Calbayog District Hospital (CDH)Document6 pagesCalbayog District Hospital (CDH)Nelin BarandinoPas encore d'évaluation
- Patient Safety Assignment 2015Document3 pagesPatient Safety Assignment 2015Aj AquinoPas encore d'évaluation
- Masteral Academic ProgramsDocument8 pagesMasteral Academic Programstom1975sgPas encore d'évaluation
- The Rise of The Intelligent Health SystemDocument299 pagesThe Rise of The Intelligent Health Systemradium.08slangPas encore d'évaluation
- Colin Leys, Health, Health Care and CapitalismDocument28 pagesColin Leys, Health, Health Care and CapitalismMarkus SchallhasPas encore d'évaluation
- Cost Accounting in Healthcare PDFDocument8 pagesCost Accounting in Healthcare PDFfilosofal62100% (2)
- Asia Pacific Observancy On HealthDocument92 pagesAsia Pacific Observancy On HealthbutterPas encore d'évaluation
- Saint Mary's Duluth Clinic Case StudyDocument12 pagesSaint Mary's Duluth Clinic Case StudyAdrianto Prayoga KusumaPas encore d'évaluation
- Target Marketing in The Health ServicesDocument5 pagesTarget Marketing in The Health ServicesSiti Fatmala RezekiPas encore d'évaluation
- WHO HIS SDS 2018.13 Eng PDFDocument64 pagesWHO HIS SDS 2018.13 Eng PDFArun MohanPas encore d'évaluation
- Tamilnadu Electropathy College Electropathy Course in MaduraiDocument5 pagesTamilnadu Electropathy College Electropathy Course in MaduraiRutvij AGPas encore d'évaluation
- Healthcare in BangladeshDocument2 pagesHealthcare in Bangladeshghostssoul 3Pas encore d'évaluation
- Budget Execution in Health: Concepts, Trends and Policy IssuesDocument44 pagesBudget Execution in Health: Concepts, Trends and Policy IssuesCandra, MPHPas encore d'évaluation
- Healthcare - Lifesciences and Review AlgeriaDocument63 pagesHealthcare - Lifesciences and Review AlgeriaAbhishek ModakPas encore d'évaluation
- Global Medicines Use in 2020: Outlook and ImplicationsDocument47 pagesGlobal Medicines Use in 2020: Outlook and Implicationssobrina25355Pas encore d'évaluation
- Agile Innovation To Transform Healthcare: Innovating in Complex Adaptive Systems Is An Everyday Process, Not A Light Bulb EventDocument8 pagesAgile Innovation To Transform Healthcare: Innovating in Complex Adaptive Systems Is An Everyday Process, Not A Light Bulb EventLex McGuirePas encore d'évaluation
- IFC HealthinAfrica Final 0 PDFDocument154 pagesIFC HealthinAfrica Final 0 PDFMidhun MohanPas encore d'évaluation
- Electronic Child Health Network (Echn) : Hospitals in OntarioDocument7 pagesElectronic Child Health Network (Echn) : Hospitals in OntariobevPas encore d'évaluation
- DR - Sreedhar Tirunagari BAMS, MD, MBA, PHD, Diploma in Public Health AYUSH ProfileDocument11 pagesDR - Sreedhar Tirunagari BAMS, MD, MBA, PHD, Diploma in Public Health AYUSH ProfileDr Sreedhar TirunagariPas encore d'évaluation
- The Challenges of Hospital Reform in MoroccoDocument10 pagesThe Challenges of Hospital Reform in MoroccoIJAR JOURNALPas encore d'évaluation
- End-Of-Use and End-Of-Life Medicines-Insights From Pharmaceutical Care Process Into Waste Medicines ManagementDocument19 pagesEnd-Of-Use and End-Of-Life Medicines-Insights From Pharmaceutical Care Process Into Waste Medicines ManagementerymshadikinPas encore d'évaluation
- The First 90 Days: Proven Strategies for Getting Up to Speed Faster and SmarterD'EverandThe First 90 Days: Proven Strategies for Getting Up to Speed Faster and SmarterÉvaluation : 4.5 sur 5 étoiles4.5/5 (122)
- The 7 Habits of Highly Effective People: The Infographics EditionD'EverandThe 7 Habits of Highly Effective People: The Infographics EditionÉvaluation : 4 sur 5 étoiles4/5 (2475)
- How the World Sees You: Discover Your Highest Value Through the Science of FascinationD'EverandHow the World Sees You: Discover Your Highest Value Through the Science of FascinationÉvaluation : 4 sur 5 étoiles4/5 (7)
- Summary: The Myth of Normal: Trauma, Illness, and Healing in a Toxic Culture By Gabor Maté MD & Daniel Maté: Key Takeaways, Summary & AnalysisD'EverandSummary: The Myth of Normal: Trauma, Illness, and Healing in a Toxic Culture By Gabor Maté MD & Daniel Maté: Key Takeaways, Summary & AnalysisÉvaluation : 4 sur 5 étoiles4/5 (9)
- Designing Your Life by Bill Burnett, Dave Evans - Book Summary: How to Build a Well-Lived, Joyful LifeD'EverandDesigning Your Life by Bill Burnett, Dave Evans - Book Summary: How to Build a Well-Lived, Joyful LifeÉvaluation : 4.5 sur 5 étoiles4.5/5 (61)
- Steal the Show: From Speeches to Job Interviews to Deal-Closing Pitches, How to Guarantee a Standing Ovation for All the Performances in Your LifeD'EverandSteal the Show: From Speeches to Job Interviews to Deal-Closing Pitches, How to Guarantee a Standing Ovation for All the Performances in Your LifeÉvaluation : 4.5 sur 5 étoiles4.5/5 (39)
- The Proximity Principle: The Proven Strategy That Will Lead to the Career You LoveD'EverandThe Proximity Principle: The Proven Strategy That Will Lead to the Career You LoveÉvaluation : 4.5 sur 5 étoiles4.5/5 (93)
- The 12 Week Year: Get More Done in 12 Weeks than Others Do in 12 MonthsD'EverandThe 12 Week Year: Get More Done in 12 Weeks than Others Do in 12 MonthsÉvaluation : 4.5 sur 5 étoiles4.5/5 (90)
- Uncontrolled Spread: Why COVID-19 Crushed Us and How We Can Defeat the Next PandemicD'EverandUncontrolled Spread: Why COVID-19 Crushed Us and How We Can Defeat the Next PandemicPas encore d'évaluation
- Do You Believe in Magic?: The Sense and Nonsense of Alternative MedicineD'EverandDo You Believe in Magic?: The Sense and Nonsense of Alternative MedicinePas encore d'évaluation
- Work Stronger: Habits for More Energy, Less Stress, and Higher Performance at WorkD'EverandWork Stronger: Habits for More Energy, Less Stress, and Higher Performance at WorkÉvaluation : 4.5 sur 5 étoiles4.5/5 (12)
- The 30 Day MBA: Your Fast Track Guide to Business SuccessD'EverandThe 30 Day MBA: Your Fast Track Guide to Business SuccessÉvaluation : 4.5 sur 5 étoiles4.5/5 (19)
- Company Of One: Why Staying Small Is the Next Big Thing for BusinessD'EverandCompany Of One: Why Staying Small Is the Next Big Thing for BusinessÉvaluation : 3.5 sur 5 étoiles3.5/5 (14)
- From Paycheck to Purpose: The Clear Path to Doing Work You LoveD'EverandFrom Paycheck to Purpose: The Clear Path to Doing Work You LoveÉvaluation : 4.5 sur 5 étoiles4.5/5 (39)
- Epic Measures: One Doctor. Seven Billion Patients.D'EverandEpic Measures: One Doctor. Seven Billion Patients.Évaluation : 4 sur 5 étoiles4/5 (13)
- The Confidence Code: The Science and Art of Self-Assurance--What Women Should KnowD'EverandThe Confidence Code: The Science and Art of Self-Assurance--What Women Should KnowÉvaluation : 4.5 sur 5 étoiles4.5/5 (175)
- The Dictionary of Body Language: A Field Guide to Human BehaviorD'EverandThe Dictionary of Body Language: A Field Guide to Human BehaviorÉvaluation : 4.5 sur 5 étoiles4.5/5 (95)
- The Ultimate Sales Letter, 4th Edition: Attract New Customers, Boost Your SalesD'EverandThe Ultimate Sales Letter, 4th Edition: Attract New Customers, Boost Your SalesÉvaluation : 4.5 sur 5 étoiles4.5/5 (98)
- When to Jump: If the Job You Have Isn't the Life You WantD'EverandWhen to Jump: If the Job You Have Isn't the Life You WantÉvaluation : 4.5 sur 5 étoiles4.5/5 (16)
- The Wisdom of Plagues: Lessons from 25 Years of Covering PandemicsD'EverandThe Wisdom of Plagues: Lessons from 25 Years of Covering PandemicsÉvaluation : 4.5 sur 5 étoiles4.5/5 (5)
- The Search for Self-Respect: Psycho-CyberneticsD'EverandThe Search for Self-Respect: Psycho-CyberneticsÉvaluation : 4.5 sur 5 étoiles4.5/5 (10)
- How to Be Everything: A Guide for Those Who (Still) Don't Know What They Want to Be When They Grow UpD'EverandHow to Be Everything: A Guide for Those Who (Still) Don't Know What They Want to Be When They Grow UpÉvaluation : 4 sur 5 étoiles4/5 (74)
- Real Artists Don't Starve: Timeless Strategies for Thriving in the New Creative AgeD'EverandReal Artists Don't Starve: Timeless Strategies for Thriving in the New Creative AgeÉvaluation : 4.5 sur 5 étoiles4.5/5 (197)
- The Definitive Executive Assistant and Managerial Handbook: A Professional Guide to Leadership for all PAs, Senior Secretaries, Office Managers and Executive AssistantsD'EverandThe Definitive Executive Assistant and Managerial Handbook: A Professional Guide to Leadership for all PAs, Senior Secretaries, Office Managers and Executive AssistantsÉvaluation : 3 sur 5 étoiles3/5 (2)