Vous aimerez peut-être aussi
- 1.porphyrin & Bile Pigment 2014Document94 pages1.porphyrin & Bile Pigment 2014Henyta TsuPas encore d'évaluation
- Clase 3 HepatogramaDocument9 pagesClase 3 HepatogramajuanpbagurPas encore d'évaluation
- Bilirubin MetabolismDocument5 pagesBilirubin MetabolismdwirosidPas encore d'évaluation
- Bilirrubinas 1Document4 pagesBilirrubinas 1Darwin GuisaoPas encore d'évaluation
- 73 Liver Chemistry and Function TestsDocument11 pages73 Liver Chemistry and Function TestsPaola PizanoPas encore d'évaluation
- Bilirubin MetabolismDocument11 pagesBilirubin MetabolismSavithri SubramaniamPas encore d'évaluation
- Bilirubin Metabolism - UpToDateDocument19 pagesBilirubin Metabolism - UpToDateMihaela Alexandra RepeziPas encore d'évaluation
- Neonatal HyperbilirubinemiaDocument36 pagesNeonatal HyperbilirubinemiamahmmoudeltaweelPas encore d'évaluation
- Hereditary Jaundice Cap125Document90 pagesHereditary Jaundice Cap125BarDFPas encore d'évaluation
- Print - Chapter 13. Bilirubin Formation and Excretion by The LiverDocument11 pagesPrint - Chapter 13. Bilirubin Formation and Excretion by The LiverbelaginaPas encore d'évaluation
- Bilirubin Metabolism: Author Section Editor Deputy EditorDocument7 pagesBilirubin Metabolism: Author Section Editor Deputy EditorGeorge Williame RigamotoPas encore d'évaluation
- Jaundice EnglishDocument5 pagesJaundice EnglishArinaManaSikanaPas encore d'évaluation
- Review On Evolution of Methods of BilirubinDocument13 pagesReview On Evolution of Methods of BilirubinAzzzPas encore d'évaluation
- Bac GroundDocument6 pagesBac GroundRitu Ayu PutriPas encore d'évaluation
- Neonatal JaundiceDocument4 pagesNeonatal JaundiceChristian Eduard de DiosPas encore d'évaluation
- Bilirubin Metabolism Applied Physiology PDFDocument6 pagesBilirubin Metabolism Applied Physiology PDFRenata SetyariantikaPas encore d'évaluation
- Gilbert Syndrome and Unconjugated Hyperbilirubinemia Due To Bilirubin Overproduction - UpToDateDocument22 pagesGilbert Syndrome and Unconjugated Hyperbilirubinemia Due To Bilirubin Overproduction - UpToDateMartinaAstMonPas encore d'évaluation
- TAYLOR 1984 AnaesthesiaDocument3 pagesTAYLOR 1984 Anaesthesiapolly91Pas encore d'évaluation
- Lec 2.5 Dr. Ngadikun 2016 PorfirinDocument33 pagesLec 2.5 Dr. Ngadikun 2016 PorfirinRobertOktaChandraPas encore d'évaluation
- Bilirubin MethodsDocument12 pagesBilirubin MethodsDarshana JuvekarPas encore d'évaluation
- 06 Bilirubin Metabolism016Document28 pages06 Bilirubin Metabolism016Arif NabeelPas encore d'évaluation
- JaundiceDocument12 pagesJaundiceAnonymous v8AfMnT5Pas encore d'évaluation
- Neonatal JaundiceDocument30 pagesNeonatal JaundiceAnonymous Y3fqBduPas encore d'évaluation
- First Page PDFDocument1 pageFirst Page PDFDora FrimpongPas encore d'évaluation
- Core Concepts:: Bilirubin MetabolismDocument9 pagesCore Concepts:: Bilirubin MetabolismManasye AlanPas encore d'évaluation
- 8 BilirubinDocument25 pages8 BilirubinTagreed DerarPas encore d'évaluation
- Measurement and Clinical Usefulness of Bilirubin in Liver DiseaseDocument10 pagesMeasurement and Clinical Usefulness of Bilirubin in Liver DiseaseNjeodo VignyPas encore d'évaluation
- Liver Function Test (TSB)Document25 pagesLiver Function Test (TSB)shafyd ramdanPas encore d'évaluation
- The Significance Malbuminuria" (Proteinuria) : CompletelyDocument3 pagesThe Significance Malbuminuria" (Proteinuria) : CompletelyAmanuel MaruPas encore d'évaluation
- Physiology and Pathology BILIRUBIN SINTESISDocument9 pagesPhysiology and Pathology BILIRUBIN SINTESISIda Bagus SaktianaPas encore d'évaluation
- Ictericia Diagnostico Ravindran2020Document7 pagesIctericia Diagnostico Ravindran2020Francisco CarpioPas encore d'évaluation
- Monorafia SP BryanDocument45 pagesMonorafia SP BryanBryan SanchezPas encore d'évaluation
- Lecture Notes: Clinical Chemistry of LiverDocument38 pagesLecture Notes: Clinical Chemistry of LivershehnilaPas encore d'évaluation
- Name of Test:-Serum Bilirubin Test: Tests For Liver FunctionDocument4 pagesName of Test:-Serum Bilirubin Test: Tests For Liver FunctionHiba EmadPas encore d'évaluation
- Hiperbilirrubinemia DirectaDocument9 pagesHiperbilirrubinemia DirectaRonal Cadillo MedinaPas encore d'évaluation
- J Mpsur 2017 09 012Document7 pagesJ Mpsur 2017 09 012riffarsyad100% (1)
- Metabolism of Bilirubin and Bile Salt SynthesisDocument34 pagesMetabolism of Bilirubin and Bile Salt SynthesisKumail LakraPas encore d'évaluation
- PPPPDocument6 pagesPPPPChristy Ada IjeomaPas encore d'évaluation
- Advances in Laboratory Diagnosis and Clinical Management of Gilbert Disease A Comprehensive ReviewDocument6 pagesAdvances in Laboratory Diagnosis and Clinical Management of Gilbert Disease A Comprehensive ReviewKIU PUBLICATION AND EXTENSIONPas encore d'évaluation
- Assessment of Jaundice in The Hospitalized Patient PDFDocument16 pagesAssessment of Jaundice in The Hospitalized Patient PDFlaura canoPas encore d'évaluation
- Core Concepts Bilirrubin MetabolismDocument9 pagesCore Concepts Bilirrubin MetabolismAngelina ChunPas encore d'évaluation
- Classification and Causes of Jaundice or Asymptomatic HyperbilirubinemiaDocument22 pagesClassification and Causes of Jaundice or Asymptomatic HyperbilirubinemiaVictor MarquesPas encore d'évaluation
- Research ProposalDocument5 pagesResearch ProposalZablon KodilaPas encore d'évaluation
- 1 Core Concepts Bilirubin MetabolismDocument9 pages1 Core Concepts Bilirubin Metabolismlink0105Pas encore d'évaluation
- 2.6 Bilirubin DeterminationDocument9 pages2.6 Bilirubin Determinationiridescent brightwinPas encore d'évaluation
- Case StudiesDocument28 pagesCase StudiespeanantPas encore d'évaluation
- Kuliah Bill Gite Harly 2013Document41 pagesKuliah Bill Gite Harly 2013DaniaPutriPas encore d'évaluation
- NIH Public Access: Author ManuscriptDocument10 pagesNIH Public Access: Author ManuscriptNofiyanty NicolasPas encore d'évaluation
- Mercy Thomas Mechanism of Bilirubin Elimination inDocument9 pagesMercy Thomas Mechanism of Bilirubin Elimination inBladimir CentenoPas encore d'évaluation
- Bilirubin Metabolism and Liver Function Test by V e BoloyaDocument35 pagesBilirubin Metabolism and Liver Function Test by V e BoloyaPrincewill SeiyefaPas encore d'évaluation
- L6 - Bilirubin MetabolismDocument28 pagesL6 - Bilirubin Metabolismyouservezeropurpose113Pas encore d'évaluation
- Role of Albumin in Cirrhosis PatientDocument7 pagesRole of Albumin in Cirrhosis Patientgigih85Pas encore d'évaluation
- IJRPR5933Document8 pagesIJRPR5933rifa iPas encore d'évaluation
- Albumin Infusion in Liver Cirrhotic Patients: Ni Made Renny A. Rena, I Dewa Nyoman WibawaDocument7 pagesAlbumin Infusion in Liver Cirrhotic Patients: Ni Made Renny A. Rena, I Dewa Nyoman WibawaChris MulyoPas encore d'évaluation
- TESTS FOR LIVER FUNCTION Arneson BookDocument28 pagesTESTS FOR LIVER FUNCTION Arneson Bookzahrotun nisaPas encore d'évaluation
- Clinical Chemistry of Liver-4th Level-3!12!2012Document39 pagesClinical Chemistry of Liver-4th Level-3!12!2012Sena YadesaPas encore d'évaluation
- Conjugated Hyperbilirubinemia: Presented by Ri 黃纓雰 91-5-6Document20 pagesConjugated Hyperbilirubinemia: Presented by Ri 黃纓雰 91-5-6Alexander NevidimovPas encore d'évaluation
- Liver PathologyDocument35 pagesLiver Pathologynhgwdwffp2Pas encore d'évaluation
- Leptin: Regulation and Clinical ApplicationsD'EverandLeptin: Regulation and Clinical ApplicationsSam Dagogo-Jack, MDPas encore d'évaluation
- International Textbook of Diabetes MellitusD'EverandInternational Textbook of Diabetes MellitusR. A. DeFronzoPas encore d'évaluation
- Why Does Obesity Cause Diabetes?: PerspectiveDocument10 pagesWhy Does Obesity Cause Diabetes?: PerspectiveJorge MedinaPas encore d'évaluation
- Bile (Report in Biochemistry)Document2 pagesBile (Report in Biochemistry)Luci BernasPas encore d'évaluation
- Fatty Liver AssignmentDocument9 pagesFatty Liver AssignmentMaryam ShahzadiPas encore d'évaluation
- Obs JauDocument22 pagesObs JauRavi GuptaPas encore d'évaluation
- SamanthaDocument3 pagesSamanthaIVy ViOlet ThOrnPas encore d'évaluation
- Francisco Varela - Intimate Distances - Fragments For A Phenomenology of Organ TransplantationDocument30 pagesFrancisco Varela - Intimate Distances - Fragments For A Phenomenology of Organ TransplantationeekeekeekeekPas encore d'évaluation
- Serology and Ultrasound For Diagnosis of Choledocolitiasis 2014Document5 pagesSerology and Ultrasound For Diagnosis of Choledocolitiasis 2014DannyPas encore d'évaluation
- Sulfur Deficiency Stephanie SeneffDocument19 pagesSulfur Deficiency Stephanie Seneffgkebiz100% (1)
- Beyond Reality No 16Document68 pagesBeyond Reality No 16pnutbuttahunny0% (1)
- Nihms 818708Document22 pagesNihms 818708bela RachmanPas encore d'évaluation
- GIT NotesDocument23 pagesGIT NotesGrey SyPas encore d'évaluation
- MR Santosh Rai: Method: CalculatedDocument10 pagesMR Santosh Rai: Method: CalculatedSantosh RaiPas encore d'évaluation
- Hepatic SteatosisDocument9 pagesHepatic Steatosiss12144017Pas encore d'évaluation
- Calculous Biliary DiseaseDocument71 pagesCalculous Biliary DiseaseMinnossPas encore d'évaluation
- 6 - Clinical Biochemistry - 1001411Document14 pages6 - Clinical Biochemistry - 1001411bsmallahPas encore d'évaluation
- Germany Homeopathic Medicines ListDocument66 pagesGermany Homeopathic Medicines Listar hijaziPas encore d'évaluation
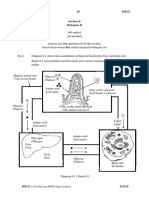
- Paper 2 Section BDocument10 pagesPaper 2 Section BtaePas encore d'évaluation
- 004 LabsDiagnosticsManualDocument64 pages004 LabsDiagnosticsManualRaju Niraula100% (1)
- HydropsDocument20 pagesHydropsKevin Satya Gananda100% (1)
- Urine Therapy by Flora Peschek Böhmer 1 PDFDocument160 pagesUrine Therapy by Flora Peschek Böhmer 1 PDFAndy Ochumba100% (8)
- Liver Structure Funciton QnsDocument4 pagesLiver Structure Funciton QnsNoora AttariPas encore d'évaluation
- Digestive SystemDocument73 pagesDigestive SystemJustine Mae OyongPas encore d'évaluation
- FatDocument147 pagesFatNenad Vujosevic100% (3)
- Jaundice - StatPearls - NCBI BookshelfDocument8 pagesJaundice - StatPearls - NCBI Bookshelfal ghiffari muhammad rayhanPas encore d'évaluation
- RETRACINGDocument54 pagesRETRACINGzer rePas encore d'évaluation
- CV - DR ManojDocument9 pagesCV - DR ManojshubahmPas encore d'évaluation
- Chapter - 2 - C - II Liver CirrhosisDocument39 pagesChapter - 2 - C - II Liver CirrhosisEmmaPas encore d'évaluation
- Frog DissectionDocument7 pagesFrog DissectionriancfPas encore d'évaluation
- KROK2 2008 Paper (200 QS)Document61 pagesKROK2 2008 Paper (200 QS)Ali ZeeshanPas encore d'évaluation
- Assessment Mouth and Oropharynx LipsDocument8 pagesAssessment Mouth and Oropharynx LipsQuinmarc LimPas encore d'évaluation