Vous aimerez peut-être aussi
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeD'EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeÉvaluation : 4 sur 5 étoiles4/5 (5794)
- Case Study GonorrheaDocument19 pagesCase Study GonorrheaErika TheresePas encore d'évaluation
- Shoe Dog: A Memoir by the Creator of NikeD'EverandShoe Dog: A Memoir by the Creator of NikeÉvaluation : 4.5 sur 5 étoiles4.5/5 (537)
- S03 - Lpl-Preet Vihar C-49, Main Vikas Marg, Preet Vihar, New DELHI-110092 DelhiDocument4 pagesS03 - Lpl-Preet Vihar C-49, Main Vikas Marg, Preet Vihar, New DELHI-110092 DelhiAr Ayoushika AbrolPas encore d'évaluation
- Pathogens Gallery Walk PostersDocument5 pagesPathogens Gallery Walk Postersapi-293084509Pas encore d'évaluation
- The Yellow House: A Memoir (2019 National Book Award Winner)D'EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Évaluation : 4 sur 5 étoiles4/5 (98)
- Second MBBS Microbiology SyllabusDocument29 pagesSecond MBBS Microbiology SyllabusUday KolhePas encore d'évaluation
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceD'EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceÉvaluation : 4 sur 5 étoiles4/5 (895)
- Koberova. 2020. RAS in ChildrenDocument5 pagesKoberova. 2020. RAS in ChildrenRachel RoselanyPas encore d'évaluation
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersD'EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersÉvaluation : 4.5 sur 5 étoiles4.5/5 (344)
- Pathoma Notes CH 1-3Document11 pagesPathoma Notes CH 1-3imdaking12392% (25)
- The Little Book of Hygge: Danish Secrets to Happy LivingD'EverandThe Little Book of Hygge: Danish Secrets to Happy LivingÉvaluation : 3.5 sur 5 étoiles3.5/5 (399)
- Zoonotic DiseasesDocument96 pagesZoonotic DiseasesWakjira GemedaPas encore d'évaluation
- Grit: The Power of Passion and PerseveranceD'EverandGrit: The Power of Passion and PerseveranceÉvaluation : 4 sur 5 étoiles4/5 (588)
- Pathophysiology of Acquired Aplastic AnaemiaDocument10 pagesPathophysiology of Acquired Aplastic AnaemiaSatya PratiwiPas encore d'évaluation
- The Emperor of All Maladies: A Biography of CancerD'EverandThe Emperor of All Maladies: A Biography of CancerÉvaluation : 4.5 sur 5 étoiles4.5/5 (271)
- Usmle ExamDocument13 pagesUsmle ExamAmal Alameen100% (2)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaD'EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaÉvaluation : 4.5 sur 5 étoiles4.5/5 (266)
- C-Reactive Protein Levels of Sepsis Patients: A Comparison of Three Immunoassay MethodsDocument5 pagesC-Reactive Protein Levels of Sepsis Patients: A Comparison of Three Immunoassay MethodslidawatiPas encore d'évaluation
- Never Split the Difference: Negotiating As If Your Life Depended On ItD'EverandNever Split the Difference: Negotiating As If Your Life Depended On ItÉvaluation : 4.5 sur 5 étoiles4.5/5 (838)
- 2007, Volume 67, Issue 1Document152 pages2007, Volume 67, Issue 1Kareem JakouchPas encore d'évaluation
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryD'EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryÉvaluation : 3.5 sur 5 étoiles3.5/5 (231)
- Rinderpest (Cattle Plague) : Dr. Munguti E.M AHITI NdombaDocument14 pagesRinderpest (Cattle Plague) : Dr. Munguti E.M AHITI NdombaFazalPas encore d'évaluation
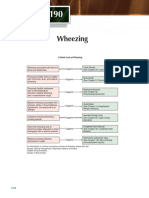
- Wheezing: A Quick Look at WheezingDocument1 pageWheezing: A Quick Look at WheezingpelinPas encore d'évaluation
- On Fire: The (Burning) Case for a Green New DealD'EverandOn Fire: The (Burning) Case for a Green New DealÉvaluation : 4 sur 5 étoiles4/5 (73)
- IMMUNIZATION LecDocument77 pagesIMMUNIZATION LecKavya ReddyPas encore d'évaluation
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureD'EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureÉvaluation : 4.5 sur 5 étoiles4.5/5 (474)
- Salmonellosis: Early Chick Mortality Necrosis Marbled Spleen Ophoritis SalpingitisDocument8 pagesSalmonellosis: Early Chick Mortality Necrosis Marbled Spleen Ophoritis Salpingitisjazz100% (2)
- Team of Rivals: The Political Genius of Abraham LincolnD'EverandTeam of Rivals: The Political Genius of Abraham LincolnÉvaluation : 4.5 sur 5 étoiles4.5/5 (234)
- B Cell PDFDocument65 pagesB Cell PDFChandan KumarPas encore d'évaluation
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyD'EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyÉvaluation : 3.5 sur 5 étoiles3.5/5 (2259)
- Cell Culture Bioprocess EngineeringDocument337 pagesCell Culture Bioprocess EngineeringIRFAN AHANGERPas encore d'évaluation
- Systemic Lupus Erythematosus Discoid in Dog CanisDocument4 pagesSystemic Lupus Erythematosus Discoid in Dog CanisAlina BlondaPas encore d'évaluation
- Spirochetes and Curved RodsDocument54 pagesSpirochetes and Curved RodsDegee O. GonzalesPas encore d'évaluation
- DS CD34 MicroBead Kit HDocument4 pagesDS CD34 MicroBead Kit Hsankalpa3Pas encore d'évaluation
- Protocol of TB TreatmentDocument15 pagesProtocol of TB TreatmentDegee GonzalesPas encore d'évaluation
- The Unwinding: An Inner History of the New AmericaD'EverandThe Unwinding: An Inner History of the New AmericaÉvaluation : 4 sur 5 étoiles4/5 (45)
- ABULALAS Vaccinated Inventory February 15 2023Document197 pagesABULALAS Vaccinated Inventory February 15 2023Rhea MagsakayPas encore d'évaluation
- Chap 15Document40 pagesChap 15Koby100% (4)
- CROUPDocument26 pagesCROUPRahul MehtaPas encore d'évaluation
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreD'EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreÉvaluation : 4 sur 5 étoiles4/5 (1090)
- Strep Throat?: What Do I Need To Know AboutDocument1 pageStrep Throat?: What Do I Need To Know AboutHandre PutraPas encore d'évaluation
- Asepsis and InfectionDocument6 pagesAsepsis and InfectionMabes100% (1)
- Immune System PosterDocument5 pagesImmune System PosterMarta Pérez MadridPas encore d'évaluation
- CELLUTISDocument16 pagesCELLUTISNorshahidah Ieda0% (1)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)D'EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Évaluation : 4.5 sur 5 étoiles4.5/5 (121)
- Policies & Procedures On Infection Prevention and ControlDocument308 pagesPolicies & Procedures On Infection Prevention and ControlHawthorn APas encore d'évaluation
- A. Why Blood A Is More Easily Attacked by Viruses Than O ?Document3 pagesA. Why Blood A Is More Easily Attacked by Viruses Than O ?Sonia KomalaPas encore d'évaluation
- Her Body and Other Parties: StoriesD'EverandHer Body and Other Parties: StoriesÉvaluation : 4 sur 5 étoiles4/5 (821)