Vous aimerez peut-être aussi
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryD'EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryÉvaluation : 3.5 sur 5 étoiles3.5/5 (231)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)D'EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Évaluation : 4.5 sur 5 étoiles4.5/5 (120)
- Grit: The Power of Passion and PerseveranceD'EverandGrit: The Power of Passion and PerseveranceÉvaluation : 4 sur 5 étoiles4/5 (588)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaD'EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaÉvaluation : 4.5 sur 5 étoiles4.5/5 (266)
- The Little Book of Hygge: Danish Secrets to Happy LivingD'EverandThe Little Book of Hygge: Danish Secrets to Happy LivingÉvaluation : 3.5 sur 5 étoiles3.5/5 (399)
- Never Split the Difference: Negotiating As If Your Life Depended On ItD'EverandNever Split the Difference: Negotiating As If Your Life Depended On ItÉvaluation : 4.5 sur 5 étoiles4.5/5 (838)
- Shoe Dog: A Memoir by the Creator of NikeD'EverandShoe Dog: A Memoir by the Creator of NikeÉvaluation : 4.5 sur 5 étoiles4.5/5 (537)
- The Emperor of All Maladies: A Biography of CancerD'EverandThe Emperor of All Maladies: A Biography of CancerÉvaluation : 4.5 sur 5 étoiles4.5/5 (271)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeD'EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeÉvaluation : 4 sur 5 étoiles4/5 (5794)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyD'EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyÉvaluation : 3.5 sur 5 étoiles3.5/5 (2259)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersD'EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersÉvaluation : 4.5 sur 5 étoiles4.5/5 (344)
- Team of Rivals: The Political Genius of Abraham LincolnD'EverandTeam of Rivals: The Political Genius of Abraham LincolnÉvaluation : 4.5 sur 5 étoiles4.5/5 (234)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreD'EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreÉvaluation : 4 sur 5 étoiles4/5 (1090)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceD'EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceÉvaluation : 4 sur 5 étoiles4/5 (895)
- Her Body and Other Parties: StoriesD'EverandHer Body and Other Parties: StoriesÉvaluation : 4 sur 5 étoiles4/5 (821)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureD'EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureÉvaluation : 4.5 sur 5 étoiles4.5/5 (474)
- The Unwinding: An Inner History of the New AmericaD'EverandThe Unwinding: An Inner History of the New AmericaÉvaluation : 4 sur 5 étoiles4/5 (45)
- The Yellow House: A Memoir (2019 National Book Award Winner)D'EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Évaluation : 4 sur 5 étoiles4/5 (98)
- On Fire: The (Burning) Case for a Green New DealD'EverandOn Fire: The (Burning) Case for a Green New DealÉvaluation : 4 sur 5 étoiles4/5 (73)
- Turning Toward PainDocument9 pagesTurning Toward PainScheckyPas encore d'évaluation
- Kiss Forex How To Trade Ichimoku PDFDocument72 pagesKiss Forex How To Trade Ichimoku PDFSastryassociates Chartered100% (3)
- 100 Years of Hydrodynamic PDFDocument28 pages100 Years of Hydrodynamic PDFnikodjolePas encore d'évaluation
- Avionic ArchitectureDocument127 pagesAvionic ArchitectureRohithsai PasupuletiPas encore d'évaluation
- George Lakoff - Metaphor, Morality & Politics, Or, Why Conservatives Have Left Liberals in The DustDocument22 pagesGeorge Lakoff - Metaphor, Morality & Politics, Or, Why Conservatives Have Left Liberals in The DustSchecky100% (5)
- George Lakoff - Metaphor, Morality & Politics, Or, Why Conservatives Have Left Liberals in The DustDocument22 pagesGeorge Lakoff - Metaphor, Morality & Politics, Or, Why Conservatives Have Left Liberals in The DustSchecky100% (5)
- General Anaesthesia MCQsDocument5 pagesGeneral Anaesthesia MCQsWasi Khan100% (3)
- George Lakoff - Cognitive ModelsDocument20 pagesGeorge Lakoff - Cognitive ModelsSchecky100% (10)
- Tim Ingold - From The Transmission of Representations To The Education of Attention PDFDocument26 pagesTim Ingold - From The Transmission of Representations To The Education of Attention PDFtomasfeza5210100% (1)
- Tech Manual 1396 Rev. B: 3.06/4.06" 15,000 Psi ES BOPDocument39 pagesTech Manual 1396 Rev. B: 3.06/4.06" 15,000 Psi ES BOPEl Mundo De Yosed100% (1)
- George Lakoff - Metaphorical ThoughtDocument41 pagesGeorge Lakoff - Metaphorical ThoughtSchecky100% (2)
- Varaah KavachDocument7 pagesVaraah KavachBalagei Nagarajan100% (1)
- George Lakoff - The Contemporary Theory of MetaphorDocument46 pagesGeorge Lakoff - The Contemporary Theory of MetaphorAntonio Giovinazzo100% (1)
- ThinkingPoints Chapter1Document7 pagesThinkingPoints Chapter1marklarPas encore d'évaluation
- Mary Magdalene Be Author of The Fourth GospelDocument14 pagesMary Magdalene Be Author of The Fourth GospelWilliam MamudiPas encore d'évaluation
- JokoBeck ThePoolsDocument3 pagesJokoBeck ThePoolsScheckyPas encore d'évaluation
- Pema Chodron QuotesDocument2 pagesPema Chodron QuotesSchecky100% (1)
- Paulcuffee SierraleoneliberiaDocument1 pagePaulcuffee SierraleoneliberiaScheckyPas encore d'évaluation
- Holocaust Literacy LessonsDocument5 pagesHolocaust Literacy LessonsScheckyPas encore d'évaluation
- Living Conditions 5507596Document5 pagesLiving Conditions 5507596ScheckyPas encore d'évaluation
- Selections From Paul JohnsonDocument5 pagesSelections From Paul JohnsonScheckyPas encore d'évaluation
- HP Mayjune BigDocument1 pageHP Mayjune BigScheckyPas encore d'évaluation
- Implications of Lipid Biology For The Pathogenesis of SchizophreniaDocument12 pagesImplications of Lipid Biology For The Pathogenesis of SchizophreniaScheckyPas encore d'évaluation
- Family LeaveDocument7 pagesFamily LeaveScheckyPas encore d'évaluation
- Rhino TankDocument1 pageRhino TankScheckyPas encore d'évaluation
- HP March April BigDocument1 pageHP March April BigScheckyPas encore d'évaluation
- George Lakoff - Mitecs - ReviewDocument15 pagesGeorge Lakoff - Mitecs - ReviewScheckyPas encore d'évaluation
- George Lakoff - Framing The Debate It's All GOP 20070104Document2 pagesGeorge Lakoff - Framing The Debate It's All GOP 20070104ScheckyPas encore d'évaluation
- George Lakoff - Don't Think of An Elephant - Know Your Values and Frame The DebateDocument142 pagesGeorge Lakoff - Don't Think of An Elephant - Know Your Values and Frame The DebateSchecky100% (4)
- In Uence of Gender On Social Outcome in SchizophreniaDocument7 pagesIn Uence of Gender On Social Outcome in SchizophreniaScheckyPas encore d'évaluation
- George Lakoff - Framing The Issue - How Conservatives Use Language To Dominate Politics 2003.10.27Document5 pagesGeorge Lakoff - Framing The Issue - How Conservatives Use Language To Dominate Politics 2003.10.27ScheckyPas encore d'évaluation
- George Lakoff - Metaphors of TerrorDocument13 pagesGeorge Lakoff - Metaphors of TerrorSchecky100% (1)
- Cognitive Subprocesses and Schizophrenia. A. Reaction-Time DecompositionDocument10 pagesCognitive Subprocesses and Schizophrenia. A. Reaction-Time DecompositionScheckyPas encore d'évaluation
- CVPDPLANDocument8 pagesCVPDPLANScheckyPas encore d'évaluation
- California Losing LusterDocument4 pagesCalifornia Losing LusterScheckyPas encore d'évaluation
- Challenge Day InformationDocument7 pagesChallenge Day InformationScheckyPas encore d'évaluation
- California Widening DivideDocument3 pagesCalifornia Widening DivideScheckyPas encore d'évaluation
- Karan AsDocument3 pagesKaran AsHariPas encore d'évaluation
- Progress Report Week#9 UlubeluDocument6 pagesProgress Report Week#9 UlubelutiantaufikPas encore d'évaluation
- Diablo Watch Newsletter, FALL 2009 Save Mount DiabloDocument16 pagesDiablo Watch Newsletter, FALL 2009 Save Mount DiabloIoannqisHatzopoulosPas encore d'évaluation
- Aplikasi Sistem Penuaian Air Hujan (Spah) Di Kawasan PerumahanDocument18 pagesAplikasi Sistem Penuaian Air Hujan (Spah) Di Kawasan PerumahanFarid Che DeramanPas encore d'évaluation
- Volvo PDFDocument218 pagesVolvo PDFNelio Lara Ricaldi0% (1)
- IMS Institute BelgradeDocument10 pagesIMS Institute BelgradeBoško JanjuševićPas encore d'évaluation
- Disa Match: A Match You Can Count OnDocument8 pagesDisa Match: A Match You Can Count OngPas encore d'évaluation
- Tank Gauging TankvisionDocument31 pagesTank Gauging Tankvisionkhangduongda3Pas encore d'évaluation
- With EU Stage V Engine Installed: 200 HP (149 KW) / 2,200 RPMDocument4 pagesWith EU Stage V Engine Installed: 200 HP (149 KW) / 2,200 RPMSara Sarmiento EcheverryPas encore d'évaluation
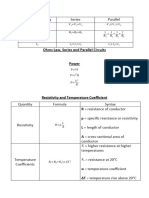
- EET - Formulas - Christmas TermDocument3 pagesEET - Formulas - Christmas TermJMDPas encore d'évaluation
- Fantasy AGE - Spell SheetDocument2 pagesFantasy AGE - Spell SheetpacalypsePas encore d'évaluation
- Augocom Micro 768 Battery Tester User ManualDocument29 pagesAugocom Micro 768 Battery Tester User ManualJorge PontonPas encore d'évaluation
- Tempera 2018 AbstractsDocument45 pagesTempera 2018 AbstractsGerard Emmanuel KamdemPas encore d'évaluation
- Study of Mosquito Larvicidal Effects of (Bitter Gourd) Extracts As NanopowderDocument3 pagesStudy of Mosquito Larvicidal Effects of (Bitter Gourd) Extracts As NanopowderAnonymous AkoPas encore d'évaluation
- Monk - Way of The Elements RevisedDocument3 pagesMonk - Way of The Elements Revisedluigipokeboy0% (1)
- University of Engineering and Technology TaxilaDocument5 pagesUniversity of Engineering and Technology TaxilagndfgPas encore d'évaluation
- Texas Instruments FootprintsDocument7 pagesTexas Instruments FootprintsSteve SmithPas encore d'évaluation
- Master Key Utbk Saintek 2022 (Paket 3) Bahasa InggrisDocument5 pagesMaster Key Utbk Saintek 2022 (Paket 3) Bahasa InggrisRina SetiawatiPas encore d'évaluation
- Arc 2019-2020Document95 pagesArc 2019-2020AEN HTM DD1 HTM DD1Pas encore d'évaluation
- Column c4 From 3rd FloorDocument1 pageColumn c4 From 3rd Floor1man1bookPas encore d'évaluation
- Theology of Work and Practical ImplicationsDocument28 pagesTheology of Work and Practical ImplicationsVinicius CardosoPas encore d'évaluation
- In Truth To Mollusca According To New Studies by J RutherfordDocument4 pagesIn Truth To Mollusca According To New Studies by J RutherfordbalaiPas encore d'évaluation
- Amc 20-21Document33 pagesAmc 20-21Vasco M C SantosPas encore d'évaluation