Vous aimerez peut-être aussi
- Adverse Drug Reaction FormDocument2 pagesAdverse Drug Reaction FormDhananjay Saini100% (1)
- ADR Reporting FormDocument2 pagesADR Reporting FormApoorva Tatti100% (1)
- ADR Reporting FormDocument2 pagesADR Reporting FormPiyush PriyadarshanPas encore d'évaluation
- CNS DR Najeeb Notes Part 3Document3 pagesCNS DR Najeeb Notes Part 3Dr. Tarush DhawanPas encore d'évaluation
- Adr Form Pvpi PDFDocument2 pagesAdr Form Pvpi PDFAndris SundaePas encore d'évaluation
- ADRnewReporting Form 1.4Document2 pagesADRnewReporting Form 1.4Sourabh kundara0% (1)
- Adrrf 2Document1 pageAdrrf 2Aniruddha ChatterjeePas encore d'évaluation
- Suspected Adverse Drug Reaction Reporting Form: Indian Pharmacopoeia CommissionDocument3 pagesSuspected Adverse Drug Reaction Reporting Form: Indian Pharmacopoeia CommissionAshu AmmuPas encore d'évaluation
- Med-F-020 Adverse Drug Reaction Reporting FormDocument2 pagesMed-F-020 Adverse Drug Reaction Reporting Formdrakmalik71Pas encore d'évaluation
- DRAP New Suspected Adverse Reaction Reporting Form For Health Care Professionals PDFDocument3 pagesDRAP New Suspected Adverse Reaction Reporting Form For Health Care Professionals PDFShakil Khan100% (1)
- Adobe Scan Feb 16, 2024Document1 pageAdobe Scan Feb 16, 2024islamomarfaruk39Pas encore d'évaluation
- Adr Form 10Document3 pagesAdr Form 10doctor uroosaPas encore d'évaluation
- ADR Form PDFDocument1 pageADR Form PDFChatie PipitPas encore d'évaluation
- Side Effect Reporting FormDocument2 pagesSide Effect Reporting FormBBB.AAAPas encore d'évaluation
- Adverse Drug Reaction FormDocument2 pagesAdverse Drug Reaction FormAre Pee Etc0% (1)
- Case 4 - MCNP - Miguel, Mark Darren, T.Document3 pagesCase 4 - MCNP - Miguel, Mark Darren, T.markPas encore d'évaluation
- Date of Onset: Am, PM: Fields Must Be Completed. All Reports Are ConfidentialDocument2 pagesDate of Onset: Am, PM: Fields Must Be Completed. All Reports Are ConfidentialJonathan Deguzman100% (1)
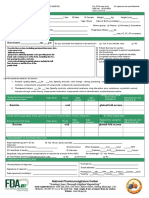
- FDA Phils-Suspected-Side-Effects-Reporting-Form-v6.0Document3 pagesFDA Phils-Suspected-Side-Effects-Reporting-Form-v6.0Marizel PormilosPas encore d'évaluation
- ADR AEFI Reporting FormDocument1 pageADR AEFI Reporting Formgulafsha1Pas encore d'évaluation
- A. Patient Details: Form NO. ADR-1Document2 pagesA. Patient Details: Form NO. ADR-1Mkamal MosaPas encore d'évaluation
- Adr FormDocument2 pagesAdr FormZaira Clarisse de GuzmanPas encore d'évaluation
- Adverse Events FormDocument2 pagesAdverse Events Formkepk.rsbmprovbaliPas encore d'évaluation
- Vaers FormDocument2 pagesVaers Formgdparduhn3Pas encore d'évaluation
- Aefi CifDocument6 pagesAefi CifVic KwanPas encore d'évaluation
- Case Report Form For HFMDDocument2 pagesCase Report Form For HFMDMendez RhuPas encore d'évaluation
- CRF HFMD AsmghDocument2 pagesCRF HFMD AsmghRyeowook RyePas encore d'évaluation
- D ReportDocument2 pagesD ReportHihiPas encore d'évaluation
- COVID-19 Vaccine Consent FormDocument2 pagesCOVID-19 Vaccine Consent FormApurva PathakPas encore d'évaluation
- Confidential Report On Adverse Drug Experience: (Mmm/dd/yyyy)Document1 pageConfidential Report On Adverse Drug Experience: (Mmm/dd/yyyy)Jorge ReyesPas encore d'évaluation
- Medication Error Reporting Form Pindaan 2Document2 pagesMedication Error Reporting Form Pindaan 2hanselMD100% (2)
- Aefi CifDocument4 pagesAefi CifVic KwanPas encore d'évaluation
- How To Fill ADR Reporitng Form and Causality AssessmentDocument38 pagesHow To Fill ADR Reporitng Form and Causality AssessmentVishal AryaPas encore d'évaluation
- Report of Suspected Adverse Drug Reactions: It's Easy To Report Online: Mhra - Gov.uk/yellowcard or Via The AppDocument2 pagesReport of Suspected Adverse Drug Reactions: It's Easy To Report Online: Mhra - Gov.uk/yellowcard or Via The AppGeorgia KavakopoulouPas encore d'évaluation
- FEMALE HPV 9 14 Years OldDocument1 pageFEMALE HPV 9 14 Years OldMA CARLA DIANNE PARABA. ESPINOSAPas encore d'évaluation
- Report On Suspected Adverse Drug ReactionsDocument2 pagesReport On Suspected Adverse Drug Reactionsyw100% (1)
- Approved ADR FormatDocument3 pagesApproved ADR Formatinayat.kabirPas encore d'évaluation
- Medical History FormDocument5 pagesMedical History FormgaloperiscolPas encore d'évaluation
- Drug Study Format For RLEDocument1 pageDrug Study Format For RLEAltroy Van AgtangPas encore d'évaluation
- Surgical Safety ChecklistDocument1 pageSurgical Safety ChecklistАндрій ДанильцівPas encore d'évaluation
- Suspected Side Effects Reporting Form v6.0Document2 pagesSuspected Side Effects Reporting Form v6.0TRIPLE 888Pas encore d'évaluation
- Borang Rabies - Sijil Vaksin RabiesDocument2 pagesBorang Rabies - Sijil Vaksin Rabiesleo89azmanPas encore d'évaluation
- Medication Error Reporting FormDocument2 pagesMedication Error Reporting Formahmad ganiePas encore d'évaluation
- Cif Zika - 2016 PDFDocument3 pagesCif Zika - 2016 PDFNicholai CabadduPas encore d'évaluation
- Pre-Departure Medical ExaminationDocument7 pagesPre-Departure Medical Examinationrummaan17Pas encore d'évaluation
- Measles CIF 2014Document2 pagesMeasles CIF 2014RionaMarieMagbutayPas encore d'évaluation
- Group Medical Insurance Claim Form Section 2Document1 pageGroup Medical Insurance Claim Form Section 2Aditya SharmaPas encore d'évaluation
- Pharmacist Workup of Drug Therapy in Pharmaceutical Care: Problem Oriented Pharmacist RecordDocument20 pagesPharmacist Workup of Drug Therapy in Pharmaceutical Care: Problem Oriented Pharmacist RecordDzaky UlayyaPas encore d'évaluation
- General Adverse Event Report Form - 20 Jul 2015Document4 pagesGeneral Adverse Event Report Form - 20 Jul 2015Cristian SabaPas encore d'évaluation
- Case Investigation Forms - Pidsrmop3ed 1Document16 pagesCase Investigation Forms - Pidsrmop3ed 1RHU Dupax del Sur100% (3)
- Rational Drug Use (Rdu) - Clin Pharma - IDocument3 pagesRational Drug Use (Rdu) - Clin Pharma - IKandysse de OcampoPas encore d'évaluation
- COVID-19 Vaccination Consent Form: Basic Info: First Tell Us Who You AreDocument2 pagesCOVID-19 Vaccination Consent Form: Basic Info: First Tell Us Who You AreVAS skytelPas encore d'évaluation
- Informed Consent UniversalDocument1 pageInformed Consent Universalahasgahsg031Pas encore d'évaluation
- UCU Ymana, Majesty Ann ADRDocument1 pageUCU Ymana, Majesty Ann ADRMajesty YmanaPas encore d'évaluation
- KipiDocument1 pageKipiHeRha DAniarPas encore d'évaluation
- Personal Accident'S / Accident Medical Reimbursement'S Attending Physician'S StatementDocument4 pagesPersonal Accident'S / Accident Medical Reimbursement'S Attending Physician'S Statementts8166Pas encore d'évaluation
- Village Medical Manual 7th Edition: A Guide to Health Care in Developing Countries (Combined Volumes 1 and 2)D'EverandVillage Medical Manual 7th Edition: A Guide to Health Care in Developing Countries (Combined Volumes 1 and 2)Pas encore d'évaluation
- Case Studies in Modern Drug Discovery and DevelopmentD'EverandCase Studies in Modern Drug Discovery and DevelopmentXianhai HuangPas encore d'évaluation
- Try VAERS: People are not reporting side effects from VaccinesD'EverandTry VAERS: People are not reporting side effects from VaccinesPas encore d'évaluation
- Good Health in the Tropics: Advice to Travellers and SettlersD'EverandGood Health in the Tropics: Advice to Travellers and SettlersPas encore d'évaluation
- Appendix - 5 (Under The Bye-Law No. 19 (B) )Document3 pagesAppendix - 5 (Under The Bye-Law No. 19 (B) )jytj1Pas encore d'évaluation
- CIR Vs PAL - ConstructionDocument8 pagesCIR Vs PAL - ConstructionEvan NervezaPas encore d'évaluation
- Hotel Reservation SystemDocument36 pagesHotel Reservation SystemSowmi DaaluPas encore d'évaluation
- BSCSE at UIUDocument110 pagesBSCSE at UIUshamir mahmudPas encore d'évaluation
- PFI High Flow Series Single Cartridge Filter Housing For CleaningDocument2 pagesPFI High Flow Series Single Cartridge Filter Housing For Cleaningbennypartono407Pas encore d'évaluation
- ARUP Project UpdateDocument5 pagesARUP Project UpdateMark Erwin SalduaPas encore d'évaluation
- Aluminum 3003-H112: Metal Nonferrous Metal Aluminum Alloy 3000 Series Aluminum AlloyDocument2 pagesAluminum 3003-H112: Metal Nonferrous Metal Aluminum Alloy 3000 Series Aluminum AlloyJoachim MausolfPas encore d'évaluation
- Cancellation of Deed of Conditional SalDocument5 pagesCancellation of Deed of Conditional SalJohn RositoPas encore d'évaluation
- United Nations Economic and Social CouncilDocument3 pagesUnited Nations Economic and Social CouncilLuke SmithPas encore d'évaluation
- Final ExamSOMFinal 2016 FinalDocument11 pagesFinal ExamSOMFinal 2016 Finalkhalil alhatabPas encore d'évaluation
- Heavy LiftDocument4 pagesHeavy Liftmaersk01Pas encore d'évaluation
- TLE - IA - Carpentry Grades 7-10 CG 04.06.2014Document14 pagesTLE - IA - Carpentry Grades 7-10 CG 04.06.2014RickyJeciel100% (2)
- Chapter 5Document3 pagesChapter 5Showki WaniPas encore d'évaluation
- Analysis of Material Nonlinear Problems Using Pseudo-Elastic Finite Element MethodDocument5 pagesAnalysis of Material Nonlinear Problems Using Pseudo-Elastic Finite Element MethodleksremeshPas encore d'évaluation
- RevisionHistory APFIFF33 To V219Document12 pagesRevisionHistory APFIFF33 To V219younesPas encore d'évaluation
- 21st Bomber Command Tactical Mission Report 178, OcrDocument49 pages21st Bomber Command Tactical Mission Report 178, OcrJapanAirRaidsPas encore d'évaluation
- Enerparc - India - Company Profile - September 23Document15 pagesEnerparc - India - Company Profile - September 23AlokPas encore d'évaluation
- Urun Katalogu 4Document112 pagesUrun Katalogu 4Jose Luis AcevedoPas encore d'évaluation
- CNC USB English ManualDocument31 pagesCNC USB English ManualHarold Hernan MuñozPas encore d'évaluation
- Pneumatic Fly Ash Conveying0 PDFDocument1 pagePneumatic Fly Ash Conveying0 PDFnjc6151Pas encore d'évaluation
- 23 Things You Should Know About Excel Pivot Tables - Exceljet PDFDocument21 pages23 Things You Should Know About Excel Pivot Tables - Exceljet PDFRishavKrishna0% (1)
- Saet Work AnsDocument5 pagesSaet Work AnsSeanLejeeBajan89% (27)
- Electrical ConnectorsDocument5 pagesElectrical ConnectorsRodrigo SantibañezPas encore d'évaluation
- Check Fraud Running Rampant in 2023 Insights ArticleDocument4 pagesCheck Fraud Running Rampant in 2023 Insights ArticleJames Brown bitchPas encore d'évaluation
- Online EarningsDocument3 pagesOnline EarningsafzalalibahttiPas encore d'évaluation
- CSEC Jan 2011 Paper 1Document8 pagesCSEC Jan 2011 Paper 1R.D. KhanPas encore d'évaluation
- Pindyck TestBank 7eDocument17 pagesPindyck TestBank 7eVictor Firmana100% (5)
- Banjara EmbroideryDocument34 pagesBanjara EmbroideryKriti Rama ManiPas encore d'évaluation
- Loading N Unloading of Tanker PDFDocument36 pagesLoading N Unloading of Tanker PDFKirtishbose ChowdhuryPas encore d'évaluation
- Algorithmique Et Programmation en C: Cours Avec 200 Exercices CorrigésDocument298 pagesAlgorithmique Et Programmation en C: Cours Avec 200 Exercices CorrigésSerges KeouPas encore d'évaluation