Vous aimerez peut-être aussi
- Antimicrobial Susceptibility TestingDocument7 pagesAntimicrobial Susceptibility TestingDarla YsavelPas encore d'évaluation
- Medical Microbiology Review of Antimicrobial Susceptibility TestingDocument7 pagesMedical Microbiology Review of Antimicrobial Susceptibility TestingTheresia Abigail JunitaPas encore d'évaluation
- Other CategoriesDocument10 pagesOther Categoriesnosila_oz854Pas encore d'évaluation
- 2009-Antimicrobial SusceptilityDocument7 pages2009-Antimicrobial SusceptilityStephanie MurillejoPas encore d'évaluation
- Anti Micro Biii AlDocument7 pagesAnti Micro Biii AltimiiniyiiPas encore d'évaluation
- Antimicrobial Susceptibility Testing: A Review of General Principles and Contemporary PracticesDocument7 pagesAntimicrobial Susceptibility Testing: A Review of General Principles and Contemporary Practicesabhishek yadavPas encore d'évaluation
- What's New in Antimicrobial Susceptibility Testing?: Dilution MIC Test Broth DilutionDocument3 pagesWhat's New in Antimicrobial Susceptibility Testing?: Dilution MIC Test Broth DilutionViswanathan AnanthanarayananPas encore d'évaluation
- VPT 607 Veterinary Chemotherapy Lab ManualDocument26 pagesVPT 607 Veterinary Chemotherapy Lab ManualSunilPas encore d'évaluation
- Antibiotic Susceptibility Testing Methods ReviewDocument8 pagesAntibiotic Susceptibility Testing Methods ReviewAndriano Arie WibowoPas encore d'évaluation
- Kirby-Bauer Disk Diffusion Susceptibility TestDocument16 pagesKirby-Bauer Disk Diffusion Susceptibility TestValeria RivasPas encore d'évaluation
- Antibiotic Susceptibility TestsDocument18 pagesAntibiotic Susceptibility Testsمحمد رحيم حسن محمودPas encore d'évaluation
- Group 4 Antibiotic Sensitivity TestingDocument8 pagesGroup 4 Antibiotic Sensitivity TestingJe Michelle LoayonPas encore d'évaluation
- Antimicrobial Susceptibility Testing FK 2012Document32 pagesAntimicrobial Susceptibility Testing FK 2012Sheryl Elita100% (1)
- Examples of Antibiotic Sensitivity Testing Methods - Antimicrobial ResistanceDocument3 pagesExamples of Antibiotic Sensitivity Testing Methods - Antimicrobial ResistanceGuranda SilvianPas encore d'évaluation
- 6 Microbiological Assay of AntibioticDocument16 pages6 Microbiological Assay of AntibioticGaurav MudaduPas encore d'évaluation
- In Vitro vs In Vivo Antimicrobial ActivityDocument2 pagesIn Vitro vs In Vivo Antimicrobial ActivityDebbyNovriozaPas encore d'évaluation
- Antimicrobial Susceptibility Testing - A Primer For Clinicians 2009 - ReadDocument18 pagesAntimicrobial Susceptibility Testing - A Primer For Clinicians 2009 - ReadJayelle2Pas encore d'évaluation
- Biological Testing of BiomaterialsDocument92 pagesBiological Testing of BiomaterialsShazia Rehman100% (1)
- Manual On Antimicrobial Susceptibility Testing Dr. M.K. LalithaDocument47 pagesManual On Antimicrobial Susceptibility Testing Dr. M.K. LalithaAntoniuz Liem100% (2)
- Antimicrobial Susceptibility Testing - Primer For CliniciansDocument20 pagesAntimicrobial Susceptibility Testing - Primer For Cliniciansdipzhit100% (1)
- Kirby-Bauer Disk Diffusion Susceptibility Test ProtocolDocument14 pagesKirby-Bauer Disk Diffusion Susceptibility Test ProtocolmauryaajitPas encore d'évaluation
- LAB 9 Antibiotics Susceptibility Tests 2nd 2020-2021Document14 pagesLAB 9 Antibiotics Susceptibility Tests 2nd 2020-2021Deena Hajj QasemPas encore d'évaluation
- Microbial Assay MethodsDocument34 pagesMicrobial Assay Methodspradeepbawane60% (5)
- Bacteriology: Principles of Antimicrobial ActionDocument35 pagesBacteriology: Principles of Antimicrobial ActionggemalynPas encore d'évaluation
- Inoculation Methods: Microbiological Challenge Testing of FoodsDocument14 pagesInoculation Methods: Microbiological Challenge Testing of FoodsBayu NugrahaPas encore d'évaluation
- Antibiotic Susceptibility TestingDocument12 pagesAntibiotic Susceptibility TestingOsama BakheetPas encore d'évaluation
- Antibac Ter Ia L Susceptibilit y Testing in The Clinic Al LaboratoryDocument34 pagesAntibac Ter Ia L Susceptibilit y Testing in The Clinic Al LaboratoryAnonymous hZYenTaXPas encore d'évaluation
- Antimicrobial Susceptibility TestingDocument6 pagesAntimicrobial Susceptibility TestingChelzea Jane EhurangoPas encore d'évaluation
- Current Technologies in Antimicrobial Susceptibility Testing and Microbial Identification:-Advantages, Limitations/challenges & Future PerspectiveDocument21 pagesCurrent Technologies in Antimicrobial Susceptibility Testing and Microbial Identification:-Advantages, Limitations/challenges & Future Perspectivebonsa dadhiPas encore d'évaluation
- A Practical Guide To ISO 10993-5 - Cytotoxicity - MDDI Medical Device and Diagnostic Industry News Products and SuppliersDocument4 pagesA Practical Guide To ISO 10993-5 - Cytotoxicity - MDDI Medical Device and Diagnostic Industry News Products and SuppliersVanessa DuzPas encore d'évaluation
- The Use of Microbiological Culture Media ArticleDocument9 pagesThe Use of Microbiological Culture Media ArticleTim Sandle100% (3)
- AmikacinDocument2 pagesAmikacinnajwa zinaouiPas encore d'évaluation
- Ampicillin 30 μg Disc Susceptibility TestingDocument2 pagesAmpicillin 30 μg Disc Susceptibility TestingKATHEPas encore d'évaluation
- Medical Microbiology: Class: 2Document3 pagesMedical Microbiology: Class: 2S APas encore d'évaluation
- Mic, MBC and Mic Cutoff ValueDocument23 pagesMic, MBC and Mic Cutoff ValueDiksha DahalPas encore d'évaluation
- Experiment 8 Determination of Antimicrobial ActivityDocument6 pagesExperiment 8 Determination of Antimicrobial ActivityAli Imran Mohamad100% (1)
- Antimicrobial Susceptibility Testing Paradigms Current Status and Future DirectionsDocument22 pagesAntimicrobial Susceptibility Testing Paradigms Current Status and Future DirectionsrehanaPas encore d'évaluation
- Micro-Mechanisms of Antimicrobial ResistanceDocument29 pagesMicro-Mechanisms of Antimicrobial ResistanceNOR UMAIRA BINTI ABU ASAN / IBSPas encore d'évaluation
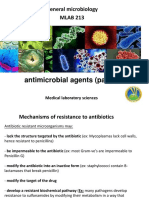
- Antimicrobial Agents (Part 2) : General Microbiology MLAB 213Document63 pagesAntimicrobial Agents (Part 2) : General Microbiology MLAB 213Norman Damaa100% (1)
- Broth and AgarDocument1 pageBroth and AgarVarghesePas encore d'évaluation
- Anti Microbial Chemotherapy: Dr. Ashish Jawarkar M.D. Consultant Pathologist Parul Sevashram HospitalDocument41 pagesAnti Microbial Chemotherapy: Dr. Ashish Jawarkar M.D. Consultant Pathologist Parul Sevashram HospitalDr. Ashish JawarkarPas encore d'évaluation
- The Definitions Given Below Have Been Selected and Restricted To Those That Are Likely To Be Useful To Users of This OIE Terrestrial ManualDocument7 pagesThe Definitions Given Below Have Been Selected and Restricted To Those That Are Likely To Be Useful To Users of This OIE Terrestrial ManualWormInchPas encore d'évaluation
- Tmp5a61 TMPDocument8 pagesTmp5a61 TMPFrontiersPas encore d'évaluation
- Validation of Microbial Recovery From Pharmacopeial Articles EpaDocument10 pagesValidation of Microbial Recovery From Pharmacopeial Articles EpaMarco HernandezPas encore d'évaluation
- EUCAST E Def 7.3.2 Yeast Testing Definitive Revised 2020Document21 pagesEUCAST E Def 7.3.2 Yeast Testing Definitive Revised 2020Guneyden GuneydenPas encore d'évaluation
- Lab Report Antimicrobial Susceptibility Testing MethodsDocument19 pagesLab Report Antimicrobial Susceptibility Testing MethodsAlyaa Athira100% (1)
- The Roles and FunctionsDocument2 pagesThe Roles and Functionssyed hafizPas encore d'évaluation
- 0052-0054 (51) Antimicrobial Effectiveness TestingDocument4 pages0052-0054 (51) Antimicrobial Effectiveness TestingDr usama El ShafeyPas encore d'évaluation
- Learning Objective 7Document14 pagesLearning Objective 7Ade Satria ApriadiPas encore d'évaluation
- EUCAST E.def 7.4 Yeast Definitive Revised 2023Document24 pagesEUCAST E.def 7.4 Yeast Definitive Revised 2023microbehunter007Pas encore d'évaluation
- LABORATORIODocument11 pagesLABORATORIOJonathan Junior C' ValverdePas encore d'évaluation
- Antibiotics TestDocument1 pageAntibiotics Testنوف الحربي.Pas encore d'évaluation
- Blog CCase Study of A New Growth-Based Rapid Microbiological Method That Detects The Presence of Specific Organisms and Provides An Estimation of Viable Cell Counthapter 2013Document3 pagesBlog CCase Study of A New Growth-Based Rapid Microbiological Method That Detects The Presence of Specific Organisms and Provides An Estimation of Viable Cell Counthapter 2013Annabel ElizabethPas encore d'évaluation
- Functionalized Nanomaterials for the Management of Microbial Infection: A Strategy to Address Microbial Drug ResistanceD'EverandFunctionalized Nanomaterials for the Management of Microbial Infection: A Strategy to Address Microbial Drug ResistanceRabah BoukherroubPas encore d'évaluation
- Parenteral Products: The Preparation and Quality Control of Products for InjectionD'EverandParenteral Products: The Preparation and Quality Control of Products for InjectionPas encore d'évaluation
- Environmental Immunochemical Analysis Detection of Pesticides and Other Chemicals: A User's GuideD'EverandEnvironmental Immunochemical Analysis Detection of Pesticides and Other Chemicals: A User's GuidePas encore d'évaluation
- ODE/PDE Analysis of Antibiotic/Antimicrobial Resistance: Programming in RD'EverandODE/PDE Analysis of Antibiotic/Antimicrobial Resistance: Programming in RPas encore d'évaluation
- Immunotherapy in Resistant Cancer: From the Lab Bench Work to Its Clinical PerspectivesD'EverandImmunotherapy in Resistant Cancer: From the Lab Bench Work to Its Clinical PerspectivesJorge Morales-MontorPas encore d'évaluation
- Antimicrobial Therapy in Veterinary MedicineD'EverandAntimicrobial Therapy in Veterinary MedicineSteeve GiguèreÉvaluation : 4 sur 5 étoiles4/5 (1)
- Microbiology and Parasitology PLE 2020 Answer PDFDocument15 pagesMicrobiology and Parasitology PLE 2020 Answer PDFMark Angelo Ponferrado100% (3)
- Microbiological Assay of AntibioticsDocument12 pagesMicrobiological Assay of AntibioticsIsmailPas encore d'évaluation
- Predictive Microbiology: Modeling Microbial Responses in FoodDocument11 pagesPredictive Microbiology: Modeling Microbial Responses in FoodHenock W. WoldemariamPas encore d'évaluation
- Dengue Bukhar Ka Ilaj Lakshan Karan Bachne Ke Upay in HindiDocument2 pagesDengue Bukhar Ka Ilaj Lakshan Karan Bachne Ke Upay in HindiSumit upayPas encore d'évaluation
- BorreliaDocument17 pagesBorreliaLin Sison Vitug100% (1)
- Sains T5Document141 pagesSains T5ZAINURRASHID BIN JUKI SGMPas encore d'évaluation
- (Tropical Medicine Science and Practice) (2008) PDFDocument506 pages(Tropical Medicine Science and Practice) (2008) PDFmilaPas encore d'évaluation
- Bacterial InfectionsDocument416 pagesBacterial Infectionsnihan tanerPas encore d'évaluation
- Dengue FeverDocument7 pagesDengue FeverTabarak BhuiyanPas encore d'évaluation
- Protect Against SalmonellaDocument8 pagesProtect Against SalmonellaUmi NurherawatiPas encore d'évaluation
- Flowcharts For Management of STI-FinalDocument22 pagesFlowcharts For Management of STI-FinalJay PaulPas encore d'évaluation
- Fusobacterium NecrophorumDocument8 pagesFusobacterium NecrophorumdavidPas encore d'évaluation
- Mutant Variations and the Danger of LockdownsDocument6 pagesMutant Variations and the Danger of LockdownsjrvvfPas encore d'évaluation
- ShigellosisDocument39 pagesShigellosisWai Kwong ChiuPas encore d'évaluation
- Submerged Culture of The Mycelium of Various Species of MushroomDocument3 pagesSubmerged Culture of The Mycelium of Various Species of Mushroombravohr98Pas encore d'évaluation
- USP 43 General Chapter 60Document3 pagesUSP 43 General Chapter 60Chetalee NaikPas encore d'évaluation
- SHC ABX Dosing GuideDocument6 pagesSHC ABX Dosing GuideAndreea SasuPas encore d'évaluation
- Traditional Starter Cultures in CheesethDocument88 pagesTraditional Starter Cultures in CheesethCAPRINOS BAJA CALIFORNIA SUR, MEXICO100% (1)
- Pediatric Vaccine Àd Vaccination PDFDocument257 pagesPediatric Vaccine Àd Vaccination PDFntnquynhpro100% (1)
- 03 Biosecurity Jit PPT FinalDocument20 pages03 Biosecurity Jit PPT FinalReza WratsongkoPas encore d'évaluation
- 1731-Article Text-11756-2-10-20210224Document6 pages1731-Article Text-11756-2-10-20210224Nurul izzahPas encore d'évaluation
- 1stinternational Congress On Food TechnologyDocument571 pages1stinternational Congress On Food TechnologyPat ChuthamasPas encore d'évaluation
- MPN Table ExplainedDocument44 pagesMPN Table ExplainedDzulfathil PuteraPas encore d'évaluation
- Bahan Kuliah HIV-AIDSDocument17 pagesBahan Kuliah HIV-AIDSKiki Rizky Andani NasutionPas encore d'évaluation
- Mojbm 03 00082Document5 pagesMojbm 03 00082Sohrab RohanePas encore d'évaluation
- Microbiology PPSCDocument4 pagesMicrobiology PPSCAmmara ZulqarnainPas encore d'évaluation
- NBDE 1: Exam 7 (Micro) : Study Online atDocument4 pagesNBDE 1: Exam 7 (Micro) : Study Online atParneetPas encore d'évaluation
- Biology 9th Solving A Biological ProblemDocument5 pagesBiology 9th Solving A Biological Problemmhussainshigri786Pas encore d'évaluation
- Infection and Host ResistanceDocument62 pagesInfection and Host ResistanceAndrea Marie T. Artajo-BoheromPas encore d'évaluation
- Typhoid FeverDocument52 pagesTyphoid Fevertummalapalli venkateswara rao100% (5)