Vous aimerez peut-être aussi
- Malignant Tumors of The Facial SkinDocument78 pagesMalignant Tumors of The Facial SkinMladen PazinPas encore d'évaluation
- 10 - Oralcavity TumorsDocument28 pages10 - Oralcavity Tumorsibrahim100% (1)
- Oral Squamous Cell CarcinomaDocument31 pagesOral Squamous Cell CarcinomaAli RahimiPas encore d'évaluation
- Head and Neck SurgeryDocument58 pagesHead and Neck SurgeryselamuPas encore d'évaluation
- Oral Potentially Malignant DisordersDocument11 pagesOral Potentially Malignant DisordersRomario GintaPas encore d'évaluation
- Malignant Epithelial NeoplasmsDocument19 pagesMalignant Epithelial NeoplasmsAtef Mahmoud AhmedPas encore d'évaluation
- Oral SCCDocument10 pagesOral SCCيونس حسينPas encore d'évaluation
- Oral Cancer 26.3.19Document23 pagesOral Cancer 26.3.19Pradeep100% (2)
- Oral Cavity & OesophagousDocument44 pagesOral Cavity & OesophagousrashmiPas encore d'évaluation
- Malignant Epithelial Non-Odontogenic Tumors 2Document11 pagesMalignant Epithelial Non-Odontogenic Tumors 2samamustafa.2003Pas encore d'évaluation
- Salivary 020Document74 pagesSalivary 020Dirga Rasyidin LPas encore d'évaluation
- 01 Oral Cavity PDFDocument106 pages01 Oral Cavity PDFGhaydaa Abukhairan0% (1)
- Nada's GI Path ReviewDocument44 pagesNada's GI Path ReviewNada Much100% (2)
- SCC Tongue Anatomy and OthersDocument21 pagesSCC Tongue Anatomy and OthersEunice RiveraPas encore d'évaluation
- Salivary Gland Neoplasms: Elizabeth J. Rosen, MD Shawn D. Newlands, MD, PHD 6/26/02Document74 pagesSalivary Gland Neoplasms: Elizabeth J. Rosen, MD Shawn D. Newlands, MD, PHD 6/26/02junaid34Pas encore d'évaluation
- Tumors of Salivary GlandDocument28 pagesTumors of Salivary Glandrameshparajuli14100% (1)
- Benign and Malignant Tumors of Oral CavityDocument56 pagesBenign and Malignant Tumors of Oral CavityPawan Kumar83% (6)
- Head and Neck LesionsDocument131 pagesHead and Neck Lesionslunaghilvin2026Pas encore d'évaluation
- Squamous Cell CarcinomaDocument19 pagesSquamous Cell CarcinomaPradeepPas encore d'évaluation
- Nasal TumorDocument20 pagesNasal TumorMahmoud ElsherbenyPas encore d'évaluation
- Oral Squamous Cell Carcinoma (OSCC)Document37 pagesOral Squamous Cell Carcinoma (OSCC)Yusra Shaukat100% (1)
- Melanoma: Edward Buckingham, M.D. Combined Plastics Conference September 6, 2000Document53 pagesMelanoma: Edward Buckingham, M.D. Combined Plastics Conference September 6, 2000Kadek Ariarta MahartamaPas encore d'évaluation
- Salivary Gland Tumors: 1. AdenomasDocument18 pagesSalivary Gland Tumors: 1. AdenomasMahammed Ahmed BadrPas encore d'évaluation
- Chapter 16 - Head and NeckDocument8 pagesChapter 16 - Head and NeckAgnieszka WisniewskaPas encore d'évaluation
- Oral PathologyDocument31 pagesOral PathologyAnonymous GyqTkXMwMPas encore d'évaluation
- Intraoral Benign TumorsDocument4 pagesIntraoral Benign TumorsSaman SadeghiPas encore d'évaluation
- Head and Nexck - PPTXDocument80 pagesHead and Nexck - PPTXVijay SudhaPas encore d'évaluation
- Oral Cancer MADE EASYDocument19 pagesOral Cancer MADE EASYMohammedPas encore d'évaluation
- Tongue Ulcers, Tumors of The Tongue and Lip, RanulaDocument26 pagesTongue Ulcers, Tumors of The Tongue and Lip, Ranulamhmdalbdyny764Pas encore d'évaluation
- Tumors: of The Nose, Sinuses and NasopharynxDocument69 pagesTumors: of The Nose, Sinuses and Nasopharynxapi-19770621Pas encore d'évaluation
- Sunarto-Head & Neck Cancer DiagnosisDocument40 pagesSunarto-Head & Neck Cancer DiagnosisnurwntPas encore d'évaluation
- Oral PathologyDocument31 pagesOral PathologyAnasthasia hutagalungPas encore d'évaluation
- Blok Spesial Sense NewDocument34 pagesBlok Spesial Sense NewYola SurbaktiPas encore d'évaluation
- Oral Cavity - Pre Malig Lesions & SCCDocument25 pagesOral Cavity - Pre Malig Lesions & SCCDeepika LamichhanePas encore d'évaluation
- Cancer of LarynxDocument29 pagesCancer of LarynxQasim HaleimiPas encore d'évaluation
- Oral Potential Malignant DisorderDocument62 pagesOral Potential Malignant DisorderOmnia SamiPas encore d'évaluation
- Git 7 PDFDocument29 pagesGit 7 PDFafaq alismailiPas encore d'évaluation
- Skin MalignanciesDocument84 pagesSkin MalignanciesDrbarathirajaPas encore d'évaluation
- Genitourinary Tract Tumors Including Renal Tumors: Pre-ReadingDocument31 pagesGenitourinary Tract Tumors Including Renal Tumors: Pre-Readingmus zaharaPas encore d'évaluation
- Tumor Ganas Mata: Alfa SylvestrisDocument53 pagesTumor Ganas Mata: Alfa SylvestrisAzilu FalaPas encore d'évaluation
- Oral Pre Cancerous LesionsDocument49 pagesOral Pre Cancerous LesionsAmit MishraPas encore d'évaluation
- Surgical Management of Malignant TumorsDocument129 pagesSurgical Management of Malignant TumorsAshish JainPas encore d'évaluation
- $12. Urinary Tract Infections 2015Document39 pages$12. Urinary Tract Infections 2015Sindhu BabuPas encore d'évaluation
- Head and Neck PPT 2024Document65 pagesHead and Neck PPT 2024lallsPas encore d'évaluation
- 1.pathology-Practical - Disease Affecting Uper Respiratory TractDocument34 pages1.pathology-Practical - Disease Affecting Uper Respiratory TractSounds of MindPas encore d'évaluation
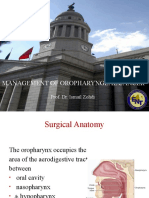
- Cancer OropharynxDocument108 pagesCancer OropharynxAshokPas encore d'évaluation
- 2 Nasopharyngeal Dise (Sept. 2019) - StudentDocument80 pages2 Nasopharyngeal Dise (Sept. 2019) - StudentNicPas encore d'évaluation
- Squamous Cell CarcinomaDocument53 pagesSquamous Cell CarcinomaWacky BlankPas encore d'évaluation
- Malignant Skin Tumors BNS 313 - 2023Document56 pagesMalignant Skin Tumors BNS 313 - 2023Kemo RakhoboPas encore d'évaluation
- Head and Neck Cancers-Predisposing Factors-Etiology-Premalign LesionsDocument41 pagesHead and Neck Cancers-Predisposing Factors-Etiology-Premalign Lesionspianistgirl99Pas encore d'évaluation
- Barr SCC FinalDocument10 pagesBarr SCC FinalSanchit MehanPas encore d'évaluation
- Dr. C.T. Karthikeyan, Associate Professor, Dept. of General SurgeryDocument40 pagesDr. C.T. Karthikeyan, Associate Professor, Dept. of General SurgeryNaveen RajeshwarPas encore d'évaluation
- SCC, Melanoma (Autosaved)Document26 pagesSCC, Melanoma (Autosaved)arun j.rPas encore d'évaluation
- Lung TumorsDocument27 pagesLung TumorsFangPas encore d'évaluation
- Oral Epithelial Tumors: Faleh SawairDocument52 pagesOral Epithelial Tumors: Faleh SawairHanin AbukhiaraPas encore d'évaluation
- Salivary GlandsDocument58 pagesSalivary GlandsApollo DentalPas encore d'évaluation
- Atlas of Diagnostically Challenging Melanocytic NeoplasmsD'EverandAtlas of Diagnostically Challenging Melanocytic NeoplasmsPas encore d'évaluation
- Salivary Gland Cancer: From Diagnosis to Tailored TreatmentD'EverandSalivary Gland Cancer: From Diagnosis to Tailored TreatmentLisa LicitraPas encore d'évaluation
- Tattoos Ink and CancerDocument9 pagesTattoos Ink and Cancereby_3tamaPas encore d'évaluation
- WHO Classification of Lung Cancer 2014Document79 pagesWHO Classification of Lung Cancer 2014dawwnPas encore d'évaluation
- Etiology of Oral Squamous Cell Carcinoma PDFDocument2 pagesEtiology of Oral Squamous Cell Carcinoma PDFChristopherballinPas encore d'évaluation
- Non Melanoma Skin CancerDocument66 pagesNon Melanoma Skin CancerSalmanArif0% (1)
- Histological and Molecular Aspects of Oral Squamous Cell Carcinoma (Review)Document5 pagesHistological and Molecular Aspects of Oral Squamous Cell Carcinoma (Review)Yeni PuspitasariPas encore d'évaluation
- Salvestrols Cures CancerDocument29 pagesSalvestrols Cures CancerJohn Tan100% (1)
- Third Eyelid Gland Neoplasms of Dogs and CatsDocument6 pagesThird Eyelid Gland Neoplasms of Dogs and CatsMicheleBerselliPas encore d'évaluation
- Nufd 488 - Cancer Case Study-7Document19 pagesNufd 488 - Cancer Case Study-7api-487121869Pas encore d'évaluation
- Dermatology GuideDocument89 pagesDermatology GuideZeljnaznanja100% (3)
- Administrarea Topica A Carmustinei in Micoza Fungoida. Eficacitate Si Efecte AdverseDocument1 pageAdministrarea Topica A Carmustinei in Micoza Fungoida. Eficacitate Si Efecte AdverseAlexandra MehedințPas encore d'évaluation
- Ojsadmin, 1340Document4 pagesOjsadmin, 1340Dr NisrinPas encore d'évaluation
- Vaginal CarcinomaDocument8 pagesVaginal CarcinomaMutiarawati MithrataelúwånzhùPas encore d'évaluation
- Derma PaperDocument5 pagesDerma PaperWacky BlankPas encore d'évaluation
- Penile Squamous Cell CarcinomaDocument64 pagesPenile Squamous Cell CarcinomaTres De GuzmanPas encore d'évaluation
- Well Differentiated Squamous Cell Carcinoma, Keratoacanthoma Type. Three Cases. DR Sarma's DermpathDocument17 pagesWell Differentiated Squamous Cell Carcinoma, Keratoacanthoma Type. Three Cases. DR Sarma's DermpathDeba P SarmaPas encore d'évaluation
- Restoration of Body Focussing On NumbersDocument95 pagesRestoration of Body Focussing On Numbersssss87va93% (27)
- Ooi 150050Document7 pagesOoi 150050MelaNia Elonk ZamroniPas encore d'évaluation
- Oral Squamous Cell CarcinomaDocument6 pagesOral Squamous Cell CarcinomaAndykaYayanSetiawan100% (2)
- Oral Potentially Malignant Disorders Healthcare Professional Training English Version - CompressedDocument120 pagesOral Potentially Malignant Disorders Healthcare Professional Training English Version - CompressedClaudio MaranhaoPas encore d'évaluation
- Case Ca Laring UMJDocument51 pagesCase Ca Laring UMJDera Seta SaputriPas encore d'évaluation
- 9781905635863Document18 pages9781905635863Peter Osundwa KitekiPas encore d'évaluation
- Cancer LaryncDocument35 pagesCancer LaryncSaya MenangPas encore d'évaluation
- CK 7 and CK 20 Positive Tumors Modern Pathol 2000Document11 pagesCK 7 and CK 20 Positive Tumors Modern Pathol 2000api-26176346Pas encore d'évaluation
- Malignant NeoplasmsDocument59 pagesMalignant NeoplasmsRosa Gusmi PutriPas encore d'évaluation
- Malignant Seborrheic Keratosis M 72Document3 pagesMalignant Seborrheic Keratosis M 72Deba P SarmaPas encore d'évaluation
- RTS2-K4-Pathology of Lung CancerDocument58 pagesRTS2-K4-Pathology of Lung CancerMarieta RitongaPas encore d'évaluation
- Qstream-1 2Document55 pagesQstream-1 2Vijay100% (1)
- Skin Tumor AgusDocument54 pagesSkin Tumor AgusHafida AuliaristaPas encore d'évaluation
- Essentials CompleteDocument66 pagesEssentials CompleteNovriman LiviaPas encore d'évaluation
- Cryo TherapyDocument8 pagesCryo TherapyAbhishek ChauhanPas encore d'évaluation