Académique Documents
Professionnel Documents
Culture Documents
Non Opioid Postoperative Analgesia
Transféré par
Gunther Dick MirandaDescription originale:
Copyright
Formats disponibles
Partager ce document
Partager ou intégrer le document
Avez-vous trouvé ce document utile ?
Ce contenu est-il inapproprié ?
Signaler ce documentDroits d'auteur :
Formats disponibles
Non Opioid Postoperative Analgesia
Transféré par
Gunther Dick MirandaDroits d'auteur :
Formats disponibles
Acta Anaesthesiol Scand 2000; 44: 11911203 Printed in Denmark.
All rights reserved
Copyright C Acta Anaesthesiol Scand 2000 ACTA ANAESTHESIOLOGICA SCANDINAVICA
ISSN 0001-5172
Review Article
Non-opioid postoperative analgesia
V. DAHL and J. C. RDER1
Departments of Anaesthesia, Brum Hospital and 1Ullevaal University Hospital, Oslo, Norway
Key words: Postoperative analgesia; review.
c Acta Anaesthesiologica Scandinavica 44 (2000)
drugs play an important part in the treatment of postoperative pain (1). Although opioids are highly efcacious, unwanted side-effects such as postoperative nausea and vomiting (PONV), drowsiness, respiratory depression, gastrointestinal and bladder dysfunction justify the search for alternative analgesics in the postoperative setting (2). During the last decades, a broader understanding of the pathophysiological mechanisms of tissue damage and postoperative pain has provided clinicians with a rationale for a balanced postoperative analgesia (3). Peripheral tissue damage and hyperalgesia are among many mechanisms responsible for the postoperative pain experience. The hypersensitisation of the dorsal horn of the spinal cord is probably of great clinical signicance (4). Although the blocking of wind-up is an intriguing phenomenon in animal models, the role of this pre-emptive analgesia is still unclear in the clinical eld (5). This paper is a review of the possible non-opioid pharmacological pain treatment modalities. The pathophysiology of postoperative pain will be reviewed, and different pharmacological approaches discussed.
ON-OPIOID
Pathophysiology of pain
A surgical procedure results in tissue damage and injury of small nerve bres. The afferent nociceptors (Amechanothermal and C-polymodal) are nerve endings in the periphery which normally have a high threshold for activation. Pain sensation may be produced by direct stimuli of these nerve endings, but the inammation due to a surgical procedure will produce a peripheral sensitisation enhancing the sensitivity of these nociceptors. Potassium, prostaglandins, bradykinins and other mediators from damaged cells trig-
ger the nociceptors to send afferent impulses via the dorsal root ganglion to the spinal cord (6). These nerves produce sensory neuropeptides, such as substance P, neurokinin A and calcium gene-related peptides. The neuropeptides will probably exert their effect both peripherally and centrally. In the periphery it will increase the excitability of sensory bres. Simultaneously, antidromic impulses will lead to a stimulation of adjacent sensory nerve bres. Increased release of catecholamines from sympathetic nerve bres will further sensitise the nociceptors, resulting in peripheral hyperalgesia (7, 8). Centrally, nociceptive transmission in the dorsal horn is enhanced. Nerve growth factor (NGF), or neurotrophin, is also released in the periphery during tissue damage. NGF may induce structural changes in the cell, thereby facilitating transport of peptides in the nerves. This will further enhance the excitability of the sensory neurones (9, 10). Repetitive transmission of nociceptive impulses into the dorsal horn will increase the glutamate-mediated transmission by upregulating the N-methyl-Daspartate (NMDA) receptor (11). The central sensitisation or wind-up phenomenon may partially be a result of a prolonged and enhanced production of nitric oxide (12). There is a complex system on many levels of compensatory neuroinhibitory mechanisms involved in the perception of pain. Opioid receptors are synthesised or upregulated in the sensory neurones both centrally and peripherally. Endogenous opioids binding to these receptors will reduce the excitability of afferent nerve bres. In the periphery, during inammation, immunocompetent cells seem to produce opioid peptides (13). Centrally the opioid receptors will act as presynaptic receptors. In the dorsal horn, interneurons will release opioid peptides, thereby inhibiting pain transmission (14). Furthermore, there are
1191
V. Dahl and J. C. Rder
inhibitory mechanisms higher up in the central nervous system. From well-dened areas in the medulla oblongata and mesencephalon inhibiting serotonergic and noradrenergic pathways will reduce pain transmission in the dorsal horn (15, 16).
Classication of analgesic drugs
Analgesic drugs may be divided into opioid and nonopioid drugs. The opioid drug class encompasses all natural and synthetic drugs which have stereospecic effects on well-dened, membrane-bound opioid receptors. These receptors belong to a superfamily of Gprotein-coupled receptors. Molecular cloning has led to the identication of three different types of opioid receptors, OP1 (d), OP2 (k) and OP3 (m), thereby conrming previous postulates of their existence (17). Recently, a fourth opioid receptor (OP4) and its pronociceptive ligand nociceptin have been identied (18). The different opioid drugs effects are dependent on their afnity to the different receptors, and whether they act as agonists (like morphine), antagonists (like naloxone) or mixed agonists/antagonists (like buprenorphine). The non-opioid analgesic drugs can be subdivided into specic and non-specic analgesics. The specic drugs are the commonly used analgesics for mild and moderate pain like the non-steroidal anti-inammatory drugs (NSAIDs), paracetamol (acetaminophen) and acetylacetic acid. The non-specic analgesics group contains all other drugs that are commonly used for other purposes but which have analgesic properties. Examples from this group are the NMDAreceptor antagonist ketamine, the a2-receptor agonists and the tricyclic antidepressant amitriptyline.
nation of several analgesic regimens like NSAIDs, local anaesthesia and other analgesics offers a means to improve postoperative pain relief and minimise sideeffects. As proposed by Miniche et al. (22), the painfree patient will enable an aggressive mobilisation and early rehabilitation after surgery, thus reducing postoperative complications such as deep venous thrombosis and pulmonary dysfunction. Early oral feeding will reduce protein waste. Not only will a multimodal approach give more satised patients, it has also been shown to reduce the length of postoperative stay and accelerate the time to hospital discharge (22). Pre-emptive analgesia refers to the theory that analgesia given before the tissue injury may block the development of neuronal hyperexitability in the central nervous system. If the same analgesic treatment is given after the injury, it will have less effect (4). Although experimental data support this theory (23), results from clinical studies are less encouraging (24, 25). In a surgical setting, the input of afferent neuronal activity into the spinal horn will be present not only during surgery but also for some time afterwards due to the continuation of the inammatory response at the site of the injury. A once-only dose of pre-emptive treatment with a single drug may fail to have effect because of insufcient or too short-lasting effect on blocking the pain stimuli into the spinal cord (26).
Local anaesthesia
Local anaesthesia is an efcient non-opioid pharmacological approach to postoperative analgesia. Local anaesthesia is used both for neural blockade and for inltration. The use of neuronal blockade for surgery is effective for postoperative pain and has an opioidsparing effect (27). Different inltration techniques have been shown to be pain reducing and opioid sparing after cholecystectomy (28), inguinal hernia repair (29), breast surgery (30), gynaecological laparotomies (31), orthopaedic (32) and anorectal (33) surgery. A recent study has also shown benecial effect from inltration of local anaesthesia in the trocar entrances after laparoscopic procedures (34). Instillation of local anaesthesia without inltrating has also been proven efcacious. Topical analgesia with lidocaine aerosol was found to be highly effective after inguinal herniorraphy (35), and instillation of bupivacaine with epinephrine or lidocaine during laparoscopy reduces postoperative scapular pain (36). Topical administration of local anaesthesia has excellent analgesic properties after ambulatory circumcision in children (37). In addition to the traditional effects of local anaesthesia, the amide local anaesthetics seem to
Principles of postoperative analgesia: What are the issues?
Although opioids still remain important drugs for severe postoperative pain, their use in postoperative pain treatment has severe limitations. Modern postoperative treatment focuses on early mobilisation and rapid discharge of patients following surgery (19). Opioid-based analgesia has side-effects such as drowsiness, respiratory depression, PONV and gastrointestinal and bladder dysfunction, which will restrict the patient from mobilisation and discharge (20). It is also clear that patients given opioids after major surgery experience less analgesic effect during movement, thus restricting them further from early mobilisation (21). The concept of balanced or multimodal analgesia has evolved rapidly during recent years. The combi-
1192
Non-opioid postoperative analgesia
have a long-lasting anti-inammatory effect, thereby blocking the postoperative inammatory process on the surgical site (38, 39). Although the benets are evident, more studies are needed to evaluate optimal methods for inltration and topical administration (40). There is also a lack of clinical studies investigating different techniques of wound inltration with combinations of other pharmacological agents and analgesic methods (41). Difculties in inltrating all relevant structures, especially after major surgery, limits the efcacy of wound inltration. The short duration of the different local anaesthetic agents is also limiting. An ideal local anaesthetic drug in the postoperative setting would be one providing ultra-long analgesia. There are promising results from animal studies showing that the duration of an anaesthetic block can be considerably prolonged by increasing the viscosity of the local anaesthetic (42). Encapsulation in liposomes prolongs the duration of the local anaesthetics in animal models (43). Another interesting eld of research is the inclusion of local anaesthesia in monoolein water systems. This technique uses the monoolein water system to give a product which is liquid at room temperature and highly viscous at body temperature, thus providing an easily injectable slow-release system (44).
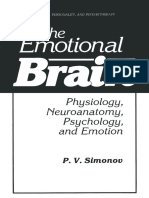
Fig. 1. Arachidonic acid cascade.
Non-steroidal anti-inammatory drugs
The arachidonic acid cascade system is the most important phospholipid derived messenger system and plays a key regulatory role in cell physiology. Oxidation of arachidonic acid via the cyclo-oxygenase (COX) pathway generates a series of prostaglandins and thromboxanes, many of which play a substantial role in the perception of pain. Prostaglandins and thromboxanes are generated by tissue trauma and mediate nociception by sensitisation of peripheral nociceptors in synergy with other chemical mediators. NSAIDs block the synthesis of prostaglandins by inhibition of the enzyme cyclo-oxygenase (45, 46, Fig. 1). However, NSAIDs also have prostaglandin-independent effects in the periphery (47, 48), and recent research suggests that a substantial part of the analgesia provided by this group of drugs is centrally mediated (49). NSAIDs are well-known drugs with analgesic and opioid-sparing effects (50). They are highly efcacious in the treatment of postoperative pain after orthopaedic and major gynaecological surgery (51, 52). For certain types of pain with little opioid sensitivity, such as pain from bone metastasis, gall bladder and urinary spasm pain, NSAIDs are particularly benecial (53). The injectable forms of NSAIDs, such as ketorol-
ac, ketoprofen and diclofenac, enable possibilities of perioperative analgesia without the many side-effects of opioids. In children, NSAIDs have been successfully used for postoperative analgesia and other painful conditions such as acute otitis media (5456). However, the use of NSAIDs is limited by contraindications and potentially severe side-effects. Prostaglandin E2 and prostacyclin (PGI2) syntheses are essential for the production of the gastric mucosa protecting mucus, and gastrointestinal bleeding is a well known complication of NSAIDs (57). Renal impairment is another risk, especially in patients who are dependent on a high level of renal prostaglandins, such as elderly patients with arteriosclerosis, hypovolaemic patients and patients with known kidney failure and congestive heart failure. In large retrospective cohort studies, however, short-term use of NSAIDs ( 5 days) in patients under 75 years of age did not increase the incidence of renal failure or gastrointestinal bleeding (58, 59). Acute bronchospasm is also a potential side-effect of NSAIDs, and 820% of patients with asthma will experience bronchospasm after using NSAIDs (60). A major issue of controversy is the combination of NSAIDs and low-molecular weight heparins for venous thrombosis prophylaxis. Although NSAIDs antiplatelet effect is unlikely to produce perioperative bleeding complications by itself (61), there are some concerns about the combination (62). During the last years it has become evident that the cyclo-oxygenase enzyme exists as at least two different isoenzymes, the COX-1 and the COX-2 enzyme (63). The COX-1 isoenzyme is the constitutive form with physiologic functions in normal homeostasis,
1193
V. Dahl and J. C. Rder
while COX-2 is the inducible form. During inammation COX-2 is induced and upregulated, thereby producing high levels of prostanoids, whereas the COX-1 levels remain almost unaffected. There are, however, tissues such as the lungs, kidneys and neural tissue which have a high level of COX-2 even in the absence of external stimuli. NSAIDs with a high COX-2 specicity would theoretically have a benecial effect on inammation and pain perception without affecting the homeostatic functions of prostaglandins. Drugs with higher potency against COX-2 than COX-1 will produce fewer side-effects. The potency of NSAIDs against either enzyme can be expressed as the ratio of their respective IC50 and the COX-2/COX-1 ratios as shown in Table 1 (64). A ratio of 1 indicates a greater inhibition of COX-2 than COX-1 and thus less propensity to induce side-effects. Indeed, a drug with a high COX-1 afnity, such as piroxicam, induces more side-effects than the new drug meloxicam with a high COX-2 afnity (65). In the near future, more selective COX-2 inhibitors such as selecoxib and rofecoxib will probably bring pain relief with less toxicity (66). The development of prostanoid E1 selective receptor antagonists is another exiting development in the eld of analgesia by prostanoid inhibition. In spite of the potentially dangerous side-effects of NSAIDs, they are of great value in the perioperative period and are usually well tolerated as long as the drug is used in appropriate doses and contraindications are respected.
Paracetamol
Paracetamol is a well-established analgesic drug for the postoperative period, and is widely used as a basis for postoperative pain treatment. The need for opioid analgesia has typically been reduced by 20 30% when combined with a regular regimen of oral or rectal paracetamol. The evidence of a central com-
Table 1
Cyclo-oxygenase IC50 values (mmol/l) of NSAIDs in intact cells. NSAID Meloxicam Piroxicam Diclofenac Indomethacin Naproxen Ibuprofen Paracetamol Aspirin COX-2 0.171 0.604 1.1 1.68 5.65 72.8 133 278 COX-1 0.214 0.002 1.57 0.028 9.56 4.85 17.9 1.67 COX-2/COX-1 RATIO 0.8 250 0.7 60 0.6 15 7.4 166
Adapted from: Camu F (64).
ponent to its action and the fact that paracetamol easily crosses the bloodbrain barrier makes this drug even more interesting (67, 68). Paracetamol, given as a single dose of 1000 mg, has a number-needed-totreat (NNT) of 3.6, which is better than for instance tramadol 100 mg or the combination of acetylacetic acid 650 mg and codeine 60 mg (69). In comparison with clinical doses of NSAIDs it is probably of less analgesic potency, but seems to have an additional analgesic effect when given in combination (70, 71). For instance, the combination of diclofenac and paracetamol for postoperative pain after oral surgery enhances and prolongs the analgesic effect compared to either of the two drugs used alone (72). Studies on children indicate that paracetamol has good analgesic properties when serum levels of 1020 mg/l are achieved, and this level can be reached with a dosage of 40 mg/kg orally (73). The use of rectal administration for children is widely used, but the recommended dosage of 20 mg/kg is probably insufcient. Studies have shown a dose/response analgesic efcacy in the postoperative paediatric patient up to a single dose of 60 mg/kg without any side-effects (74). Bremerich et al. have measured the mean paracetamol concentration after rectal administration to 3.5 mg/l after 20 mg/kg and 6.2 mg/l after 40 mg/kg, with poor analgesic effect in the postoperative period (75). When compared with oral paracetamol, rectal administration has a somewhat slower onset with a maximum serum concentration at 22.5 h as compared to 0.6 h for tablets, and a lower peak serum level (76). This should be taken into consideration when suppositories are used for postoperative pain treatment. Clearly, a single rectal dose of 4060 mg/kg paracetamol seems safe in children. If paracetamol is used rectally in adults, the dosage should probably exceed the peroral dosage by 50%. Recently, an intravenous precursor of paracetamol, propacetamol, has been developed. One gram of the precursor readily converts into 0.5 g paracetamol. Propacetamol has proven to be efcacious as postoperative analgesia. After orthopaedic surgery it has been demonstrated that propacetamol reduces the postoperative opioid requirement by 46% (77). There are concerns regarding the side-effects of paracetamol, such as a potential genotoxic effect (78) and renal toxicity, when used in combination with NSAIDs in vulnerable patients (79). Also, the therapeutic window of paracetamol is low, and even small amounts of paracetamol overdosage can result in liver damage (80). When used in analgesic doses, however, there is no evidence of genotoxicity (81). Paracetamol in combination with NSAIDs should, however, be
1194
Non-opioid postoperative analgesia
used with caution in patients requiring a high level of prostaglandins to maintain adequate renal perfusion, such as hypovolaemic patients and elderly patients with renal failure. When used alone, paracetamol is considered safe even in this group of patients. In summary, paracetamol is highly efcacious as a basic postoperative analgesic. Used in combination with a NSAID, paracetamol seems to give additional analgesia. The use of intravenous propacetamol will enable a more exible use of this drug in the postoperative setting.
NMDA-receptor antagonists
The NMDA receptor is a glutamate receptor characterised by afnity for N-methyl-D-aspartate. It has an allosteric binding site for the excitatory amino acid and a site within the channel itself to which magnesium ions bind in a voltage-dependent manner. The positive voltage dependence of channel conductance and the high permeability of the conducting channel to calcium ions are important in excitotoxicity and neuronal plasticity. Excitation of the NMDA-receptor system in the dorsal horn plays an important role in the sensitisation process (11, 82). The use of NMDAreceptor antagonists has been shown both to prevent and reverse hyperalgesia in animal studies (83). Lately, NMDA receptors have been located in the unmyelinated axons in the periphery, thus indicating that excitatory amino acids, in addition to their role in the central nervous system, may play a role in the primary nociception in the periphery (84). The glutamate excitatory transmitter system is widely spread in the central nervous system and is involved in many important physiological processes. NMDAreceptor antagonism will therefore be prone to lead to unwanted side-effects, thus limiting its use in clinical pain treatment. Ketamine, an anaesthetic agent well known for more than 30 years, has been shown to interact with a number of receptor systems such as the NMDA-receptor system, opioid receptors, monoaminergic receptors and muscarinic receptors (85). In low doses it may result in a selective, non-competitive NMDA blockade (86). Low doses of ketamine have in some studies been shown to have postoperative analgesic effect. Although most studies have focused on the use of ketamine as pre-emptive analgesia (87, 88), some studies also advocate its use postoperatively (89). There are, however, several studies that fail to show any effect of low-dose ketamine (90, 91), especially when applied preoperatively in small doses. The use of larger doses of ketamine in the postoperative period is limited by
its known psychomimetic side-effects. Analgesic concentrations of ketamine start at approximately 1200 ng/ml (92), whereas plasma concentrations of ketamine on awakening from general anaesthesia have been reported in the range of 61100 ng/ml. Psychedelic side-effects of ketamine are reported at plasma levels as low as 1200 ng/ml (93). Ketamine seems to have a potent analgesic effect on certain types of chronic pathologic pain conditions (94). Studies on human volunteers seem to indicate that ketamine exerts its primary blocking effects when the NMDA-receptor-controlled ion channel has already been opened by a continuous nociceptive stimulus (95). This could explain why ketamine is a poor analgesic when used pre-emptively or for acute pain, while it is highly efcacious for pathological pain conditions. Ketamine has also been used as an epidural or intrathecal drug for pain alleviation after surgery. The efcacy of ketamine administered in these ways is controversial, and there are several reports of unpleasant systemic side-effects (96, 97). The neurotoxicity of ketamine is not yet clear, and further animal studies are needed. There is a theoretical interaction between the NMDA-receptor system and the opioid receptor system in the dorsal horn. Ketamine may be of benet in combination with opioids, especially regarding the reduction of tolerance after long-term treatment with opioids (98, 99). Ketamine is a racemic mixture of two enantiomers, S()-ketamine and R()-ketamine. S()-ketamine is 34 times more potent than R()-ketamine. Although some report that the S() enantiomer has fewer psychomimetic side-effects, there are clinical studies which indicate the opposite (100102). The S() enantiomer will soon be commercially available in Europe, and further studies are necessary to establish whether the use of one of the enantiomers has clinical advantages. In summary, the use of ketamine as an analgesic in the immediate postoperative period is of limited value. Other NMDA-antagonists with a better specicity and afnity, such as dextromethorphan, may prove more benecial and are now under clinical investigation (103).
a2-receptor agonists
a2-receptor agonists have sedative, anxiolytic, analgesic and haemodynamic properties. Veterinarians have used this group of drugs as anaesthetics for many years, but its use in humans as an analgesic is recent. Clonidine and dexdemetomidine have been used as
1195
V. Dahl and J. C. Rder
preoperative anxiolytic and sedative drugs (104, 105), and dexmedetomidine has been tried out as an anaesthetic agent (106, 107). However, the severe side-effects, such as sympatholysis, hypotension and bradycardia, limit their use in clinical practice (108). Thus, regarding general anaesthetic properties, these drugs will remain adjuvants (109). The a2-agonists clonidine and dexmedetomidine are imidazoline compounds with different partial agonist properties, dexmedetomidine with a selectivity ratio of 1600:1 for a2:a1 and clonidine with 200:1. The a2-receptors are widely spread in the central nervous system, and three isoreceptors have been recognised. The receptor is the binding site for the adrenergic neurotransmitter norepinephrine. a2-adrenoceptors are located on primary afferent terminals (centrally and in the periphery); they are also found in the supercial laminae of the spinal cord and within several brainstem nuclei involved in analgesia (110). Animal studies support analgesic action at all three sites, although their relative importance is controversial (111). There is clear evidence of a spinal site of action for clonidine (112, 113). Clonidine, 150 mg, injected intrathecally after caesarean section or minor orthopaedic surgery yields analgesia for 46 h (114, 115). Epidural administration of a larger dose of clonidine produces analgesia with 50% reduction in opioid requirement (116). Clonidine is approximately twice as potent given epidurally compared with intravenously (117). The most interesting aspect of intrathecal or epidural administration of a2-receptor agonists is their synergistic action with opioids (118, 119). An epidural bolus administration of the combination of fentanyl and clonidine will reduce the analgesic dose of each component by approximately 60% (120). Clonidine will
also enhance and prolong the effect of local anaesthesia intrathecally (121, 122). Peripheral administration of clonidine also seems to have analgesic properties (123, 124), possibly by a reduction of norepinephrine release in the terminal nerve endings. There is also evidence of additional analgesia when added to local anaesthesia in peripheral nerve blocks (125). The use of clonidine for regional analgesia is summarised in Table 2. The use of larger doses of clonidine as an analgesic is limited by its sedative/anaesthetic properties by actions in the locus coeruleus (126). Sedation after epidural administration of clonidine reects a substantial systemic absorption. Epinephrine, an a-receptor agonist with little selectivity, has been widely used as an adjuvant to spinal and epidural administration of local anaesthesia and opioids for many years (127, 128). Epinephrine improves the analgesic properties and prolongs the duration of action from intrathecally or epidurally administered analgesic regimens. Epinephrine seems to act both as a a2-agonist at the spinal cord level and as a local vasoconstrictor in the epidural space, thus reducing the systemic absorption of local anaesthetics and opioids (129). There are, however, some concerns about the possible detrimental effect of epinephrine to the blood supply of the spinal cord (130). Nevertheless, the addition of epinephrine 2 mg/ml to epidural solutions is widely used in the Scandinavian countries and seems to be safe and well tolerated (129). In postoperative pain treatment, the use of the a2receptor agonists as an adjuvant to epidurally or intrathecally administered opioids and local anaesthetics is highly benecial. Its synergistic action with these drugs will substantially reduce the doses
Table 2
Summary of clinical experience with clonidine for regional analgesia. Patient group Intraoperative Postoperative Use Alone local anesthetic Alone opioid bupivacaine bupivacaine bupivacaine Alone mepivacaine Dose 300600 mg 150 mg 400 mg 75150 mg 20 mg/h 75 mg 13 mg/kg 75150 mg 150300 mg 10100 mg Effect anesthetic use by 5075% Prolonged anaesthesia by 50100% Analgesia 5 h Prolongs analgesia by 100% opioid use 50%, pain relief Prolongs analgesia 100% Prolongs analgesia 100% Prolongs analgesia 30% Reduces tourniquet pain 710 h analgesia Prolongs analgesia 50100% Side-effects blood-pressure sedation Sedation, BP Minimal (Reduced hypoxaemia) Minimal Minimal Minimal Sedation, BP Minimal
Obstetric (labour) Paediatrics (caudal) Spinal administration intraoperative Postoperative Peripheral nerve block
Adapted from: Eisenbach, De Kock and Klimscha (111).
1196
Non-opioid postoperative analgesia
needed of each drug, thus reducing the possible sideeffects. In the future, a better understanding of the structural differences of the different a2-receptors may result in an extended therapeutic use of more selective a2-agonists.
Miscellaneous
Neostigmine
Neostigmine administrated intrathecally in animal models increases the concentration of acetylcholine and produces analgesia (132, 133). This analgesic effect can be reversed with a muscarin antagonist, thus indicating an action by the cholinergic system. In humans, intrathecal doses ranging from 25 mg to 75 mg have produced analgesia in patients undergoing vaginal hysterectomies or orthopaedic surgery (134, 135). These studies have also revealed a dose-related incidence of troublesome side-effects, especially nausea and vomiting. More recent studies have shown analgesic effects of much lower doses of neostigmine with a very low incidence of side-effects. Doses as low as 5 mg or 10 mg still have analgesic properties (136, 137). Lauretti and colleagues have shown a dose-independent analgesic effect of intrathecal neostigmine at doses of 14 mg/kg without any side-effects after minor orthopaedic procedures (137). The use of neostigmine intrathecally as an analgesic adjuvant is still experimental and only further studies will reveal its usefulness in the clinical setting.
sient lumbar pain during treatment (143, 144). Intravenous infusion of adenosine has been shown to reduce isourane concentration requirements and stabilise blood pressure during general anaesthesia (145). A low dose of perioperative adenosine, 80 mg kg1 min1, reduces both the peroperative need of volatile anaesthetic and the postoperative opioid analgesic requirement after abdominal hysterectomy and breast surgery (146, 147). Adenosine infusion may also induce pain in healthy volunteers (148, 149) and angina-like pain in patients with angina pectoris (150). In the periphery, the sensitisation of the primary nociceptive afferent is probably mediated by the A2-receptor subtype. Adenosine induced chest pain was inhibited by the A1-receptor antagonist aminophylline, thus suggesting an A1-mediated effect (151). The use of adenosine in postoperative treatment is precluded by its complex mode of action, possible side-effects and short half-life. It may have a useful role in the treatment of complex, chronic pain conditions. The role of a more specic A1-receptor agonist is still experimental.
Corticosteroids
The glucocorticoids block both the cyclo-oxygenase and the lipo-oxygenase pathways in the inammatory cascade, thus implying a profound effect in the eicosanoid and the prostanoid pain mediation. The use of glucocorticoids to reduce pain and inammation after dental surgery is well documented (152154). Analgesic effects have also been reported after general surgery (155), orthopaedic surgery (156) and back surgery (157). A single dose of 12 mg betamethasone intramuscularly before surgery for ambulatory procedures reduced both postoperative pain and nausea (158). Though there might be a concern about possible impairment of the immune system, corticosteroids seem safe to use as postoperative adjuvants for a limited period of time. This is especially the case in patients with contraindication to NSAIDs. The welldocumented anti-emetic effect is an additional benet from using corticosteroids (158, 159).
Adenosine
The purine nucleotide adenosine 5-triphosphate (ATP) is a part of every cell in the human body, and plays a vital role in the cell metabolism. Extracellular ATP and its metabolite adenosine have pronounced effects in several biological processes such as liver glycogen metabolism, muscle contraction, cardiac function, platelet function and neurotransmission (138). The effect of adenosine is mediated through at least two different subtypes of cell-surface receptors, the A1 and A2 receptors. The A1-subtype receptor seems to be involved in modulation of pain transmission at the spinal level, and the effect is linked to the inhibition of the adenyl cyclase activity (139141), reduced Ca2 presynaptic inux (140) or inhibition of substance P-like immmunoreactivity (142). Because of its short half-life in the tissues, adenosine must be used as a continuous infusion. Intrathecal administration of adenosine has been used with some success to treat patients with chronic neuropathic pain, but a subpopulation reported tran-
Non-pharmacological techniques
The possible side-effects of both opioid and nonopioid pharmacological treatment of postoperative pain make the use of non-pharmacological techniques interesting, especially in the outpatient setting. Transcutaneous electrical stimulation (TENS), acupuncturelike transcutaneous electrical stimulation (ALTENS) and percutaneous electrical nerve stimulation (PENS) are widely used in the treatment of chronic pain conditions. The use of these techniques is increasing in
1197
V. Dahl and J. C. Rder
postoperative pain treatment (160). TENS has been shown to reduce pain after knee surgery (161), and studies indicate a 1530% decrease in postoperative opioid requirement (162). There are studies, however, which fail to show any clinical benets from TENS (163). Acupuncture has been tried out with variable success (164, 165). The possible mechanism of the effect of these afferent impulse techniques includes stimulation of descending, pain-inhibitory pathways, inhibition of substance P release and the release of endogenous opioid substances within the central nervous system (160). The use of cryoanalgesia after orthopaedic surgery seems efcacious (166, 167) and has supplementary positive effects such as reduction of postoperative oedema. Also, preoperative psychological preparation for a surgical procedure, psychoprophylaxis, reduces the need for postoperative analgesics (168). The use of non-pharmacological techniques is interesting, but needs further clinical investigation.
properties as efcacious as morphine in animal trials (174). A neuronal type of calcium channel blocker SNX-111, derived from the venom of the pacic cone snail, is under investigation for its pain modulating properties (174).
Summary
Although signicant improvement has been made in the treatment of pain in the postoperative period, many patients still experience unnecessary discomfort resulting in distress, higher morbidity and prolonged stay in hospital. The standard pillar of postoperative treatment of severe pain is the use of opioids. However, adverse reactions to opioids make their use unfavourable. A better understanding of the pathophysiology of pain has helped clinicians to a more balanced approach to postoperative pain treatment. The development of the multimodal approach to postoperative analgesia, with the use of different drugs acting via different routes to give good analgesia, with minimal side-effects, represents a major development in the treatment of postoperative pain. Early, aggressive mobilisation and feeding must follow in order to restore normal conditions quickly. Alternatives to opioids should be used as extensively as possible. Local anaesthesia, used as regional blocks or as wound inltration, is most benecial. Paracetamol has good basic analgesic properties, and should probably be used in dosages higher than recommended today. The combination with a NSAID results in better and longer-lasting analgesia. The intravenous form propacetamol will increase the possibilities of its use. The new concept of selective COX-2 inhibiting NSAIDs will result in analgesic and anti-inammatory drugs with fewer side-effects. The wellknown inexpensive group of corticosteroids have good analgesic and anti-emetic properties, and are especially interesting to use in patients who do not tolerate NSAIDs. The a2-receptor agonists like clonidine, when administered epidurally or intrathecally, are useful adjuncts, but their adverse effects on sedation and hypotension limit their use. NMDA-receptor antagonists are of limited value in the postoperative period. Adenosine and neostigimine are still on a research level but may lead to new, clinically useful analgesic drugs. In the future, cannabinoids, cholecystokinin-receptor antagonists and neurokinin-1 antagonists may become important analgesic drugs.
Possible drugs in the future
Cannabinoids: Cannabis has been known for thousands of years, and is popular in recreational use for its psychoactive properties. Cannabis has also been used as a therapeutic against emesis, pain and loss of appetite. Lately, two cannabinoid receptors (CB1 and CB2) and their endogenous ligands have been identied. There is growing evidence for a potential therapeutical use of synthetic cannabinoid receptor agonists and antagonists, and a number are under clinical investigation, including cannabdiol (neuroprotection), CT3 (analgesia and anti-inammation), anandamide (analgesia), palmithylethanolaminide (analgesia) and SR-141716 (antipsychosis) (169). Cholecystokinin (CCK) is an important regulator of gastrointestinal function, but it is also a neurotransmitter in the central nervous system. Animal studies indicate a nociceptive action of the specic CCK-B receptor antagonist (170). Neurokinin-1 (NK-1) antagonists have been shown to block the induction but not the maintenance of central sensitisation (171, 172), and may prove useful in a pre-emptive context. Calcium channel blockers such as verapamil are under clinical investigation as an adjuvant to epidural analgesia with local anaesthesia (173). Even further removed from clinical practice, research on natural venoms might reveal interesting substances. Epibatidine, a substance extracted from the skin of the poisonous tree frog, epipedobates tricolor, seems to bind to the acetylcholine receptor. Its nicotine-like structure has been determined and the chemical substance ABT-594 demonstrates analgesic
References
1. Kehlet H. Surgical stress: The role of pain and analgesia. Br J Anaesth 1989: 63: 189195.
1198
Non-opioid postoperative analgesia
2. Calvey TN, Williams NE. Principles and practice of pharmacology for anaesthetists. Cambridge: Blackwell Science, 1997. 3. Dahl JB, Rosenberg J, Dirkes WE, Mogensen T, Kehlet H. Prevention of postoperative pain by balanced analgesia. Br J Anaesth 1990: 64: 518520. 4. Wall PD. The prevention of postoperative pain. Pain 1988: 33: 289290. 5. McQuay HJ. Pre-emptive analgesia. Br J Anaesth 1992: 69: 1 3. 6. Cousins MJ. Acute pain and the injury response: Immediate and prolonged effects. Reg Anesth 1989: 14: 162179. 7. Levine JD, Coderre JJ, Basbaum AI. The peripheral nervous system and the inammatory process. In: Dubner R, Gebhart GF, Bond MR, eds. Proceedings of the Vth world congress on Pain. Amsterdam: Elsevier Science Publishers, 1988: 33 43. 8. Raja SN, Meyer RA, Campbell JN. Peripheral mechanisms of somatic pain. Anesthesiology 1988: 68: 571590. 9. McMahon SB. NGF as mediator of inammatory pain. Philos Trans R Soc Lond B Biol Sci 1996: 351: 431440. 10. Lewin GR, Rueff A, Mendell LM. Peripheral and central mechanisms of NGF-induced hyperalgesia. Eur J Neurosci 1994: 6: 19031912. 11. Dougherty PM, Willis WD. Enhancement of spinothalamic neuron responses to chemical and mechanical stimuli following combined micro-iontophoretic application of Nmethyl-D-aspartic acid and substance P. Pain 1991: 47: 85 93. 12. Aley KO, McCarter G, Levine JD. Nitric oxide signaling in pain and nociceptor sensitization in the rat. J Neurosci 1998: 18: 70087014. 13. Stein C. Peripheral and non-neuronal opioid effects. Current Opinion in Anaesthesiology 1994: 7: 347351. 14. Lambert DG. Opioid receptors. Current Opinion in Anaesthesiology 1995: 8: 317322. 15. Westlund KN, Bowker RM, Ziegler MG, Coulter JD. Origins and terminations of descending noradrenergic projection to the spinal cord of the monkey. Brain Res 1984: 292: 116. 16. Bowker R, Westlund KN., Coulter JD. Origin of serotonergic projections of the spinal cord in rat: an immunocytochemical-retrograde transport study. Brain Res 1981: 226: 187199. 17. Singh VK, Bajpai K, Biswas S, Haq W, Khan MY, Mathur KB. Molecular biology of opioid receptors: Recent advances. Review Neuroimmunomodulation 1997: 4: 285297. 18. Calo G. The orphan receptor and nociception. ESA 8th annual meeting refresher course lectures. 2000: 197201. 19. Pedersen SH, Douville LM, Eberlein TJ. Accelerated surgical stay programs: a mechanism to reduce health care costs. Ann Surg 1994: 219: 374381. 20. Kehlet H, Rung GW, Callesen T. Postoperative opioid analgesia: time for a reconsideration. J Clin Anesth 1996: 8: 441 445. 21. Esmail Z, Montgomery C, Courtm C, Kestle J. Efcacy and complications of morphine infusions in postoperative paediatric patients. Paediatr Anaesth 1999: 9: 321327. 22. Miniche S, Hansen BL, Christensen S-E, Dahl JB, Kehlet H. Activity of patients and duration of hospitalisation following hip-replacement with balanced treatment of pain and early mobilisation. Ugeskr Lger 1992: 154: 14951499. 23. Woolf CJ, Chong MS. Preemptive analgesia Treating postoperative pain by preventing the establishment of central sensitization. Anesth Analg 1993: 77: 362379. 24. Dahl V, Raeder JC, Ern PE, Kovdal A. Pre-emptive effect of pre-incisional versus post-incisional inltration of local anaesthesia on children undergoing hernioplasty. Acta Anaesthesiol Scand 1996: 40: 487451. 25. Dahl JB, Kehlet H. The value of pre-emptive analgesia in the treatment of postoperative pain. Br J Anaesth 1993: 70: 434 439. 26. Breivik H. Pre-emptive analgesia. Current Opinion in Anaesthesiology 1994: 7: 458461. 27. Tverskoy M, Coszacov C, Ayache M, Bradley EL, Kissin I. Postoperative pain after inguinal herniorraphy with different types of anesthesia. Anesth Analg 1990: 70: 2935. 28. Moss G, Regal ME, Lichtig L. Reducing postoperative pain, narcotics, and length of hospitalisation. Surgery 1986: 99: 206210. 29. McLoughlin J, Kelley CJ. Study of the effectiveness of bupivacaine inltration of the ilioinguinal nerve at the time of hernia repair for postoperative pain relief. Br J Clin Pract 1989: 8: 281283. 30. Owen H, Galloway DJ, Mitchell KG. Analgesia by wound inltration after surgical excision of benign breast lumps. Ann R Coll Surg Engl 1985: 67: 114115. 31. Patridge BL, Stabile BE. The effects of incisional bupivacaine on postoperative narcotic requirement, oxygen saturation and length of stay in the postoperative unit. Acta Anaesthesiol Scand 1990: 34: 486491. 32. Bourne MH, Johnson KA. Postoperative pain relief using local anesthetic instillation. Foot Ankle 1988: 8: 350351. 33. Pryn SJ, Cross MM, Murison SC, McGinn FP. Postoperative analgesia for haemorroidectomy. Anaesthesia 1989: 44: 964 966. 34. Uzunkoy A, Coskun A, Akinci F. The application of local anaesthesia before and after surgery in laparoscopic cholecystectomy. IMRA 1999: 11: A 75. 35. Sinclair R, Cassuto J, Hogstrom S et al. Topical anesthesia with lidocaine aerosol in the control of postoperative pain. Anesthesiology 1988: 68: 895901. 36. Narchi A, Benhamou D, Fernandez H. Intraperitoneal local anesthetic for shoulder pain after day-case laparoscopy. Lancet 1991: 338: 15691570. 37. Tree-Trakarn T, Pirayavaraporn S, Lertakyamee J. Topical analgesia for relief of post-circumcision pain. Anesthesiology 1987: 67: 395399. 38. Lisander B. An antiinammatory effect of lidocaine. Acta Anaesthesiol Scand 1996: 40: 285286. 39. Elhakim M, Elkott M, Ali M, Tahoun HM. Intraperitoneal lidocaine for postoperative pain after laparoscopy. Acta Anaesthesiol Scand 2000: 44: 280284. 40. Amid PK, Shulman AG, Lichtenstein IL. Local anaesthesia for inguinal hernia repair: step-by-step procedure. Ann Surg 1994: 220: 735737. 41. Dahl JB, Frederiksen HJ. Wound inltration for operative and postoperative analgesia. Current Opinion in Anaesthesiology 1995: 8: 835840. 42. Renck H, Hassan HG, Lindberg B, kerman B. Effects of macromolecular adjuvants on the duration of prilocaine. Experimental studies on the effect of variations of viscosity and sodium content and of inclusion of adrenaline. Acta Anaesthesiol Scand 1988: 32: 355364. 43. Grant GJ, Lax J, Susser L, Zakowski M, Weissman TE, Turndorf H. Wound inltration with liposomal bupivacaine prolongs analgesia in rats. Acta Anaesthesiol Scand 1997: 41: 204207. 44. Engstrm S, Engstrm L. Phase behavior of the lidocainemonoolein water system. Int J Pharmaceutics 1992: 79: 113122. 45. Vane JR. Inhibition of prostaglandin synthesis as a mechanism of the action for the aspirin-like drugs. Nature New Biol 1971: 231: 232235. 46. Ferrante MF. Non-steroidal anti-inammatory drugs. In: Ferranta MF, VadeBoncouer TR, eds. Postoperative pain management. New York: Churchill Livingstone, 1993: 133143.
1199
V. Dahl and J. C. Rder
47. Trang LE. Prostaglandins and inammation. Semin Arthritis Rheum 1980: 9: 153155. 48. Rmsing J, Miniche S, stergaard D, Dahl JB. Local inltration with NSAIDs for postoperative analgesia: Evidence for a peripheral analgesic action. Acta Anaesthesiol Scand 2000: 44: 672683. 49. Bjrkman R, Hedner T, Hallman KM, Henning M, Hedner J. Localisation of the central antinociceptive effects of diclofenac in the rat. Brain Res 1992: 590: 6673. 50. Dahl JB, Kehlet H. Non-steroidal anti-inammatory drugs: rationale for use in severe postoperative pain. Br J Anaesth 1991: 66: 703712. 51. Engel C, Lund B, Kristensen SS, Axel G, Nielsen JB. Indomethacin as an adjacent after hysterectomies. Acta Anaesthesiol Scand 1989: 33: 489501. 52. Dahl V, Raeder JC, Drsdal S, Wathne O, Brynhildsrud J. Prophylactic oral ibuprofen or ibuprofen-codeine versus placebo for postoperative pain after primary hip arthroplasty. Acta Anaesthesiol Scand 1995: 39: 323326. 53. Oosterlink W, Philip NH, Charing C. A double blind single dose comparison of intramuscular ketorolac trometamine and pethidine in the treatment of renal colic. J Clin Pharmacol Ther 1990: 30: 336341. 54. Bertin L, Pons G, dAthis A et al. A randomized, double blind, multicentre controlled trial of ibuprofen versus acetaminophen and placebo for symptoms of acute otitis media in children. Fundam Clin Pharmacol 1996: 10: 387392. 55. Mather SJ, Peutrell JM. Postoperative morphine requirements, nausea and vomiting following anaesthesia for tonsillectomy. Comparison of intravenous morphine and nonopioid analgesic techniques. Paediatr Anaesth 1995: 5: 185 188. 56. Bhatt-Metha V, Rosen DA. Management of acute pain in children. Clin Pharm 1991: 10: 667685. 57. Hawkey CJ. Non-steroidal anti-inammatory drugs and peptic ulcers. Br Med J 1990: 300: 278284. 58. Strom BL, Berlin JA, Kinmal JL et al. Parenteral ketorolac and risk of gastrointestinal and operative site bleeding. A postmarketing surveillance study. JAMA 1996: 275: 376382. 59. Feldman HI, Kinman JL, Berlin JA et al. Parenteral ketorolac: the risk for acute renal failure. Ann Intern Med 1997: 126: 193199. 60. Zikowski D, Hord AH, Haddow JD. Ketorolac induced bronchospasm. Anesth Analg 1993: 76: 417419. 61. Thwaites BK, Nigus DB, Bouska GW, Mongan PD, Ayala EF, Merrill GA. Intravenous ketorolac thromethamine does not worsen platelet function during knee arthroscopy under general anaesthesia. Anesth Analg 1995: 81: 119124. 62. Weale A, Warvik D, Durant N. Is there hemostatic interaction between low-molecular-weight heparin and non-steroidal analgesics after total hip replacement? [letter] Lancet 1993: 342: 995. 63. Goppelt-Struebe M. Regulation of prostaglandin endoperoxide synthase (cyclooxygenase) isoenzyme expression. Prostaglandins Leukot Essent Fatty Acids 1995: 52: 213222. 64. Camu F. COX-1 and COX-2 inhibition current status and future perspectives. 6th ESA annual meeting, Barcelona, 1998: 14RC1. 65. Mitchell JA, Akarasereenont P, Thiemermann C, Flower RJ, Vane JR. Selectivity of non-steroidal anti-inammatory drugs as inhibitors of constitutive and inducible cyclooxygenase. Proc Natl Acad Sci U S A 1993: 90: 1169311697. 66. Warner TD, Giuliano F, Vojnovic I, Bukasa A, Mitchell JA, Vane JR. Nonsteroid drug selectivities for cyclo-oxygenase1 rather than cyclo-oxygenase-2 are associated with human gastrointestinal toxicity: a full in vitro analysis. Proc Natl Acad Sci U S A 1999: 96: 75637568. 67. Bannwarth B, Netter P, Lapicque F et al. Plasma and cerebrospinal uid concentrations of paracetamol after a single intravenous dose of propacetamol. Br J Clin Pharmacol 1992: 34: 7981. 68. Piletta P, Porchet HC, Dayer P. Central analgesic effect of acetaminophen but not of aspirin. Clin Pharmacol Ther 1991: 49: 350354. 69. Moore A, Collins S, Carroll D, McQuay H. Paracetamol with and without codeine in acute pain: a quantitative systematic review. Pain 1997: 70: 193201. 70. Montgomery JE, Sutherland CJ, Kestin IG, Sneyd JR. Morphine consumption in patients receiving rectal paracetamol and diclofenac alone and in combination. Br J Anaesth 1996: 77: 445447. 71. Seymor RA, Kelly PJ, Hawkesford JE. The efcacy of ketoprofen and paracetamol (acetaminophen) in postoperative pain after third molar surgery. Br J Clin Pharmacol 1996: 41: 581585. 72. Breivik EK, Barkvoll P, Skovlund E. Combining diclofenac with acetaminophen or acetaminophen-codeine after oral surgery: a randomised, double blind, single oral dose study. Clin Pharmacol Ther 1999: 66: 625635. 73. Anderson BJ, Holford NHG, Woollard GA, Kanagasundaram S, Mahadevan M. Perioperative pharmacodynamics of acetaminophen analgesia in children. Anesthesiology 1999: 90: 411421. 74. Korpela R, Korvenoja P, Meretoja OA. Morphine-sparing effect of acetaminophen in pediatric day-case surgery. Anesthesiology 1999: 91: 442447. 75. Bremerich DH, Neidhart G, Kessler P, Behne M. Prophylactically administered rectal acetaminophen does not result in analgesic serum concentrations and has no opioid-sparing effect in the early postoperative period in small children. EJA 2000: 17 (Suppl 19): A 485. 76. Blume H, Ali SL, Elze M et al. Relative Bioverfrbarkeit Von Paracetamol in Suppositorien-zubereitungen im Vergleich zu Tabletten. Arzneimittelforsch 1994: 12: 13331338. 77. Peduto VA, Ballabio M, Stefanini S. Efcacy of propacetamol in the treatment of postoperative pain morphine-sparing effect in orthopedic surgery. Acta Anaesthesiol Scand 1998: 42: 293298. 78. Rannug U, Holme JA, Hongslo JK et al. An evaluation of the genetic toxicity of paracetamol. Mutat Res 1995: 327: 179 200. 79. Bach PF, Hardy TI. Relevance of animal models to analgesicassociated papillary necrosis in human. Kidney Int 1985: 28: 605613. 80. Peterson RG, Rumack BH. Age as a variable in acetaminophen overdose. Arch Intern Med 1981: 141: 390393. 81. Bergamn K, Muller L, Teigen SW. Current issues in mutagenesis and carcinogenesis: the genotoxicity and carcigenotoxicity of paracetamol. Mutat Res 1996: 349: 263288. 82. Woolf CJ, Thomson SW. The induction and maintenance of central sensitisation is dependent on N-methyl-D-aspartic acid receptor activation: implication for the treatment of post-injury pain hypersensitivity states. Pain 1991: 44: 293 299. 83. Ma QP, Woolf CJ. Noxious stimuli induce an N-methyl-Daspartate receptor dependent hypersensitivity of the exion withdrawal reex to touch: Implications for the treatment of mechanical allodynia. Pain 1995: 61: 383390. 84. Stubhaug A. Ketamine in the treatment of spontaneous ongoing pain and evoked pain. Thesis. Oslo: University of Oslo, 1999. 85. Hirota K, Lambert DG. Ketamine: Its mechanism(s) of action and unusual clinical use. Br J Anaesth 1996: 77: 441 444.
1200
Non-opioid postoperative analgesia
86. Eide PK, Stubhaug A, Breivik H, Oye I. Reply to ST Meller: Ketamine relief from chronic pain through actions at the NMDA receptor. Pain 1997: 72: 289291. 87. Tverskoy M, Oz Y, Isakson A, Finger J, Bradley EL, Kissin I. Preemptive effect of fentanyl and ketamine on postoperative pain and wound hyperalgesia. Anesth Analg 1994: 78: 205209. 88. Fu ES, Miguel R, Scharf JE. Preemptive ketamine decreases postoperative narcotic requirements in patients undergoing abdominal surgery. Anesth Analg 1997: 84: 10861090. 89. Dich-Nielsen JO, Svendsen LB, Berthelsen P. Intramuscular low-dose ketamine versus pethidine for postoperative pain treatment after thoracic surgery. Acta Anaesthesiol Scand 1992: 36: 583587. 90. Mathisen LC, Aasb V, Raeder JC. Lack of pre-emptive effect of R-ketamine in laparoscopic cholecystectomy. Acta Anaesthesiol Scand 1999: 43: 220224. 91. Adam F, Libier M, Oszustrowicz T, Lefebvre D, Beal J, Meynadier J. Preoperative small-dose ketamine has no preemptive analgesic effect in patients undergoing total mastectomy. Anesth Analg 1999: 89: 444447. 92. Kharash ED. Pharmacokinetics of ketamine. In: TA Bowdle, A Horita, ED Karasch, eds. The pharmacologic basis of anaesthesiology. New York: Churchill Livingstone, 1995: 357373. 93. Bowdle TA, Radant AD, Cowley DS, Kharasch ED, Strassman RJ, Roy-Byrne PP. Psychedelic effects of ketamine in healthy volunteers. Anesthesiology 1998: 88: 822828. 94. Eide PK, Jrum E, Stubhaug A, Bremnes J, Breivik H. Relief of post-herpetic neuralgia with the N-methyl-D-aspartic acid receptor antagonist ketamine: a double-blind, crossover comparision with morphine and placebo. Pain 1994: 58: 347354. 95. Arendt-Nielsen L, Petersen-Felix S, Fischer M, Bak P, Bjerring P, Zbinden AM. The effect of N-methyl-D-aspartate antagonists (Ketamine) on single and repeated nociceptive stimuli: a placebo-controlled experimental human study. Anesth Analg 1995: 81: 6368. 96. Schneider I, Diltoer M. Continuous extradural infusion of ketamine during labour. Can J Anaesth 1987: 34: 657658. 97. Bion JF. Intrathecal ketamine for war surgery. A preliminary study under war conditions. Anaesthesia 1984: 39: 10231028. 98. Dickenson AH. NMDA receptor antagonists: interaction with opioids. Acta Anaesthesiol Scand 1997: 41: 15. 99. Bell RF. Low-dose subcutaneous ketamine infusion and morphine tolerance. Pain 1999: 83: 101103. 100. White PF, Ham J, Way WL, Trevor AJ. Pharmacology of ketamine isomers in surgical patients. Anesthesiology 1980: 52: 231239. 101. Calvey TN. Chirality in anaesthesia. Anaesthesia 1992: 47: 9394. 102. Mathisen LC, Skjelbred P, Skoglund LA, Oye I. Effect of ketamine, an NMDA receptor inhibitor, in acute and chronic orofacial pain. Pain 1995: 61: 215220. 103. Wu CT, Yu JC, Yeh CC et al. Preincisional dextromethorphan treatment decreases postoperative pain and opioid requirement after laparoscopic cholecystectomy. Anesth Analg 1999: 88: 13311334. 104. Carabine UA, Wright PMC, Moore J. Preanaesthetic medication with clonidine: a dose-response study. Br J Anaesth 1991: 67: 7983. 105. Scheinin H, Jaakola M-L, Sjvall S et al. Intramuscular dexmedetomidine as premedication for general anaesthesia. A comparative multi-center study. Anesthesiology 1993: 79: 10651075. 106. Aho M, Erkola O, Kallio A, Scheinin H, Korttila K. Dexmedetomidine infusion for maintenance of anaesthesia in patients undergoing abdominal hysterectomy. Anesth Analg 1992: 75: 940946. Buhrer M, Mappes A, Lauber R, Stanski DR, Maitre PO. Dexmedetomidine decreases thiopental dose requirement and alters distribution pharmacokinetics. Anesthesiology 1994: 80: 12161227. Kanto J. Clincal pharmacology of dexmedetomidine. Acta Anaesthesiol Scand 1993: 37 (Suppl 100): 177179. Kanto J. The place of alpha-2-agonists in anaesthesiology of today (editorial). Acta Anaesthesiol Scand 1997: 41: 45. Unnerstall JR, Kopajtic TA, Kuhar MJ. Distribution of alpha 2 agonists binding sites in the rat and human central nervous system: Analysis of some functional, anatomic correlates of the pharmacologic effects of clonidine and related adrenergic agents. Brain Res Rev 1984: 7: 69101. Eisenach JC, De Kock M, Klimscha W. a2-adrenergic agonists for regional anaesthesia. Anesthesiology 1996: 85: 655674. Eisenach JC, Detweiler D, Hood DD. Hemodynamic and analgesic actions of epidurally administered clonidine. Anesthesiology 1993: 78: 277287. Eisenach JC, Hood DD, Tuttle R, Shafer S, Smith T, Tong C. Computer-controlled epidural infusion to targeted cerebrospinal uid concentrations in humans: Clonidine. Anesthesiology 1995: 83: 3347. Bonnet F, Boico O, Rostaing S, Loriferne JF, Saada M. Clonidine-induced analgesia in postoperative patients: Epidural versus intramuscular administration. Anesthesiology 1990: 72: 423427. Filos KS, Goudas LC, Patroni O, Polyzou V. Intrathecal clonidine as a sole analgesic for pain relief after caesarean section. Anesthesiology 1992: 77: 267274. De Kock M, Crochet B, Morimont C, Scholtes J-L. Intravenous or epidural clonidine for intra- and postoperative analgesia. Anesthesiology 1993: 79: 525531. Bernard JM, Kick O, Bonnet F. Comparision of intravenous and epidural clonidine for postoperative patient-controlled analgesia. Anesth Analg 1995: 81: 706712. Yaksh TL, Reddy SVR. Studies in the primate on the analgesic effects associated with intrathecal actions of opiates, alpha adrenergic agonists and baclofen. Anesthesiology 1981: 54: 451467. Monasky MS, Zinsmeister AR, Stevens CW, Yaksh TL. Interaction of intrathecal morphine and ST-91 on antinociception in the rat: Dose-response analysis, antagonism and clearance. J Pharmacol Exp Ther 1990: 254: 383392. Eisenbach JC, DAngelo R, Taylor C, Hood DD. An isobolographic study of epidural clonidine and fentanyl after cesarean section. Anesth Analg 1994: 79: 285290. Bonnet F, Brun-Buisson V, Saada M, Boico O, Rostaing S, Touboul C. Dose-related prolongation of hyperbaric tetracaine spinal anesthesia by clonidine in humans. Anesth Analg 1989: 68: 619622. Liu S, Chiu AA, Neal JM, Carpenter RL, Bainton BG, Gerancher JC. Oral clonidine prolongs lidocaine spinal anesthesia in human volunteers. Anesthesiology 1995: 82: 1353 1359. Davis KD, Treede RD, Raja SN et al. Topical application of clonidine relieves hyperalgesia in patients with sympathetically maintained pain. Eur J Pharmacol 1991: 47: 309 317. Gentili M, Juhel A, Bonnet F. Peripheral analgesic effect of intra-articular clonidine. Eur J Pharmacol 1996: 64: 593596. Singelyn FJ, Dangoisse M, Bartholomee S, Gouverneur JM. Adding clonidine to mepivacaine prolongs the duration of anesthesia and analgesia after axillary brachial plexus block. Reg Anesth 1992: 17: 148150.
107.
108. 109. 110.
111.
112.
113.
114.
115.
116.
117.
118.
119.
120.
121.
122.
123.
124. 125.
1201
V. Dahl and J. C. Rder
126. Maze M, Tranquilli W. Alpha-2 adrenoceptor agonists: Dening the role in clinical anesthesia. Anesthesiology 1991: 74: 581605. 127. Eisenach JC, Grice SC, Dewan DM. Epinephrine enhances analgesia produced by epidural bupivacaine during labor. Anesth Analg 1987: 66: 447451. 128. Priddle HD, Andros GJ. Primary spinal anesthetic effects of epinephrine. Anesth Analg 1950: 29: 156162. 129. Niemi G, Breivik H. Adrenaline markedly improves thoracic epidural analgesia produced by low-dose infusion of bupivacaine, fentanyl and adrenaline after major surgery. Acta Anaesthesiol Scand 1998: 42: 897909. 130. Renck H. Neurological complications of central nerve blocks. Acta Anaesthesiol Scand 1995: 39: 859868. 131. Bouaziz H, Tong C, Eisenach JC. Postoperative analgesia from intrathecal neostigmine in sheep. Anesth Analg 1995: 80: 15. 132. Naguib M, Yaksh TL. Antinociceptive effects of spinal cholinesterase inhibition and isobolographic analysis of the interaction with m and a2 receptor systems. Anesthesiology 1994: 80: 13381348. 133. Lauretti GR, Hood DD, Eisenach JC, Pfeifer BL. A multicenter study of neostigmine for analgesia following vaginal hysterectomy. Anesthesiology 1998: 89: 913918. 134. Lauretti GR, Oliviera APM, Reis MP, Prado WA. Intrathecal neostigmine for postoperative analgesia after orthopedic surgery. J Clin Anesth 1997: 9: 473477. 135. Lauretti GR, Oliviera APM, Reis MP, Mattos AL. Transdermal nitroglycerine enhances spinal neostigmine postoperative analgesia following gynecological surgery. Anesthesiology 1998: 89: 1073A. 136. Kruskowski JA, Hood DD, Eisenach JC, Mallak KA, Parker RI. Intrathecal neostigmine for post cesarean analgesia: Dose-response. Anesth Analg 1997: 84: 12691275. 137. Lauretti GR, Oliveira R, Reis MP, Juliao MCC, Pereira NL. Study of three different doses of epidural neostigmine coadministered with lidocaine for postoperative analgesia. Anesthesiology 1999: 90: 15341538. 138. Agteresch HJ, Dagnelie PC, Van den Berg WO, Wilson JHP. Adenosine triphosphate: Established and potential clinical applications. Drugs 1999: 58: 211232. 139. Sollevi A. Adenosine for pain control. Acta Anaesthesiol Scand 1997: 110 (Suppl): 135136. 140. Poon A, Sawynok J. Antinociception by adenosine analogs and an adenosine kinase inhibitor: dependence on formaline concentration. Eur J Pharmacol 1995: 286: 177184. 141. Li J, Perl ER. Adenosine inhibition of synaptic transmission in the substantia gelatinosa. J Physiol 1994: 72: 16111621. 142. Sjlund KF, Sollevi A, Segerdahl M, Lundeberg T. Intrathecal adenosine analog administration reduces substance P in cerebrospinal uid along with behavioral effects that suggests antinociception in rats. Anesth Analg 1997: 85: 627 632. 143. Belfrage M, Segerdahl M, Arner S, Sollevi A. The safety and efcacy of intrathecal adenosine with chronic neuropathic pain. Anesth Analg 1997: 89: 136142. 144. Karlsten R, Goerdth T Jr. An A1-selective adenosine agonist abolishes allodynia elicited by vibration and touch after intrathecal injection. Anesth Analg 1995: 80: 844847. 145. Segerdahl M, Persson E, Ekblom A, Sollevi A. Peroperative adenosine infusion reduces isourane concentrations during general anaesthesia for shoulder surgery. Acta Anaesthesiol Scand 1996: 40: 792797. 146. Segerdahl M, Irestedt L, Sollevi A. Antinociceptive effect of perioperative adenosine infusion in abdominal hysterectomy. Acta Anaesthesiol Scand 1997: 41: 473479. 147. Segerdahl M, Ekblom A, Sandelin K, Wickman M, Sollevi A. Intraoperative adenosine infusion reduces the requirements for isourane and postoperative analgesia. Anesth Analg 1995: 80: 11451149. 148. Pappagallo M, Gaspardone A, Tomai F et al. Analgesic effect of bamiphylline on pain induced by intradermal injection of adenosine. Pain 1993: 53: 199204. 149. Watt AH, Lewis DJM, Horne JJ, Smith PM. Reproduction of epigastric pain of duodenal ulceration by adenosine. Br Med J 1987: 294: 1012. 150. Sylven, C, Beerman R, Jonzon B, Brandt R. Angina pectorislike pain provoked by intravenous adenosine in healthy volunteers. Br Med J 1986: 293: 227230. 151. Crea F, Pupita G, Galassi AR et al. Role of adenosine in pathogenesis of anginal pain. Circulation 1990: 81: 164172. 152. Skjelbred P, Lkken P. Postoperative pain and inammatory reaction reduced by injection of a corticosteroid. Eur J Clin Pharmacol 1982: 21: 291296. 153. Olstad OA, Skjelbred P. Comparison of the analgesic effect of corticosteroid and paracetamol in patients with pain after oral surgery. Br J Clin Pharmacol 1986: 22: 437442. 154. Baxendale BR, Vater M, Lavery KM. Dexamethasone reduces pain and swelling following extraction of third molar teeth. Anaesthesia 1993: 48: 961964. 155. Schulze S, Mller IW, Bang U et al. Effect of combined prednisolone, epidural analgesia and indomethacin on pain, systemic response and convalescence after cholecystectomy. Acta Chir Scand 1990: 156: 203209. 156. Vvargas JH, Ross DG. Corticosteroids and anterior cruciate ligament repair. Am J Sports Med 1989: 17: 532534. 157. Glasser Rs, Knego RS, Delashaw JB, Fessler Rg. The perioperative use of corticosteroids and bupivacaine in the management of lumbar disc disease. J Neurosurg 1993: 78: 383 387. 158. Aasboe V, Raeder JC, Groegaard B. Betamethasone reduces postoperative pain and nausea after ambulatory surgery. Anesth Analg 1998: 87: 319323. 159. Pappas ALS, Sukhani R, Hotaling A et al. The effect of preoperative dexamethasone on the immediate and delayed postoperative morbidity in children undergoing adenotonsillectomy. Anesth Analg 1998: 87: 5761. 160. White PF. Management of postoperative pain and emesis. Can J Anaesth 1995: 42: 10531055. 161. Arvidsson J, Eriksson E. Postoperative TENS pain relief after knee surgery: objective evaluation. Orthopedics 1986: 9: 13461351. 162. Tyler E, Caldwell C, Ghia JN. Transcutaneous electrical nerve stimulation: an alternative approach to the management of postoperative pain. Anesth Analg 1982: 61: 449456. 163. McCallum MI, Glynn CJ, Moore RA et al. Transcutaneous electrical nerve stimulation in the management of acute postoperative pain. Br J Anaesth 1988: 61: 308312. 164. Sung YF, Kutner MH, Cerine FC, Frederikson EL. Comparison of the effect of acupuncture and codeine on postoperative dental pain. Anesth Analg 1977: 56: 473478. 165. Ekblom A, Hansson P, Thomsson M, Thomas M. Increased postoperative pain and consumption of analgesia following acupuncture. Pain 1991: 44: 241247. 166. Schefer NM, Scheitel PL, Lipton NMN. Use of cryo/cuff for the control of postoperative pain and edema. J Foot Surg 1992: 31: 141148. 167. Dervin GF, Taylor DE, Keene GC. Effects of cold and compression dressings on early postoperative outcomes for the arthroscopic anterior cruciate ligament reconstruction patient. J Orthop Sports Phys Ther 1998: 27: 403406. 168. Egbert LD, Battit GE, Welch CE, Barlett MK. Reduction of
1202
Non-opioid postoperative analgesia
postoperative pain by encouragement and instruction of patient: a study of doctor-patient rapport. N Engl J Med 1964: 270: 825827. Pop E. Cannabinoids, endogenous ligands and synthetic analogs. Curr Opin Chem Biol 1999: 3: 418425. Yamamoto T, Nozaki-Taguchi N. The effect of intrathecally administered FK480, a cholcystokinin-A receptor antagonist, and YM022, a cholecystokinin-B receptor antagonist, on the formalin test in the rat. Anesth Analg 1996: 83: 107113. Ma Q-P, Woolf JC. Tachykinin NK1-receptor antagonist RP67580 attenuates progressive hypersensitivity of exor reex during experimental inammation in rats. Eur J Pharmacol 1997: 322: 165171. Traub RJ. The spinal contribution of substance P to the generation and maintenance of inammatory hyperalgesia in the rat. Pain 1996: 67: 151161. 173. Choe H, Kim JS, Ko SH et al. Epidural verapamil reduces analgesic consumption after lower abdominal surgery. Anesth Analg 1998: 86: 786790. 174. Silverstein JH. New concepts in anaesthesia receptors and neurotransmitters. ASA annual refresher course lectures October 913, 1999, Dallas, Texas: 264.
169. 170.
171.
172.
Address: Vegard Dahl Dept of Anaesthesia Brum Hospital N-1306 Brum postterminal Norway e-mail: vdahl/ah.telia.no
1203
Vous aimerez peut-être aussi
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryD'EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryÉvaluation : 3.5 sur 5 étoiles3.5/5 (231)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)D'EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Évaluation : 4.5 sur 5 étoiles4.5/5 (121)
- Grit: The Power of Passion and PerseveranceD'EverandGrit: The Power of Passion and PerseveranceÉvaluation : 4 sur 5 étoiles4/5 (588)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaD'EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaÉvaluation : 4.5 sur 5 étoiles4.5/5 (266)
- The Little Book of Hygge: Danish Secrets to Happy LivingD'EverandThe Little Book of Hygge: Danish Secrets to Happy LivingÉvaluation : 3.5 sur 5 étoiles3.5/5 (400)
- Never Split the Difference: Negotiating As If Your Life Depended On ItD'EverandNever Split the Difference: Negotiating As If Your Life Depended On ItÉvaluation : 4.5 sur 5 étoiles4.5/5 (838)
- Shoe Dog: A Memoir by the Creator of NikeD'EverandShoe Dog: A Memoir by the Creator of NikeÉvaluation : 4.5 sur 5 étoiles4.5/5 (537)
- The Emperor of All Maladies: A Biography of CancerD'EverandThe Emperor of All Maladies: A Biography of CancerÉvaluation : 4.5 sur 5 étoiles4.5/5 (271)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeD'EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeÉvaluation : 4 sur 5 étoiles4/5 (5794)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyD'EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyÉvaluation : 3.5 sur 5 étoiles3.5/5 (2259)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersD'EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersÉvaluation : 4.5 sur 5 étoiles4.5/5 (344)
- Team of Rivals: The Political Genius of Abraham LincolnD'EverandTeam of Rivals: The Political Genius of Abraham LincolnÉvaluation : 4.5 sur 5 étoiles4.5/5 (234)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreD'EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreÉvaluation : 4 sur 5 étoiles4/5 (1090)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceD'EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceÉvaluation : 4 sur 5 étoiles4/5 (895)
- Her Body and Other Parties: StoriesD'EverandHer Body and Other Parties: StoriesÉvaluation : 4 sur 5 étoiles4/5 (821)
- Kyusho Top Ten Points Vital Point Self ProtectionDocument57 pagesKyusho Top Ten Points Vital Point Self Protectiongreeneyedprincess100% (1)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureD'EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureÉvaluation : 4.5 sur 5 étoiles4.5/5 (474)
- Movement Disorders & Multiple Sclerosis-Kumar & Clark'sDocument8 pagesMovement Disorders & Multiple Sclerosis-Kumar & Clark'sindia2puppyPas encore d'évaluation
- The Unwinding: An Inner History of the New AmericaD'EverandThe Unwinding: An Inner History of the New AmericaÉvaluation : 4 sur 5 étoiles4/5 (45)
- Testing and Interpretation of Visual Perceptual Skills - CVS 2017Document76 pagesTesting and Interpretation of Visual Perceptual Skills - CVS 2017Katalin Molnár100% (2)
- The Yellow House: A Memoir (2019 National Book Award Winner)D'EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Évaluation : 4 sur 5 étoiles4/5 (98)
- On Fire: The (Burning) Case for a Green New DealD'EverandOn Fire: The (Burning) Case for a Green New DealÉvaluation : 4 sur 5 étoiles4/5 (73)
- Mental IllnessDocument10 pagesMental IllnessretnagumilangPas encore d'évaluation
- Therapy and The Neural Network Model: Theodore Wasserman Lori Drucker WassermanDocument210 pagesTherapy and The Neural Network Model: Theodore Wasserman Lori Drucker WassermanRonal Perino100% (1)
- Stress ManagementDocument33 pagesStress ManagementBabasab Patil (Karrisatte)Pas encore d'évaluation
- Nursing Care Plan For Peptic Ulcer NCPDocument2 pagesNursing Care Plan For Peptic Ulcer NCPderic85% (46)
- Guillain BarreDocument20 pagesGuillain BarreRama JosuaPas encore d'évaluation
- (P. v. Simonov (Auth.) ) The Emotional Brain PhysiDocument274 pages(P. v. Simonov (Auth.) ) The Emotional Brain PhysiludmilaromPas encore d'évaluation
- Adult Hemiplegia - Martha BobathDocument185 pagesAdult Hemiplegia - Martha BobathGabriela Marinescu88% (8)
- Cedera KepalaDocument102 pagesCedera KepalaNesaPas encore d'évaluation
- Cerebrovascular AccidentDocument17 pagesCerebrovascular Accidentmanisha paikarayPas encore d'évaluation
- The Nervous System: Dr. Garry NiedermayerDocument74 pagesThe Nervous System: Dr. Garry Niedermayersweta paudelPas encore d'évaluation
- Disorders of The Nervous System: Vascular DisorderDocument3 pagesDisorders of The Nervous System: Vascular DisorderHetty100% (1)
- Neurology - Headache - SOAP Note - Fiona CostelloDocument3 pagesNeurology - Headache - SOAP Note - Fiona CostelloSafiqul Islam ShawnPas encore d'évaluation
- Welcome To My Case Study Presentation: BHPI, CRP, Savar DhakaDocument19 pagesWelcome To My Case Study Presentation: BHPI, CRP, Savar DhakaKaushik Dipto RoyPas encore d'évaluation
- NBME Shelf Exam Sample Questions - PsychiatryDocument7 pagesNBME Shelf Exam Sample Questions - PsychiatryBasma TaherPas encore d'évaluation
- General Psychology (Soc. Sci. 1) Course Outline Psychology: The Study of BehaviorDocument5 pagesGeneral Psychology (Soc. Sci. 1) Course Outline Psychology: The Study of BehaviorShairuz Caesar Briones DugayPas encore d'évaluation
- Soal Bailey OsaDocument1 pageSoal Bailey OsaRowley GeoffPas encore d'évaluation
- Spatial Neglect - Overview, Etiology, Mechanisms and Morbidities in Spatial NeglectDocument9 pagesSpatial Neglect - Overview, Etiology, Mechanisms and Morbidities in Spatial NeglectRivulet1Pas encore d'évaluation
- NervousDocument25 pagesNervousfairyzzzPas encore d'évaluation
- KTP Mcat Quicksheets PDFDocument24 pagesKTP Mcat Quicksheets PDFChristine Annmarie TapawanPas encore d'évaluation
- 2019 GonzalezDocument15 pages2019 GonzalezAnn ChristinePas encore d'évaluation
- Neurological Disorders: Prof. Bernardo Fernandez IIDocument33 pagesNeurological Disorders: Prof. Bernardo Fernandez IIBernardPas encore d'évaluation
- Encephalopathies: Zerlyn T. Leonardo, M.D., FPCP, FPNADocument50 pagesEncephalopathies: Zerlyn T. Leonardo, M.D., FPCP, FPNAJanellee DarucaPas encore d'évaluation
- P300 and Emotiv PDFDocument16 pagesP300 and Emotiv PDFPaasol100% (1)
- Typical Absence Seizures and Their Treatment: Current TopicDocument5 pagesTypical Absence Seizures and Their Treatment: Current TopicAndika Eriza PutraPas encore d'évaluation
- Lecture 5Document4 pagesLecture 5Alina ChesimPas encore d'évaluation
- Rawatan Klien Dua DiagnosisDocument62 pagesRawatan Klien Dua DiagnosisPUSAT LATIHAN AADKPas encore d'évaluation
- Extract From Anatomy Course LectureDocument5 pagesExtract From Anatomy Course LectureMumuh Moe' MuhtadinPas encore d'évaluation