Vous aimerez peut-être aussi
- Saudi CPR Guidlines in EnglishDocument16 pagesSaudi CPR Guidlines in EnglishpiyushbamsPas encore d'évaluation
- Cardiac AssessmentDocument48 pagesCardiac AssessmentRatheesh NathPas encore d'évaluation
- Airway Obstruction - Types, Causes, and SymptomsDocument6 pagesAirway Obstruction - Types, Causes, and SymptomsGilbertLiem100% (1)
- Plasmapheresis Procedure Removes Antibodies From BloodstreamDocument13 pagesPlasmapheresis Procedure Removes Antibodies From BloodstreamSampath GoudPas encore d'évaluation
- Laws Applicable To HospitalsDocument6 pagesLaws Applicable To HospitalsRajat Tiwari100% (1)
- Severe Dengue in ICUDocument35 pagesSevere Dengue in ICUanaeshklPas encore d'évaluation
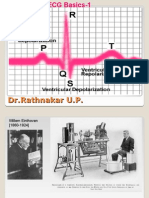
- ECG Basics 1Document24 pagesECG Basics 1Dr.U.P.Rathnakar.MD.DIH.PGDHMPas encore d'évaluation
- Paediatric and Neonatal Service and Clinical Quality IndicatorsDocument8 pagesPaediatric and Neonatal Service and Clinical Quality IndicatorsSyamsul Arifin100% (1)
- Anaphylaxis CEACCP 2004Document3 pagesAnaphylaxis CEACCP 2004kuruppukarlPas encore d'évaluation
- RSI For Nurses ICUDocument107 pagesRSI For Nurses ICUAshraf HusseinPas encore d'évaluation
- Difficult AirwayDocument77 pagesDifficult AirwayParvathy R Nair100% (1)
- A&E Triage SystemDocument5 pagesA&E Triage SystemArnel AlmutiahPas encore d'évaluation
- CABGDocument3 pagesCABGprofarmahPas encore d'évaluation
- Fumigation in Operation TheatresDocument22 pagesFumigation in Operation TheatresUtkarsh RaiPas encore d'évaluation
- Jurnal Reading Pembimbing: Dr. Iwan Sys Indrawanto, SP - KJDocument25 pagesJurnal Reading Pembimbing: Dr. Iwan Sys Indrawanto, SP - KJaribudiperdanaPas encore d'évaluation
- Pediatric Emergencies 1Document101 pagesPediatric Emergencies 1VIPIN V NAIR100% (1)
- Blood Transfusion Single Use PathwayDocument6 pagesBlood Transfusion Single Use PathwayropusanPas encore d'évaluation
- In-Patient Department Staff & Bed DistributionDocument6 pagesIn-Patient Department Staff & Bed DistributionSiddhi RanePas encore d'évaluation
- Informed ConsentDocument25 pagesInformed ConsentMaylodie ingallaPas encore d'évaluation
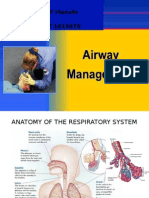
- Airway ManagementDocument42 pagesAirway ManagementOwy100% (4)
- Cardiac EmergencyDocument61 pagesCardiac EmergencyAgustina Tri P. DPas encore d'évaluation
- On Emergency DrugsDocument25 pagesOn Emergency DrugsBikram Chhetry100% (1)
- Patient Safety Guidelines for Anaesthesia MonitoringDocument21 pagesPatient Safety Guidelines for Anaesthesia MonitoringDzarrinPas encore d'évaluation
- Aldrete Discharge Scoring - Appropriate For Post Anesthesia PhaseDocument28 pagesAldrete Discharge Scoring - Appropriate For Post Anesthesia PhaseHeather PorterPas encore d'évaluation
- Stroke Society of the Philippines: Guide for Stroke TreatmentDocument22 pagesStroke Society of the Philippines: Guide for Stroke TreatmentSuresh ShresthaPas encore d'évaluation
- Chest TraumaDocument79 pagesChest TraumaAnusha VerghesePas encore d'évaluation
- Ivc FilterDocument15 pagesIvc FilterashishPas encore d'évaluation
- Monitoring of Patient in ICU: Prepared By: Ms. Anugrah Dayal TutorDocument19 pagesMonitoring of Patient in ICU: Prepared By: Ms. Anugrah Dayal TutorannuPas encore d'évaluation
- Post Cardiac ArrestDocument2 pagesPost Cardiac ArrestAlthea AlcalaPas encore d'évaluation
- Role of Code Blue TeamsDocument18 pagesRole of Code Blue TeamsBintang Lenny SihotangPas encore d'évaluation
- CABGDocument29 pagesCABGDeepika PatelPas encore d'évaluation
- Canadian Triage and Acuity Scale for PediatricsDocument30 pagesCanadian Triage and Acuity Scale for PediatricsPrince Jhessie L. AbellaPas encore d'évaluation
- Australian Model Triage ScaleDocument3 pagesAustralian Model Triage ScaleHendraDarmawanPas encore d'évaluation
- Hpcsa Booklet 2 Generic Ethical Rules With AnexuresDocument58 pagesHpcsa Booklet 2 Generic Ethical Rules With Anexuresapi-301960722Pas encore d'évaluation
- Somatosensory System OkDocument47 pagesSomatosensory System OkIrayumastutiPas encore d'évaluation
- prehospital-EMS-COVID-19-recommendations - 4.4Document19 pagesprehospital-EMS-COVID-19-recommendations - 4.4MEONEPas encore d'évaluation
- Arterial LineDocument2 pagesArterial LineRaghav Goyal100% (1)
- Musculoskeletal Exam Questions PortfolioDocument7 pagesMusculoskeletal Exam Questions Portfolioapi-360345296Pas encore d'évaluation
- Assisting A Tracheostomy ProcedureDocument2 pagesAssisting A Tracheostomy ProcedureMIKKI100% (2)
- Antituberculous Therapy in Special SituationsDocument8 pagesAntituberculous Therapy in Special SituationsMobeen Raza100% (1)
- Emergency Care for LVAD PatientsDocument23 pagesEmergency Care for LVAD PatientsVashish RamrechaPas encore d'évaluation
- GUIDELINE For IMPROVING OUTCOME After Anaesthesia and Critical Care - 2017 - College of AnaesthesiologistsDocument83 pagesGUIDELINE For IMPROVING OUTCOME After Anaesthesia and Critical Care - 2017 - College of AnaesthesiologistsSanj.etcPas encore d'évaluation
- Min Min Min Min: Most Urgent Very Urgent Urgent Less Urgent Not UrgentDocument1 pageMin Min Min Min: Most Urgent Very Urgent Urgent Less Urgent Not UrgentAlma Alnajjar0% (1)
- Severity Scoring Systems in The Critically IllDocument5 pagesSeverity Scoring Systems in The Critically Illdefitrananda100% (1)
- Endocarditis, Pericarditic, Myocarditis: TopicDocument104 pagesEndocarditis, Pericarditic, Myocarditis: TopicOM VERMAPas encore d'évaluation
- Hemodynamic Monitoring Techniques and Their Clinical ApplicationsDocument44 pagesHemodynamic Monitoring Techniques and Their Clinical Applicationsinvisigoth17Pas encore d'évaluation
- ICU Scoring Systems Guide OverviewDocument35 pagesICU Scoring Systems Guide OverviewVijay Gadagi100% (3)
- Discharge Summary FormatDocument14 pagesDischarge Summary Formatenumula kumarPas encore d'évaluation
- Deep Vein Thrombosis - 2003Document34 pagesDeep Vein Thrombosis - 2003farmasi_hm100% (1)
- Fat EmbolismDocument12 pagesFat EmbolismHastina HadnanPas encore d'évaluation
- Management of Status Asthmatic Us in ChildrenDocument7 pagesManagement of Status Asthmatic Us in Childrenjshq1971Pas encore d'évaluation
- Ensuring Optimal Crash Cart FunctionDocument11 pagesEnsuring Optimal Crash Cart FunctionKarren FernandezPas encore d'évaluation
- CPP - Primary and Secondary SurveyDocument6 pagesCPP - Primary and Secondary Survey一臣みちるPas encore d'évaluation
- CABG PresentationDocument55 pagesCABG Presentationnmaykanathan100% (7)
- Hospital: Ms .Neethu Vincent Asst Professor KVM College of NursingDocument29 pagesHospital: Ms .Neethu Vincent Asst Professor KVM College of NursingNeethu VincentPas encore d'évaluation
- RVT ATLS Review & General Principles in TraumaDocument91 pagesRVT ATLS Review & General Principles in TraumaRifqi NuriyPas encore d'évaluation
- Venous Air EmbolismDocument16 pagesVenous Air EmbolismEylia MelikaPas encore d'évaluation
- CPR - Cardiopulmonary ResuscitationDocument31 pagesCPR - Cardiopulmonary ResuscitationPanji HerlambangPas encore d'évaluation
- Siriraj 4Document3 pagesSiriraj 4Winda MelatiPas encore d'évaluation
- Stroke Score 2009Document6 pagesStroke Score 2009Pebrian SyahPas encore d'évaluation
- Acute Renal FailureDocument26 pagesAcute Renal FailureHendy SetiawanPas encore d'évaluation
- Management of AscitesDocument5 pagesManagement of AscitesHendy SetiawanPas encore d'évaluation
- Who 2006 Prevention of Postpartum HaemorrhageDocument121 pagesWho 2006 Prevention of Postpartum HaemorrhagekimmyraverPas encore d'évaluation
- Who 2006 Prevention of Postpartum HaemorrhageDocument121 pagesWho 2006 Prevention of Postpartum HaemorrhagekimmyraverPas encore d'évaluation
- Immediate Hypersensitivity ReactionsDocument8 pagesImmediate Hypersensitivity ReactionsHendy SetiawanPas encore d'évaluation
- Dysfunctional Uterine Bleeding CausesDocument15 pagesDysfunctional Uterine Bleeding CausesHendy SetiawanPas encore d'évaluation
- Immunotherapy For Sepsis - A New Approach Against An Ancient FoeDocument3 pagesImmunotherapy For Sepsis - A New Approach Against An Ancient FoeHendy SetiawanPas encore d'évaluation
- Icru 82Document67 pagesIcru 82Aditya DisdusPas encore d'évaluation
- Rulerships and Qualities Anatomy and Physiology Correlated To The ZodiacDocument4 pagesRulerships and Qualities Anatomy and Physiology Correlated To The Zodiactushar100% (1)
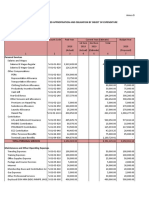
- Programmed Appropriation and Obligation by Object of ExpenditureDocument7 pagesProgrammed Appropriation and Obligation by Object of ExpenditureKristin Villaseñor-MercadoPas encore d'évaluation
- Can gray hair be donated for cancer wigsDocument1 pageCan gray hair be donated for cancer wigsDawa TsheringPas encore d'évaluation
- Cap 2019 04 01 PDFDocument58 pagesCap 2019 04 01 PDFRajeev PareekPas encore d'évaluation
- VaricoceleDocument3 pagesVaricoceleMandy ChengPas encore d'évaluation
- Light Pollution ImpactsDocument7 pagesLight Pollution ImpactsIqra Qazi100% (1)
- Rheumatoid ArthritisDocument15 pagesRheumatoid ArthritisPJHG100% (2)
- Dr. Nugroho Sigit SpRad PDFDocument20 pagesDr. Nugroho Sigit SpRad PDFMira HandayaniPas encore d'évaluation
- Interview With T.C. FryDocument18 pagesInterview With T.C. Fryraweater100% (1)
- OEC Chapter 1-5Document20 pagesOEC Chapter 1-5Phil McLeanPas encore d'évaluation
- Understanding Hiatal HerniaDocument37 pagesUnderstanding Hiatal HerniaRaju Shrestha100% (2)
- Odontogenic Tumours - (2) L5Document28 pagesOdontogenic Tumours - (2) L5nooraaaPas encore d'évaluation
- Course Work EssayDocument12 pagesCourse Work EssayKanza NajamPas encore d'évaluation
- CT BR SureSubtraction CT DSADocument11 pagesCT BR SureSubtraction CT DSAWALVRadiologyPas encore d'évaluation
- Hijama PointsDocument23 pagesHijama PointsShahbaz Ahmed100% (1)
- CASE PRESENTATION ANALYSISDocument45 pagesCASE PRESENTATION ANALYSISBasneyatPragyanPas encore d'évaluation
- Posted: Mon Jun 21, 2010 4:02 PM Post Subject: DENTAL MCQS: Previous Year PaperDocument16 pagesPosted: Mon Jun 21, 2010 4:02 PM Post Subject: DENTAL MCQS: Previous Year PaperMadhul Singhal100% (1)
- QIMP14 AppendixDocument12 pagesQIMP14 AppendixShahriar MostafaPas encore d'évaluation
- Interventional BronchosDocument323 pagesInterventional BronchosFranspol100% (1)
- Naked® JuiceDocument3 pagesNaked® Juicecxuser43211Pas encore d'évaluation
- Clinical guidelines for liver transplantationDocument53 pagesClinical guidelines for liver transplantationMadalina StoicescuPas encore d'évaluation
- Lista de Lucrari 3Document30 pagesLista de Lucrari 3Anonymous 0epuGwQTJPas encore d'évaluation
- Alcoholism among Malaysian YouthDocument8 pagesAlcoholism among Malaysian YouthsuemePas encore d'évaluation
- Gestational Trophoblastic DiseaseDocument40 pagesGestational Trophoblastic DiseaseAayupta Mohanty100% (2)
- Filipino Pancit Bihon P20.00: Main CourseDocument16 pagesFilipino Pancit Bihon P20.00: Main CourseElaine AustriaPas encore d'évaluation
- Newly Diagnosed GlioblastomaDocument30 pagesNewly Diagnosed GlioblastomaJubairPas encore d'évaluation
- Clinical Summary Guide 05Document2 pagesClinical Summary Guide 05Diarti_PMIKPas encore d'évaluation
- Comparing Chronological, Cause-Effect, and Compare-Contrast OrdersDocument3 pagesComparing Chronological, Cause-Effect, and Compare-Contrast OrdersIpha BadjaPas encore d'évaluation
- Clinical Study Baccharis Dracunculifolia As Agent For The Control of BiofilmDocument7 pagesClinical Study Baccharis Dracunculifolia As Agent For The Control of BiofilmimamaptPas encore d'évaluation