Vous aimerez peut-être aussi
- Grit: The Power of Passion and PerseveranceD'EverandGrit: The Power of Passion and PerseveranceÉvaluation : 4 sur 5 étoiles4/5 (588)
- The Yellow House: A Memoir (2019 National Book Award Winner)D'EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Évaluation : 4 sur 5 étoiles4/5 (98)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeD'EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeÉvaluation : 4 sur 5 étoiles4/5 (5795)
- Never Split the Difference: Negotiating As If Your Life Depended On ItD'EverandNever Split the Difference: Negotiating As If Your Life Depended On ItÉvaluation : 4.5 sur 5 étoiles4.5/5 (838)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceD'EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceÉvaluation : 4 sur 5 étoiles4/5 (895)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersD'EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersÉvaluation : 4.5 sur 5 étoiles4.5/5 (345)
- Shoe Dog: A Memoir by the Creator of NikeD'EverandShoe Dog: A Memoir by the Creator of NikeÉvaluation : 4.5 sur 5 étoiles4.5/5 (537)
- The Little Book of Hygge: Danish Secrets to Happy LivingD'EverandThe Little Book of Hygge: Danish Secrets to Happy LivingÉvaluation : 3.5 sur 5 étoiles3.5/5 (400)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureD'EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureÉvaluation : 4.5 sur 5 étoiles4.5/5 (474)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryD'EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryÉvaluation : 3.5 sur 5 étoiles3.5/5 (231)
- On Fire: The (Burning) Case for a Green New DealD'EverandOn Fire: The (Burning) Case for a Green New DealÉvaluation : 4 sur 5 étoiles4/5 (74)
- The Emperor of All Maladies: A Biography of CancerD'EverandThe Emperor of All Maladies: A Biography of CancerÉvaluation : 4.5 sur 5 étoiles4.5/5 (271)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaD'EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaÉvaluation : 4.5 sur 5 étoiles4.5/5 (266)
- The Unwinding: An Inner History of the New AmericaD'EverandThe Unwinding: An Inner History of the New AmericaÉvaluation : 4 sur 5 étoiles4/5 (45)
- Team of Rivals: The Political Genius of Abraham LincolnD'EverandTeam of Rivals: The Political Genius of Abraham LincolnÉvaluation : 4.5 sur 5 étoiles4.5/5 (234)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyD'EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyÉvaluation : 3.5 sur 5 étoiles3.5/5 (2259)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreD'EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreÉvaluation : 4 sur 5 étoiles4/5 (1091)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)D'EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Évaluation : 4.5 sur 5 étoiles4.5/5 (121)
- Her Body and Other Parties: StoriesD'EverandHer Body and Other Parties: StoriesÉvaluation : 4 sur 5 étoiles4/5 (821)
- Computational BioengineeringDocument480 pagesComputational Bioengineeringscribd990Pas encore d'évaluation
- Endocrine 50 Questions & AnswersDocument28 pagesEndocrine 50 Questions & AnswersBrooke Susac100% (1)
- Medical Management of in Children: A Delphi Consensus: BlepharokeratoconjunctivitisDocument8 pagesMedical Management of in Children: A Delphi Consensus: Blepharokeratoconjunctivitisriskab123Pas encore d'évaluation
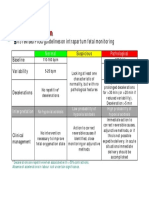
- CTG Classification PDFDocument1 pageCTG Classification PDFganotPas encore d'évaluation
- Dorn Method Certification CourseDocument10 pagesDorn Method Certification Coursejpepe100% (1)
- Adv For CounselorDocument2 pagesAdv For CounselorRashmi RanjanPas encore d'évaluation
- Para Instwise Adm Af Reporting Cancel r1Document639 pagesPara Instwise Adm Af Reporting Cancel r1Rutvik DhoriyaPas encore d'évaluation
- Portfolio ResumeDocument2 pagesPortfolio Resumeapi-658308760Pas encore d'évaluation
- FeverDocument45 pagesFeverAsish Geiorge100% (1)
- Welcome Letter For FamiliesDocument3 pagesWelcome Letter For FamiliesChild and Family InstitutePas encore d'évaluation
- AAA Mixed Pain SMGDocument37 pagesAAA Mixed Pain SMGandhita96Pas encore d'évaluation
- Management of Diabetes: DR Rukman Mecca M I 51 ST Batch Calicut Med CollegeDocument47 pagesManagement of Diabetes: DR Rukman Mecca M I 51 ST Batch Calicut Med CollegeRukman MeccaPas encore d'évaluation
- Ilase UM PDFDocument31 pagesIlase UM PDFVijay Prabu GPas encore d'évaluation
- Opioid AnalgesicDocument43 pagesOpioid AnalgesicAnanta MiaPas encore d'évaluation
- BandurasTheory PDFDocument23 pagesBandurasTheory PDFJohncarlo DungogPas encore d'évaluation
- Psychology - Article 38Document1 pagePsychology - Article 38piping stressPas encore d'évaluation
- Abg Case StudiesDocument22 pagesAbg Case StudiesMaria DalalPas encore d'évaluation
- Diagnosis of Iron-Deficiency Anemia in The ElderlyDocument3 pagesDiagnosis of Iron-Deficiency Anemia in The ElderlyGeranyl LaguardiaPas encore d'évaluation
- Intravenous Fluid Guideline-1Document4 pagesIntravenous Fluid Guideline-1Marco CalvaraPas encore d'évaluation
- Kasus AsmaDocument5 pagesKasus AsmaHananun Zharfa0% (3)
- Grandjean 2000Document13 pagesGrandjean 2000Ivan VeriswanPas encore d'évaluation
- Surgical Drains Catheters and Tubes (M)Document120 pagesSurgical Drains Catheters and Tubes (M)nikprov100% (6)
- Anti AcidsDocument8 pagesAnti AcidsMohammad Ali Abu Ma'ashPas encore d'évaluation
- Malaria ModulDocument18 pagesMalaria ModulcheiwinarnoPas encore d'évaluation
- Data StokDocument26 pagesData StokUlfhey ChupidPas encore d'évaluation
- The Truth About ReikiDocument6 pagesThe Truth About ReikiM RezaPas encore d'évaluation
- Level 1: Healing Touch Certificate ProgramDocument2 pagesLevel 1: Healing Touch Certificate Programapi-25955699Pas encore d'évaluation
- Psychiatric MisadventuresDocument10 pagesPsychiatric MisadventuresRob_212Pas encore d'évaluation
- Trans CounselingDocument71 pagesTrans CounselingMolly GumPas encore d'évaluation
- Health Teaching PlanDocument4 pagesHealth Teaching PlanRene John Francisco80% (5)