Vous aimerez peut-être aussi
- Families, Friends & CarersDocument32 pagesFamilies, Friends & Carersmick.pride81Pas encore d'évaluation
- Article Taming The Terrible MomentsDocument3 pagesArticle Taming The Terrible Momentsapi-232349586Pas encore d'évaluation
- Oxford Handbooks Online: Intellectual DisabilitiesDocument20 pagesOxford Handbooks Online: Intellectual DisabilitiesCristina100% (1)
- Autism Physician Handbook: Dr. Wendy EdwardsDocument40 pagesAutism Physician Handbook: Dr. Wendy EdwardsLoptus100% (1)
- Frustrated, Overlooked and Excluded: How People With Disabilities Have Been Feeling During The COVID-19 PandemicDocument15 pagesFrustrated, Overlooked and Excluded: How People With Disabilities Have Been Feeling During The COVID-19 PandemicCOUCH HealthPas encore d'évaluation
- Psych Final Exam Study GuideDocument15 pagesPsych Final Exam Study Guidecsuhajda97Pas encore d'évaluation
- Speech On How To Foster A Great RelationshipDocument4 pagesSpeech On How To Foster A Great RelationshipBlack Tirah TirahPas encore d'évaluation
- Module 22-Motivational InterviewingDocument23 pagesModule 22-Motivational InterviewingmelodyfathiPas encore d'évaluation
- Management of Childhood and Adolescent DisordersDocument26 pagesManagement of Childhood and Adolescent Disordersdurgesh yadav100% (1)
- Analysis of The Motion Picture "Babies"Document7 pagesAnalysis of The Motion Picture "Babies"Immanuel Greene60% (5)
- Personality Development EmotionsDocument13 pagesPersonality Development EmotionsMae-maeGarmaPas encore d'évaluation
- 4 Foundations To Help Trauma-Impacted YouthDocument4 pages4 Foundations To Help Trauma-Impacted YouthwaleskacrzPas encore d'évaluation
- Peer PowerDocument74 pagesPeer PowerThe Centre for Welfare Reform100% (1)
- Development and validation of the General Activities of Daily Living ScaleDocument10 pagesDevelopment and validation of the General Activities of Daily Living ScaleCarlos Eduardo NortePas encore d'évaluation
- Home and Community Based Services Made Simple: A Quick Reference Guide to Creating a Successful and Sustainable ProgramD'EverandHome and Community Based Services Made Simple: A Quick Reference Guide to Creating a Successful and Sustainable ProgramPas encore d'évaluation
- Young Children PDFDocument8 pagesYoung Children PDFfotinimavr94Pas encore d'évaluation
- Welcome Letter For FamiliesDocument3 pagesWelcome Letter For FamiliesChild and Family InstitutePas encore d'évaluation
- Dissertation FinalDocument61 pagesDissertation FinalDedipya ImmadisettyPas encore d'évaluation
- The Child Bipolar QuestionnaireDocument10 pagesThe Child Bipolar QuestionnairefranciscatomiPas encore d'évaluation
- Psychological First AidDocument81 pagesPsychological First AidJay Mark BibosoPas encore d'évaluation
- Promoting Healthy Aging by Confronting AgeismDocument7 pagesPromoting Healthy Aging by Confronting AgeismJuanito MaravillasPas encore d'évaluation
- Interventions For Classroom DisruptionDocument54 pagesInterventions For Classroom DisruptionnosunarPas encore d'évaluation
- Professional Meeting Reflective Journal-2Document3 pagesProfessional Meeting Reflective Journal-2api-399086837Pas encore d'évaluation
- Learn about your strengths and areas for growth with the JOHARI Window modelDocument6 pagesLearn about your strengths and areas for growth with the JOHARI Window modelAndrea Torres VicentPas encore d'évaluation
- Healing Through PlayDocument2 pagesHealing Through PlayEunice KhainzaPas encore d'évaluation
- Solution Focused Counseling With Nvoluntary ClientsDocument13 pagesSolution Focused Counseling With Nvoluntary ClientsJuanaPas encore d'évaluation
- Gottfredson's TheoryDocument44 pagesGottfredson's TheoryAinnur Nurul Aini Mudayat100% (3)
- Activities of Living PatientDocument5 pagesActivities of Living PatientclaudiaPas encore d'évaluation
- Chapter 20 - Culturally Adaptive InterviewingDocument94 pagesChapter 20 - Culturally Adaptive InterviewingNaomi LiangPas encore d'évaluation
- Family Dynamics and CoachingDocument17 pagesFamily Dynamics and Coachingberman_adamPas encore d'évaluation
- SLCS RDocument2 pagesSLCS RdanieljohnarboledaPas encore d'évaluation
- Theory Interpersonal RelationshipDocument40 pagesTheory Interpersonal RelationshipBheru LalPas encore d'évaluation
- G8-Health-Q2-LM-Family Health IIDocument71 pagesG8-Health-Q2-LM-Family Health IIJohn Nomerson B. GumbaPas encore d'évaluation
- Family Empowerment ScaleDocument9 pagesFamily Empowerment ScaleNeneng VitriyahPas encore d'évaluation
- Guidelines For Evaluation of Permanent ImpairmentDocument106 pagesGuidelines For Evaluation of Permanent ImpairmentJorge MartinsPas encore d'évaluation
- Group Counselling With ChildrenDocument33 pagesGroup Counselling With ChildrenMariyya Muzaffar JanjuaPas encore d'évaluation
- For Emma Draft Preplanning Template For Discharge With Ndis SupportDocument6 pagesFor Emma Draft Preplanning Template For Discharge With Ndis Supportapi-336687121Pas encore d'évaluation
- Referral Checklist for 6-Year-OldsDocument1 pageReferral Checklist for 6-Year-Oldsmarkus_danusantosoPas encore d'évaluation
- ARMIDILO-G Full Info Pack For Support Staff With Consent To Research Nov 2012Document19 pagesARMIDILO-G Full Info Pack For Support Staff With Consent To Research Nov 2012JessicaPas encore d'évaluation
- First Friday Presentation 2 3 23Document60 pagesFirst Friday Presentation 2 3 23api-339789222Pas encore d'évaluation
- Sample Literature Review - PsychologyDocument9 pagesSample Literature Review - Psychologyapi-242012614Pas encore d'évaluation
- Instrumental Activities of Daily LivingDocument3 pagesInstrumental Activities of Daily LivingAndrzej KlimczukPas encore d'évaluation
- Ethical DilemaDocument9 pagesEthical Dilemadavid proctorPas encore d'évaluation
- Self-Awareness Strategies for TeachersDocument22 pagesSelf-Awareness Strategies for TeachersKatheryne100% (1)
- Depression Children PDFDocument2 pagesDepression Children PDFConstanzaPas encore d'évaluation
- The Children's Eating Behavior InventoryDocument14 pagesThe Children's Eating Behavior Inventoryguilherme augusto paroPas encore d'évaluation
- Infant and Early Childhood Mental Health Core Concepts and Clinical Practice by Kristie Brandt Bruce D. Perry Stephen Seligman Ed TronickDocument382 pagesInfant and Early Childhood Mental Health Core Concepts and Clinical Practice by Kristie Brandt Bruce D. Perry Stephen Seligman Ed TronickRucsandra MurzeaPas encore d'évaluation
- L5 Children With Emotional or Behavioral DisorderDocument24 pagesL5 Children With Emotional or Behavioral DisorderAGLDPas encore d'évaluation
- Filipino Mothers' Disciplinary PracticesDocument10 pagesFilipino Mothers' Disciplinary PracticesEthel M. Lagustan- MorenoPas encore d'évaluation
- Supporting SiblingsDocument55 pagesSupporting Siblingsapi-247396878Pas encore d'évaluation
- Suicidal Ideation Risk Assessment: Steps and Resources For Exploring Thoughts of SuicideDocument12 pagesSuicidal Ideation Risk Assessment: Steps and Resources For Exploring Thoughts of SuicideShreeya GhagPas encore d'évaluation
- Guia - AdolescentesDocument6 pagesGuia - AdolescentesCentro De Psicoterapia Condesa100% (1)
- Parenting A Child With Special NeedsDocument16 pagesParenting A Child With Special NeedsShiang LinPas encore d'évaluation
- Autism Spectrum and Open-MindednessDocument2 pagesAutism Spectrum and Open-MindednessJaime MontoyaPas encore d'évaluation
- The Supervisory Relationship Questionnaire (SRQ)Document3 pagesThe Supervisory Relationship Questionnaire (SRQ)kartutePas encore d'évaluation
- Alexander2010 (Fase Terapi)Document27 pagesAlexander2010 (Fase Terapi)astri100% (1)
- The Effects of Emotional Intelligence On Job Performance and LifeDocument37 pagesThe Effects of Emotional Intelligence On Job Performance and LifeXihomara AvilaPas encore d'évaluation
- The ROI of Mental Wellness in the Workplace: Why It's Necessary to Boost Employee ProductivityD'EverandThe ROI of Mental Wellness in the Workplace: Why It's Necessary to Boost Employee ProductivityPas encore d'évaluation
- Collaborative Problem Solving Group A Complete Guide - 2020 EditionD'EverandCollaborative Problem Solving Group A Complete Guide - 2020 EditionPas encore d'évaluation
- Hidden Disabilities and Conditions: Creating an Inclusive WorkplaceD'EverandHidden Disabilities and Conditions: Creating an Inclusive WorkplacePas encore d'évaluation
- Why Collective Bargaining Should Be Made Possible, Especially For The Public Sector in Zimbabwe. DiscussDocument6 pagesWhy Collective Bargaining Should Be Made Possible, Especially For The Public Sector in Zimbabwe. DiscussWinnie MugovaPas encore d'évaluation
- House Bill 1016Document11 pagesHouse Bill 1016Herman ClederaPas encore d'évaluation
- Opening ChecklistDocument75 pagesOpening Checklistsujay13780100% (1)
- CSR 2010Document499 pagesCSR 2010Daljeet Sidhu70% (10)
- Registration Number: SecunderabadDocument2 pagesRegistration Number: SecunderabadmANOHARPas encore d'évaluation
- 2022 07 27 - 2022 Review of Electronic Communications Sector Consultation Document - FINALDocument33 pages2022 07 27 - 2022 Review of Electronic Communications Sector Consultation Document - FINALBernewsAdminPas encore d'évaluation
- Tef French Exam Preparation: Course DescriptionDocument2 pagesTef French Exam Preparation: Course DescriptionFido DidoPas encore d'évaluation
- Grounds For Eviction of TenantDocument49 pagesGrounds For Eviction of TenantRajivSmithPas encore d'évaluation
- Introduction To Globalization PPTDocument24 pagesIntroduction To Globalization PPTrose belle garcia100% (1)
- CH 15Document72 pagesCH 15Debora Silvyana ManaluPas encore d'évaluation
- Bar Prep - Outline - Trusts - ShortDocument7 pagesBar Prep - Outline - Trusts - ShortAnonymous Cbr8Vr2SX100% (1)
- Casestudyb 1rDocument7 pagesCasestudyb 1rapi-497060945100% (1)
- Exercise - Mixed TensesDocument2 pagesExercise - Mixed TensesКсюша КривцунPas encore d'évaluation
- History 1200-1700Document238 pagesHistory 1200-1700surbhi prajapati86% (7)
- Magna Financial Services Group Cannot Foreclose Chattel Mortgage and Claim Unpaid BalanceDocument1 pageMagna Financial Services Group Cannot Foreclose Chattel Mortgage and Claim Unpaid BalanceJohn Rhil RamosPas encore d'évaluation
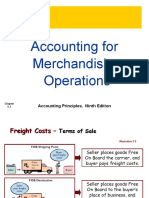
- Accounting For Merchandising Operations: Accounting Principles, Ninth EditionDocument17 pagesAccounting For Merchandising Operations: Accounting Principles, Ninth EditionMehedi HasanPas encore d'évaluation
- Examination 2011 General English Xiith Time: 3 Hrs. M.M. 100 InstructionsDocument16 pagesExamination 2011 General English Xiith Time: 3 Hrs. M.M. 100 InstructionsDeepak SewkaniPas encore d'évaluation
- Strategic Intellectual Capital Management in Multinational Organizations Sustainability and Successful ImplicationsDocument358 pagesStrategic Intellectual Capital Management in Multinational Organizations Sustainability and Successful Implicationsbiscodyl0% (1)
- The Kenite HypothesisDocument16 pagesThe Kenite Hypothesisشريف السركي100% (2)
- FijiTimes - March 1Document48 pagesFijiTimes - March 1fijitimescanadaPas encore d'évaluation
- DepEd Isabela Waiver Form for Student Press ConferenceDocument2 pagesDepEd Isabela Waiver Form for Student Press ConferenceJessa Mae Magday Nugal100% (1)
- Bulletin For Virtual Worship ServiceDocument8 pagesBulletin For Virtual Worship ServiceChrist Church OfficePas encore d'évaluation
- Understanding Power Dynamics and Developing Political ExpertiseDocument29 pagesUnderstanding Power Dynamics and Developing Political Expertisealessiacon100% (1)
- Declaration Acknowledgement Slip for Shahzad HaiderDocument2 pagesDeclaration Acknowledgement Slip for Shahzad HaiderShehzad HaiderPas encore d'évaluation
- SOP - Guidelines For Conducting F&B Service MeetingsDocument2 pagesSOP - Guidelines For Conducting F&B Service MeetingsHusam MohamedPas encore d'évaluation
- Central Europe Phrasebook 3 Czech v1 m56577569830517707Document21 pagesCentral Europe Phrasebook 3 Czech v1 m56577569830517707Raman GoyalPas encore d'évaluation
- Ethiopian History SeeDocument240 pagesEthiopian History Seetilahunthm100% (1)
- 942 3 Boo - Com Case StudyDocument5 pages942 3 Boo - Com Case Studybulajica100% (1)
- Resume-Vinit KhuranaDocument4 pagesResume-Vinit KhuranaabhishekatupesPas encore d'évaluation
- Quimiging vs. Icao, 1970 - Personality of Conceived ChildDocument4 pagesQuimiging vs. Icao, 1970 - Personality of Conceived ChildhenzencameroPas encore d'évaluation