Vous aimerez peut-être aussi
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryD'EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryÉvaluation : 3.5 sur 5 étoiles3.5/5 (231)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)D'EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Évaluation : 4.5 sur 5 étoiles4.5/5 (121)
- Grit: The Power of Passion and PerseveranceD'EverandGrit: The Power of Passion and PerseveranceÉvaluation : 4 sur 5 étoiles4/5 (588)
- Never Split the Difference: Negotiating As If Your Life Depended On ItD'EverandNever Split the Difference: Negotiating As If Your Life Depended On ItÉvaluation : 4.5 sur 5 étoiles4.5/5 (838)
- The Little Book of Hygge: Danish Secrets to Happy LivingD'EverandThe Little Book of Hygge: Danish Secrets to Happy LivingÉvaluation : 3.5 sur 5 étoiles3.5/5 (400)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaD'EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaÉvaluation : 4.5 sur 5 étoiles4.5/5 (266)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeD'EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeÉvaluation : 4 sur 5 étoiles4/5 (5794)
- Her Body and Other Parties: StoriesD'EverandHer Body and Other Parties: StoriesÉvaluation : 4 sur 5 étoiles4/5 (821)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreD'EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreÉvaluation : 4 sur 5 étoiles4/5 (1090)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyD'EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyÉvaluation : 3.5 sur 5 étoiles3.5/5 (2259)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersD'EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersÉvaluation : 4.5 sur 5 étoiles4.5/5 (345)
- Shoe Dog: A Memoir by the Creator of NikeD'EverandShoe Dog: A Memoir by the Creator of NikeÉvaluation : 4.5 sur 5 étoiles4.5/5 (537)
- The Emperor of All Maladies: A Biography of CancerD'EverandThe Emperor of All Maladies: A Biography of CancerÉvaluation : 4.5 sur 5 étoiles4.5/5 (271)
- Team of Rivals: The Political Genius of Abraham LincolnD'EverandTeam of Rivals: The Political Genius of Abraham LincolnÉvaluation : 4.5 sur 5 étoiles4.5/5 (234)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceD'EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceÉvaluation : 4 sur 5 étoiles4/5 (895)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureD'EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureÉvaluation : 4.5 sur 5 étoiles4.5/5 (474)
- On Fire: The (Burning) Case for a Green New DealD'EverandOn Fire: The (Burning) Case for a Green New DealÉvaluation : 4 sur 5 étoiles4/5 (74)
- The Yellow House: A Memoir (2019 National Book Award Winner)D'EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Évaluation : 4 sur 5 étoiles4/5 (98)
- Best Aid To Orthopedics PDFDocument586 pagesBest Aid To Orthopedics PDFDNDTPas encore d'évaluation
- The Unwinding: An Inner History of the New AmericaD'EverandThe Unwinding: An Inner History of the New AmericaÉvaluation : 4 sur 5 étoiles4/5 (45)
- Lecture Notes On Orthopaedics and Fractures PDFDocument257 pagesLecture Notes On Orthopaedics and Fractures PDFDanny Irung0% (1)
- Fracture Classifications in Clinical Practice PDFDocument132 pagesFracture Classifications in Clinical Practice PDFAkbar Khan100% (1)
- Muscles of The ScapulaDocument6 pagesMuscles of The ScapulaAndika Anjani AgustinPas encore d'évaluation
- George MCQ 2010Document9 pagesGeorge MCQ 2010Mohamad RamadanPas encore d'évaluation
- Caldwell Luc - Radical Antrostomy - Procedure Canine Fossa and Inferior Meatal Puncture and Inferior Meatal AntrostomyDocument13 pagesCaldwell Luc - Radical Antrostomy - Procedure Canine Fossa and Inferior Meatal Puncture and Inferior Meatal AntrostomyAlexi Chávez EchevarríaPas encore d'évaluation
- MilwaukeeDocument24 pagesMilwaukeeRiaz UddinPas encore d'évaluation
- Calcaneal FractureDocument34 pagesCalcaneal Fracturemmm.orthoPas encore d'évaluation
- 2023 JOT Low Transcondylar Fractures of The Distal Humerus - A Multicenter Cohort StudyDocument6 pages2023 JOT Low Transcondylar Fractures of The Distal Humerus - A Multicenter Cohort StudyjcmarecauxlPas encore d'évaluation
- 02 The Nose and The Associated StructuresDocument72 pages02 The Nose and The Associated Structuresmalaths757Pas encore d'évaluation
- Lateral Condylar Fracture in ChildrenDocument19 pagesLateral Condylar Fracture in ChildrenMuhammed Muzzammil SanganiPas encore d'évaluation
- Ecz Grade 10 - 12 Biology Summarised Notes (Locomotion and The Skeleton) With Exam Questions and AnswersDocument15 pagesEcz Grade 10 - 12 Biology Summarised Notes (Locomotion and The Skeleton) With Exam Questions and AnswersItx Jones100% (1)
- Ankle AnatomyDocument59 pagesAnkle AnatomyAsmat Ullah QureshiPas encore d'évaluation
- Histology of Cartilage & Bone: DR Punita Manik Department of Anatomy K G Medical Univesity U P LucknowDocument61 pagesHistology of Cartilage & Bone: DR Punita Manik Department of Anatomy K G Medical Univesity U P LucknowbeylaPas encore d'évaluation
- Brace Modifications That Can Result in Improved Curve Correction in Idiopathic ScoliosisDocument7 pagesBrace Modifications That Can Result in Improved Curve Correction in Idiopathic ScoliosisjeanPas encore d'évaluation
- Morning Report: Pembimbing: Dr. Djunifer Hasudungan Sagala, Sp. OT (K) Dr. Andreas Wahyu W, Sp. OTDocument55 pagesMorning Report: Pembimbing: Dr. Djunifer Hasudungan Sagala, Sp. OT (K) Dr. Andreas Wahyu W, Sp. OTSinda AgathaPas encore d'évaluation
- Spine SurgeryDocument10 pagesSpine Surgerymarismith23Pas encore d'évaluation
- Human Anatomy and Physiology Laboratory Manual Fetal Pig Version 12Th Edition Marieb Solutions Manual Full Chapter PDFDocument29 pagesHuman Anatomy and Physiology Laboratory Manual Fetal Pig Version 12Th Edition Marieb Solutions Manual Full Chapter PDFAlexandraPerrymzyd100% (10)
- Lig Hyrtl+Porul Crotaphitico-BuccinatorDocument4 pagesLig Hyrtl+Porul Crotaphitico-BuccinatorMatei HerminaPas encore d'évaluation
- Anatomy & Physiology: Essentials ofDocument93 pagesAnatomy & Physiology: Essentials ofRamzen Raphael DomingoPas encore d'évaluation
- Anatomy Final All Questions (New)Document175 pagesAnatomy Final All Questions (New)Sevval OzcelikPas encore d'évaluation
- The HandDocument4 pagesThe HandRoland Garcia Pelagio Jr.Pas encore d'évaluation
- Desarrollo de La Enf. Segmento ADYACENTE.2006: March 2014Document9 pagesDesarrollo de La Enf. Segmento ADYACENTE.2006: March 2014J Alan SantosPas encore d'évaluation
- Prosthetic 7Document3 pagesProsthetic 7زهراء فاضل اجبير فعيلPas encore d'évaluation
- Spinal Disc HerniationDocument5 pagesSpinal Disc HerniationJoshua Hong100% (1)
- Baumgaertner. The Value of The Tip-Apex Distance PDFDocument8 pagesBaumgaertner. The Value of The Tip-Apex Distance PDFIcaruscignusPas encore d'évaluation
- Henry Vernon Crock M.D., M.S., F.R.C.S., F.R.A.C.S. (Auth.) - Practice of Spinal Surgery-Springer Vienna (1983) PDFDocument334 pagesHenry Vernon Crock M.D., M.S., F.R.C.S., F.R.A.C.S. (Auth.) - Practice of Spinal Surgery-Springer Vienna (1983) PDFIonut VladPas encore d'évaluation
- Tumor Flash Cards - Osteochondroma and Multiple Hereditary ExostosisDocument23 pagesTumor Flash Cards - Osteochondroma and Multiple Hereditary Exostosislaxge54Pas encore d'évaluation
- Osteologie CraniuDocument94 pagesOsteologie Craniualiss0410Pas encore d'évaluation
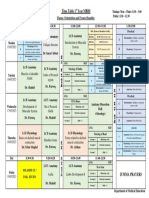
- Timetable 1st Year MBBS MSK Module Week 2Document1 pageTimetable 1st Year MBBS MSK Module Week 2UZAIR KHANPas encore d'évaluation