Vous aimerez peut-être aussi
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceD'EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceÉvaluation : 4 sur 5 étoiles4/5 (895)
- Never Split the Difference: Negotiating As If Your Life Depended On ItD'EverandNever Split the Difference: Negotiating As If Your Life Depended On ItÉvaluation : 4.5 sur 5 étoiles4.5/5 (838)
- The Yellow House: A Memoir (2019 National Book Award Winner)D'EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Évaluation : 4 sur 5 étoiles4/5 (98)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeD'EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeÉvaluation : 4 sur 5 étoiles4/5 (5794)
- Shoe Dog: A Memoir by the Creator of NikeD'EverandShoe Dog: A Memoir by the Creator of NikeÉvaluation : 4.5 sur 5 étoiles4.5/5 (537)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaD'EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaÉvaluation : 4.5 sur 5 étoiles4.5/5 (266)
- The Little Book of Hygge: Danish Secrets to Happy LivingD'EverandThe Little Book of Hygge: Danish Secrets to Happy LivingÉvaluation : 3.5 sur 5 étoiles3.5/5 (400)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureD'EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureÉvaluation : 4.5 sur 5 étoiles4.5/5 (474)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryD'EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryÉvaluation : 3.5 sur 5 étoiles3.5/5 (231)
- Grit: The Power of Passion and PerseveranceD'EverandGrit: The Power of Passion and PerseveranceÉvaluation : 4 sur 5 étoiles4/5 (588)
- The Emperor of All Maladies: A Biography of CancerD'EverandThe Emperor of All Maladies: A Biography of CancerÉvaluation : 4.5 sur 5 étoiles4.5/5 (271)
- The Unwinding: An Inner History of the New AmericaD'EverandThe Unwinding: An Inner History of the New AmericaÉvaluation : 4 sur 5 étoiles4/5 (45)
- On Fire: The (Burning) Case for a Green New DealD'EverandOn Fire: The (Burning) Case for a Green New DealÉvaluation : 4 sur 5 étoiles4/5 (74)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersD'EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersÉvaluation : 4.5 sur 5 étoiles4.5/5 (344)
- Team of Rivals: The Political Genius of Abraham LincolnD'EverandTeam of Rivals: The Political Genius of Abraham LincolnÉvaluation : 4.5 sur 5 étoiles4.5/5 (234)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreD'EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreÉvaluation : 4 sur 5 étoiles4/5 (1090)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyD'EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyÉvaluation : 3.5 sur 5 étoiles3.5/5 (2259)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)D'EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Évaluation : 4.5 sur 5 étoiles4.5/5 (121)
- Her Body and Other Parties: StoriesD'EverandHer Body and Other Parties: StoriesÉvaluation : 4 sur 5 étoiles4/5 (821)
- Systemic BacteriologyDocument495 pagesSystemic BacteriologyAkash KaranwalPas encore d'évaluation
- National Guideline For Laboratory Sample Referral System HLS WEB Version 1Document80 pagesNational Guideline For Laboratory Sample Referral System HLS WEB Version 1Mkaruka BrellaPas encore d'évaluation
- GeneXpert SOP Xpert Processing EPTB Specimens DRAFTDocument7 pagesGeneXpert SOP Xpert Processing EPTB Specimens DRAFTFitra lestari100% (1)
- DPR Taluk Hospital NeelashwaramDocument17 pagesDPR Taluk Hospital NeelashwaramsunojPas encore d'évaluation
- X-Ray Architecture (Beatriz Colomina)Document201 pagesX-Ray Architecture (Beatriz Colomina)Rocio Marisol Torres100% (1)
- Pedia Revalida ReviewDocument83 pagesPedia Revalida Reviewcbac1990Pas encore d'évaluation
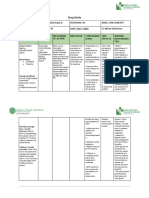
- Drug Study PDFDocument14 pagesDrug Study PDFsretirado02Pas encore d'évaluation
- Death DefeatedDocument234 pagesDeath DefeatedyurilenkoPas encore d'évaluation
- PDF TextDocument2 pagesPDF TextSATYAM KANNAUJPas encore d'évaluation
- 100 Item MEDICAL SURGICAL Nursing ExaminationDocument15 pages100 Item MEDICAL SURGICAL Nursing Examinationalexis_borjPas encore d'évaluation
- Common Pediatric Cases in OpdDocument90 pagesCommon Pediatric Cases in OpdJamie Sebastian100% (3)
- Q3-DLL HEALTH 8 - Wk1Document11 pagesQ3-DLL HEALTH 8 - Wk1Krizelle Mae DublaPas encore d'évaluation
- Medical Surgical Nursing Exams BoardDocument36 pagesMedical Surgical Nursing Exams BoardCINDY� BELMESPas encore d'évaluation
- Conflicts Clarify 1951Document754 pagesConflicts Clarify 1951FraterPrieriusPas encore d'évaluation
- 2.1 Medical Surgical Nursing - I Papers QPDocument15 pages2.1 Medical Surgical Nursing - I Papers QPAnju KarunakaranPas encore d'évaluation
- Buchanan 2015Document9 pagesBuchanan 2015cuplikan buola duniaaPas encore d'évaluation
- Case Scenario Mohsen SaadDocument6 pagesCase Scenario Mohsen SaadIbrahim HemdanPas encore d'évaluation
- Gambaran Radiologi TuberkulosisDocument36 pagesGambaran Radiologi TuberkulosisNathania PutriPas encore d'évaluation
- Diseases Caused by Bacteria, Viruses, and Nematodes and OthersDocument748 pagesDiseases Caused by Bacteria, Viruses, and Nematodes and OthersNeha UpadhyayPas encore d'évaluation
- Germ Vs Cellular Theory PDFDocument37 pagesGerm Vs Cellular Theory PDFpaulxe100% (3)
- Pediatrics Mock Board QuestionnaireDocument14 pagesPediatrics Mock Board Questionnairejampogaott100% (1)
- TubercolosisDocument8 pagesTubercolosisNitesh Bhura100% (1)
- Shaykkh Shahbaaz Project PPT Zeroth ReviewDocument13 pagesShaykkh Shahbaaz Project PPT Zeroth ReviewShaykkh ShahbaawzPas encore d'évaluation
- PresentasiDocument30 pagesPresentasiagusPas encore d'évaluation
- IGRA Vs PPDDocument9 pagesIGRA Vs PPDrafaelreanoPas encore d'évaluation
- Hiv Guidelines April 2018-2 PDFDocument195 pagesHiv Guidelines April 2018-2 PDFmpiirwe ramadhanPas encore d'évaluation
- Q3-Health-D3 CotDocument4 pagesQ3-Health-D3 CotDennis MartinezPas encore d'évaluation
- Pathogens: A Reconsideration of Koch's Sequence-Based Identification of MicrobialDocument17 pagesPathogens: A Reconsideration of Koch's Sequence-Based Identification of MicrobialGilbert Dela Serna MurilloPas encore d'évaluation
- Meier Et Al, 1996Document4 pagesMeier Et Al, 1996boni_sebayangPas encore d'évaluation