Vous aimerez peut-être aussi
- Thorax and Lungs AssessmentDocument28 pagesThorax and Lungs AssessmentMiden AlbanoPas encore d'évaluation
- Bag Technique: Name: Angeline M. Taghap Grade: Year and Section: BSN 2 B DateDocument11 pagesBag Technique: Name: Angeline M. Taghap Grade: Year and Section: BSN 2 B DateAngeline TaghapPas encore d'évaluation
- Shampooing Hair in BedDocument2 pagesShampooing Hair in BedDuchess Juliane Jose Mirambel100% (1)
- MMDSTDocument2 pagesMMDSTJulie Ann Gamboa EwicanPas encore d'évaluation
- Thorax and Lungs Assessment ChecklistDocument8 pagesThorax and Lungs Assessment ChecklistXing-Jin RomeroPas encore d'évaluation
- Manaois - SPIRITUALITY IN NURSING QUIZDocument3 pagesManaois - SPIRITUALITY IN NURSING QUIZDan Dan Manaois100% (1)
- Bag TechniqueDocument3 pagesBag TechniqueKristina Marie Bugnosen100% (1)
- Leopolds Maneuver - Return DemoDocument1 pageLeopolds Maneuver - Return DemornrmmanphdPas encore d'évaluation
- Rectal and Vaginal Suppository Insertion GuideDocument2 pagesRectal and Vaginal Suppository Insertion GuideMariah Jane TaladuaPas encore d'évaluation
- Health, Wellness and IllnessDocument4 pagesHealth, Wellness and Illnessmbx47Pas encore d'évaluation
- Mouth and OropharynxDocument17 pagesMouth and OropharynxNursidar Pascual MukattilPas encore d'évaluation
- Nursing Care PlansDocument2 pagesNursing Care PlansatchiekPas encore d'évaluation
- Basic Interventions To Maintain Mobility and Exercise - Nov. 20Document9 pagesBasic Interventions To Maintain Mobility and Exercise - Nov. 20Tom CuencaPas encore d'évaluation
- Nursing Care of A Family With A Toddler Child: Christine M. Fiel, RN MN LPT MaedDocument25 pagesNursing Care of A Family With A Toddler Child: Christine M. Fiel, RN MN LPT MaedJrose CuerpoPas encore d'évaluation
- Assisting With Cast ApplicationDocument6 pagesAssisting With Cast ApplicationPrince TulauanPas encore d'évaluation
- Handwashing QuestionsDocument2 pagesHandwashing Questionsknicky FranciscoPas encore d'évaluation
- Gordons Functional Health Patterns GuideDocument4 pagesGordons Functional Health Patterns GuideteuuuuPas encore d'évaluation
- Assessing AbdomenDocument1 pageAssessing AbdomenKeesha Mae Urgelles TimogPas encore d'évaluation
- Drug Therapeutic Record TemplateDocument1 pageDrug Therapeutic Record TemplateAubrey Justine GaleonPas encore d'évaluation
- NCM 100 H.A Procedure DPPER 3Document51 pagesNCM 100 H.A Procedure DPPER 3Richelle Joy Durano RegatunaPas encore d'évaluation
- Assessing the Chest and AbdomenDocument19 pagesAssessing the Chest and AbdomenNicole BertulfoPas encore d'évaluation
- Self Breast ExaminationDocument2 pagesSelf Breast ExaminationMaye Marquino Lofranco NeriPas encore d'évaluation
- Head To Toe AssessmentDocument56 pagesHead To Toe AssessmentmisshiePas encore d'évaluation
- 10 Rights of Drug AdministrationDocument1 page10 Rights of Drug AdministrationDoyTanPas encore d'évaluation
- NALAM 106 Ass. AntibioticsDocument6 pagesNALAM 106 Ass. AntibioticsBeth100% (1)
- Cleansing Bed Bath: General ObjectivesDocument3 pagesCleansing Bed Bath: General ObjectivesPauline AñesPas encore d'évaluation
- Handwashing and Gloving (Checklist)Document2 pagesHandwashing and Gloving (Checklist)Christian Christopher Lopez100% (1)
- Compilation of Reviewer For Fundamentals of Nursing PDF FreeDocument49 pagesCompilation of Reviewer For Fundamentals of Nursing PDF FreeTyler VintPas encore d'évaluation
- Elec 121Document14 pagesElec 121MARITONI MEDALLAPas encore d'évaluation
- Apgar Scoring System ExplainedDocument3 pagesApgar Scoring System ExplainedAshley SorgenPas encore d'évaluation
- Case ScenarioDocument2 pagesCase ScenarioMARIA ANGELIKA DEL ROSARIOPas encore d'évaluation
- Flail Chest (Tayug)Document25 pagesFlail Chest (Tayug)Adrian MallarPas encore d'évaluation
- Guidelines in BedmakingDocument9 pagesGuidelines in Bedmakinglex aspira100% (1)
- Health Education Plan - Case StudyDocument7 pagesHealth Education Plan - Case StudyRenzy Mayven Pedriña LobatonPas encore d'évaluation
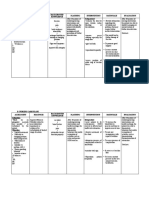
- Assessment Nursing Diagnosis Rationale Planning Implementation Rationale EvaluationDocument2 pagesAssessment Nursing Diagnosis Rationale Planning Implementation Rationale EvaluationHsintan HsuPas encore d'évaluation
- Assistive Devices - WalkerDocument51 pagesAssistive Devices - WalkerGrand Levi100% (1)
- History of Health Education and NursingDocument3 pagesHistory of Health Education and Nursing3amabelle arevaloPas encore d'évaluation
- Bag TechniqueDocument30 pagesBag Techniquecoosa liquors100% (1)
- Open GlovingDocument29 pagesOpen GlovingLexi Lore100% (1)
- Gordon's Health Pattern ChecklistDocument3 pagesGordon's Health Pattern ChecklistNavora, Bryle TrixthanePas encore d'évaluation
- NCP RiskDocument2 pagesNCP RiskNorries Jonell CaballarPas encore d'évaluation
- LAB Calculating Diets and Meal Planning Module 1Document15 pagesLAB Calculating Diets and Meal Planning Module 1Angelica PalacPas encore d'évaluation
- Assessing the Thorax and LungsDocument26 pagesAssessing the Thorax and LungsTarah LedesmaPas encore d'évaluation
- Demographic Profile, Bubbleshe, Discharge Planning Methods Edited... Wala Pa Yung NCP KODocument6 pagesDemographic Profile, Bubbleshe, Discharge Planning Methods Edited... Wala Pa Yung NCP KONicoh AvilaPas encore d'évaluation
- Sultan Kudarat State University College of Health SciencesDocument7 pagesSultan Kudarat State University College of Health SciencesRheal P EsmailPas encore d'évaluation
- Nursing Physical AssessmentDocument5 pagesNursing Physical AssessmentApril Louise PaluganPas encore d'évaluation
- The Qualities and Responsibilities of a Good Health Care ProviderDocument5 pagesThe Qualities and Responsibilities of a Good Health Care ProviderEvelyn Medina0% (1)
- St. Michael's College: Nursing Care Plan FormDocument3 pagesSt. Michael's College: Nursing Care Plan Formacademic purposesPas encore d'évaluation
- Nursing Care PlanDocument1 pageNursing Care PlanMikki lor PuaganPas encore d'évaluation
- Foley Catheter Insertion ProcedureDocument6 pagesFoley Catheter Insertion ProcedureJustine VillaflorPas encore d'évaluation
- ETHICAL AND LEGAL ASPECTS OF HEALTH EDUCATIONDocument4 pagesETHICAL AND LEGAL ASPECTS OF HEALTH EDUCATIONMaria Angelika BughaoPas encore d'évaluation
- Health AssessmentDocument31 pagesHealth AssessmentLoi Ocampo Crespo100% (1)
- Excellent Very Good Good Fair PoorDocument4 pagesExcellent Very Good Good Fair PoorJmarie Brillantes PopiocoPas encore d'évaluation
- NCP PneumoniaDocument2 pagesNCP Pneumoniajulz_otso6359Pas encore d'évaluation
- Basic Nutrition and Diet TherapyDocument48 pagesBasic Nutrition and Diet Therapytamy_001Pas encore d'évaluation
- Administering Oral MedicationsDocument5 pagesAdministering Oral MedicationsAda Gay Olandia SerencioPas encore d'évaluation
- NCM 120 Procedural Checklist NEURODocument60 pagesNCM 120 Procedural Checklist NEUROLorenz Jude CańetePas encore d'évaluation
- Health Assessment Checklist Week1 and 2Document7 pagesHealth Assessment Checklist Week1 and 2Wylyn Mae VisqueraPas encore d'évaluation
- Western Mindanao student evaluation formsDocument13 pagesWestern Mindanao student evaluation formsRay Daniel E. BilbaoPas encore d'évaluation
- Assessing The Appearance and Mental Status Skin, Hair and Nails Basic ConceptDocument9 pagesAssessing The Appearance and Mental Status Skin, Hair and Nails Basic ConceptArtemis B BellaPas encore d'évaluation
- HO#1.1 Caring For The BodyDocument7 pagesHO#1.1 Caring For The BodyGemma CanlapanPas encore d'évaluation
- Grade 4 WINS OrientationDocument2 pagesGrade 4 WINS OrientationChristine FranciscoPas encore d'évaluation
- Macronutrients ProteinsDocument2 pagesMacronutrients ProteinsEllice O. MonizPas encore d'évaluation
- Your Body Speaks Your Mind by Deb ShapiroDocument315 pagesYour Body Speaks Your Mind by Deb Shapiroisidora milosevic100% (2)
- Nursing Abbreviations, Acronyms and Symbols QuizDocument3 pagesNursing Abbreviations, Acronyms and Symbols QuizAjeng Citra S SeptiyantriPas encore d'évaluation
- Acy 087Document14 pagesAcy 087johnsmithdosPas encore d'évaluation
- Alvarez 2015Document18 pagesAlvarez 2015Clara RodriguesPas encore d'évaluation
- Report - AYESHA KHATOON (230750060006)Document3 pagesReport - AYESHA KHATOON (230750060006)ahmedkhandba1Pas encore d'évaluation
- 4th Quarter CAPSTONEDocument30 pages4th Quarter CAPSTONEWallace RamosPas encore d'évaluation
- Đề số 10Document4 pagesĐề số 10Duong Nguyen Trieu100% (1)
- KCC Mall 69kV Substation DesignDocument18 pagesKCC Mall 69kV Substation DesignRomie ArazaPas encore d'évaluation
- r147229149 Jenny Valdirio CUR147229149Document1 pager147229149 Jenny Valdirio CUR147229149Jenny Valdirio PozzoPas encore d'évaluation
- Quality Assurance in Medical LaboratoriesDocument69 pagesQuality Assurance in Medical Laboratories"DocAxi" Maximo B Axibal Jr MD FPSP100% (1)
- Annex 2 7d PEMAPS QuestionnaireDocument5 pagesAnnex 2 7d PEMAPS QuestionnaireAlma PustaPas encore d'évaluation
- Single/ Exam Zone Centre DetailsDocument5 pagesSingle/ Exam Zone Centre DetailsHarsh AroraPas encore d'évaluation
- Sport Science and Sports Medicine Framework 2017 v1Document31 pagesSport Science and Sports Medicine Framework 2017 v1api-443327549Pas encore d'évaluation
- Annual Report 2013-14Document198 pagesAnnual Report 2013-14shahabPas encore d'évaluation
- Cholera FinalDocument57 pagesCholera FinalBinayaPas encore d'évaluation
- Fundamentals of EU Regulatory Affairs, Fifth Edition Comparative MatrixDocument42 pagesFundamentals of EU Regulatory Affairs, Fifth Edition Comparative Matrixasifmdzakaria57% (7)
- Lean GuideDocument155 pagesLean GuideSujoy Kar100% (1)
- Warehouse Center Checklist 2Document5 pagesWarehouse Center Checklist 2Sankar ChinnathambiPas encore d'évaluation
- Obstetrics Case Proforma TemplateDocument4 pagesObstetrics Case Proforma TemplateSwapneelShah100% (1)
- USMLE High YieldDocument8 pagesUSMLE High YieldNajia ChoudhuryPas encore d'évaluation
- Ar-Afff 3 MSDS LCFDocument5 pagesAr-Afff 3 MSDS LCFMark YePas encore d'évaluation
- GRADE 5 - WEEK 6 Catch UpDocument8 pagesGRADE 5 - WEEK 6 Catch Upbutchabdon1992Pas encore d'évaluation
- Bio SaftyDocument7 pagesBio Saftyapi-283956320Pas encore d'évaluation
- 1 s2.0 S2772569323000026 MainDocument8 pages1 s2.0 S2772569323000026 MainAditya RizkyPas encore d'évaluation
- Hematology Lecture - AnemiaDocument10 pagesHematology Lecture - AnemiaKimberly EspaldonPas encore d'évaluation
- International Congress 1263Document12 pagesInternational Congress 1263AksMastPas encore d'évaluation
- Modern Language Aptitude Test Ethics in Assessing Foreign Language Learning DisabilityDocument11 pagesModern Language Aptitude Test Ethics in Assessing Foreign Language Learning DisabilitypirhotmunthePas encore d'évaluation