Vous aimerez peut-être aussi
- Nowak PancreasDocument53 pagesNowak PancreasSahirPas encore d'évaluation
- Lesson 7 Glucose HomeostasisDocument39 pagesLesson 7 Glucose Homeostasissaja MuhammadPas encore d'évaluation
- Jurnal KedokteranDocument29 pagesJurnal KedokteranRatna ChairunnisaPas encore d'évaluation
- Physio Correl - Insulin and GlucagonDocument33 pagesPhysio Correl - Insulin and GlucagonDan Tristam MicabaloPas encore d'évaluation
- Hormones in Metabolism (DR - Ani Retno)Document45 pagesHormones in Metabolism (DR - Ani Retno)AciPas encore d'évaluation
- Glucagon and Its Metabolic EffectsDocument31 pagesGlucagon and Its Metabolic EffectsnikenPas encore d'évaluation
- Glycolysis - 1 - WUSLDocument52 pagesGlycolysis - 1 - WUSLAruni piyuminiPas encore d'évaluation
- Pancreas Aug 4Document53 pagesPancreas Aug 4Dr.Gomathi sivakumarPas encore d'évaluation
- Metabolic Syndrome and Diabetes - 200918Document80 pagesMetabolic Syndrome and Diabetes - 200918helena.lovrincevicPas encore d'évaluation
- Introduction To The Endocrine Control On MetabolismDocument79 pagesIntroduction To The Endocrine Control On Metabolisminka.elsePas encore d'évaluation
- Kuliah Biokimia Blok 2.4.1Document44 pagesKuliah Biokimia Blok 2.4.1Prajna PPas encore d'évaluation
- Pancreas: Ahmad AminuddinDocument16 pagesPancreas: Ahmad AminuddinWhydia Wedha SutedjaPas encore d'évaluation
- Diabetic Emergencies in Small AnimalsDocument17 pagesDiabetic Emergencies in Small Animalsdia_diannePas encore d'évaluation
- Metabolism Interaction and Hormone Regulation.Document81 pagesMetabolism Interaction and Hormone Regulation.fikaduPas encore d'évaluation
- InsulinDocument50 pagesInsulinTandin SonamPas encore d'évaluation
- Physio 7Document12 pagesPhysio 7amjadPas encore d'évaluation
- Worksheet MteabDocument3 pagesWorksheet MteabMariel TagazaPas encore d'évaluation
- Lecture 14Document25 pagesLecture 14Rezwan Noor NSUPas encore d'évaluation
- Carbohydrate Storage and Synthesis in Liver and Muscle: GlycogenDocument40 pagesCarbohydrate Storage and Synthesis in Liver and Muscle: GlycogenJay R PlogioPas encore d'évaluation
- GI and Reproductive HormoneDocument74 pagesGI and Reproductive Hormonepranutan739Pas encore d'évaluation
- Lecture (9) Integration of MetabolismDocument40 pagesLecture (9) Integration of MetabolismMahmoud ElazbPas encore d'évaluation
- Anatomy of Pancreas and Glucose Homeostasis: DR - Sasikala. JDocument48 pagesAnatomy of Pancreas and Glucose Homeostasis: DR - Sasikala. JsaranpcPas encore d'évaluation
- Physiology of Diabetes: Dr. Solomon Sathishkumar. MDDocument36 pagesPhysiology of Diabetes: Dr. Solomon Sathishkumar. MDKhaled LajmiPas encore d'évaluation
- Carbohydrate Metabolism b-170810140942 PDFDocument119 pagesCarbohydrate Metabolism b-170810140942 PDFsimasPas encore d'évaluation
- Glycolysis Regulation: 1 Dr. Suheir EreqatDocument22 pagesGlycolysis Regulation: 1 Dr. Suheir EreqatIbrahim BarhamPas encore d'évaluation
- Blood Sugar: AtionDocument93 pagesBlood Sugar: Ationmidhunramesh007100% (2)
- 1 s2.0 S0092867417314435 MainDocument33 pages1 s2.0 S0092867417314435 MainJiearPas encore d'évaluation
- End PancreasDocument29 pagesEnd Pancreasahmed alkramyPas encore d'évaluation
- InMet I Well-Fed State Spring 23Document32 pagesInMet I Well-Fed State Spring 23Erin HillPas encore d'évaluation
- Carbohydrate Metabolism and BiosynthesisDocument44 pagesCarbohydrate Metabolism and BiosynthesisEmman RegondolaPas encore d'évaluation
- GluconeogenesisDocument48 pagesGluconeogenesisQshyanPas encore d'évaluation
- Regulation of Glycogen MetabolismDocument18 pagesRegulation of Glycogen MetabolismNoel ManyisePas encore d'évaluation
- PP BioquímicaDocument22 pagesPP BioquímicaPeter ParkerPas encore d'évaluation
- Gluconeogenesis and Cori CycleDocument21 pagesGluconeogenesis and Cori CycleAboubakar Moalim Mahad moh'dPas encore d'évaluation
- Carbohydrate Metab 2Document65 pagesCarbohydrate Metab 2Ma-anJaneDiamosPas encore d'évaluation
- Intergration of MetabolismDocument112 pagesIntergration of MetabolismSantino MajokPas encore d'évaluation
- Overview of The Major Metabolic PathwaysDocument6 pagesOverview of The Major Metabolic Pathwayssmilechance80% (1)
- Reg of BGDocument42 pagesReg of BGSuhayb CumarPas encore d'évaluation
- Metabolisme GlikogenDocument17 pagesMetabolisme GlikogenMUHAMMAD RIDOPas encore d'évaluation
- Diabetes Mellitus: Regulation of Blood GlucoseDocument65 pagesDiabetes Mellitus: Regulation of Blood GlucoseReggae BautistaPas encore d'évaluation
- Glucose HomeostasisDocument37 pagesGlucose HomeostasisBryan DocallasPas encore d'évaluation
- 췌장호르몬과 당뇨Document28 pages췌장호르몬과 당뇨missoni0408Pas encore d'évaluation
- Insulin PresentationDocument43 pagesInsulin Presentationinnocence faded100% (2)
- Hepatica ClearanceDocument6 pagesHepatica ClearanceStephania NiñoPas encore d'évaluation
- Human Biology (Biologi Manuasia) : Prof Madya Dr. Mohamad Aziz DollahDocument29 pagesHuman Biology (Biologi Manuasia) : Prof Madya Dr. Mohamad Aziz DollahQisNani NorainiPas encore d'évaluation
- CHO Lec 1Document9 pagesCHO Lec 1sajjadany50Pas encore d'évaluation
- Insulin, Glucagon FinalDocument27 pagesInsulin, Glucagon FinalDhruvil GadhiyaPas encore d'évaluation
- Metabolism of CarbohydratesDocument5 pagesMetabolism of Carbohydrateskathleenmaisiedevilla.021105Pas encore d'évaluation
- Insulin and The Oral HypoglycemicsDocument9 pagesInsulin and The Oral HypoglycemicsHasibPas encore d'évaluation
- Diabetes Spectr 2004 Aronoff 183 90Document8 pagesDiabetes Spectr 2004 Aronoff 183 90Bodea DoruPas encore d'évaluation
- Glycolysis For NursesDocument17 pagesGlycolysis For NursesAaron WallacePas encore d'évaluation
- Ch. 4.4 - Hormonal Regulation of Carbohydrate MetabolismDocument19 pagesCh. 4.4 - Hormonal Regulation of Carbohydrate MetabolismCardiac RebuttalPas encore d'évaluation
- Glucose Homeostasis: by Dr. Sumbul FatmaDocument28 pagesGlucose Homeostasis: by Dr. Sumbul Fatmaraanja2Pas encore d'évaluation
- Anatomy and PhysiologyDocument2 pagesAnatomy and PhysiologyJeffrey Calicdan BucalaPas encore d'évaluation
- 14 - Blood Glucose HomeostasisDocument34 pages14 - Blood Glucose HomeostasischeckmatePas encore d'évaluation
- LIPOGENESISDocument6 pagesLIPOGENESISMUTHONI IRERIPas encore d'évaluation
- Recitation - Metabolic Fate of Glucose and Fatty AcidsDocument2 pagesRecitation - Metabolic Fate of Glucose and Fatty AcidshoytherePas encore d'évaluation
- 4-CHO Metabolism 2 & DMDocument33 pages4-CHO Metabolism 2 & DMlobna adelPas encore d'évaluation
- Dr. Solomon Sathishkumar, MD Department of Physiology Christian Medical College Vellore, IndiaDocument48 pagesDr. Solomon Sathishkumar, MD Department of Physiology Christian Medical College Vellore, IndiaKrairat KomdeePas encore d'évaluation
- UntitledDocument56 pagesUntitledkelvin kyandoPas encore d'évaluation
- Quarter: 1 Lesson 1 Content Standard:: What I Need To KnowDocument13 pagesQuarter: 1 Lesson 1 Content Standard:: What I Need To KnowRichard Balicat Jr.Pas encore d'évaluation
- Tiếng Anh Chuyên Ngành - Trắc Nghiệm 2Document3 pagesTiếng Anh Chuyên Ngành - Trắc Nghiệm 2Nguyễn Thiện LuânPas encore d'évaluation
- Basic Mechanical Ventilation PDFDocument8 pagesBasic Mechanical Ventilation PDFPabloIgLopezPas encore d'évaluation
- Vital Signs Procedures ChecklistDocument3 pagesVital Signs Procedures Checklistjuancristo91% (22)
- Acute Respiratory Failure Pa Tho PhysiologyDocument4 pagesAcute Respiratory Failure Pa Tho Physiologyroseanne18100% (4)
- EPILEPSYDocument5 pagesEPILEPSYIffa NooramPas encore d'évaluation
- NCM116 Module 3 Cerebrovascular Disease QuizDocument5 pagesNCM116 Module 3 Cerebrovascular Disease QuizIvan FernandezPas encore d'évaluation
- English Sistem EndocrineDocument9 pagesEnglish Sistem EndocrineNurlaili YaniPas encore d'évaluation
- Chap 12 Energy and RespirationDocument34 pagesChap 12 Energy and RespirationGeorge ApidiPas encore d'évaluation
- Muscles NotesDocument13 pagesMuscles NotesGabrielle ThompsonPas encore d'évaluation
- Muscle PhysiologyDocument64 pagesMuscle Physiologylynn.dargham2Pas encore d'évaluation
- Krok 1 Stomatology 2010Document22 pagesKrok 1 Stomatology 2010helloPas encore d'évaluation
- M.SC Questions PaperDocument2 pagesM.SC Questions Paperkhela Ram SorenPas encore d'évaluation
- Physiology of The Liver: Corresponding AuthorDocument12 pagesPhysiology of The Liver: Corresponding AuthorMansour HazaPas encore d'évaluation
- Multiple Choice Questions-Acid Base BalanceDocument6 pagesMultiple Choice Questions-Acid Base Balanceyeshi janexoPas encore d'évaluation
- The European Guideline On Management of Major Bleeding and Coagulopathy Following Trauma Sixth Edition (2023) PDFDocument1 pageThe European Guideline On Management of Major Bleeding and Coagulopathy Following Trauma Sixth Edition (2023) PDFMatheus LiraPas encore d'évaluation
- Plant Tissues: Class: 7 Board: ICSE Year: 2021-2022Document31 pagesPlant Tissues: Class: 7 Board: ICSE Year: 2021-2022shalu malaniPas encore d'évaluation
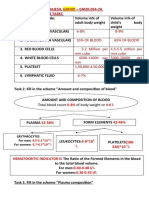
- Name - Soni Ritika Rajesh, Group - GM20-054-2A Physiology Week 03 TasksDocument10 pagesName - Soni Ritika Rajesh, Group - GM20-054-2A Physiology Week 03 TasksRitika SoniPas encore d'évaluation
- Science Vi-Quarter 2 Module (Week 1-2 Circulatory System)Document12 pagesScience Vi-Quarter 2 Module (Week 1-2 Circulatory System)Denver TamayoPas encore d'évaluation
- Business Brochure Template DesignDocument2 pagesBusiness Brochure Template DesignRuuRii NoPas encore d'évaluation
- Concepts of Human Physiology in Ayurveda: January 2008Document14 pagesConcepts of Human Physiology in Ayurveda: January 2008raj28_999Pas encore d'évaluation
- The Human Endocrine System's Glands WorksheetDocument4 pagesThe Human Endocrine System's Glands WorksheetAngelyn Mirones100% (2)
- Human Body Organ Systems - WorksheetDocument7 pagesHuman Body Organ Systems - WorksheetMirellaPas encore d'évaluation
- Blood Supply of The HeartDocument5 pagesBlood Supply of The HeartMohammed EljackPas encore d'évaluation
- Functions of CarbohydrateDocument11 pagesFunctions of CarbohydrateAbdulbaasit AyoolaPas encore d'évaluation
- Perilite Exposure and Hot Sitz BathDocument23 pagesPerilite Exposure and Hot Sitz BathJohn Dave V. VillarmentePas encore d'évaluation
- RespirationDocument33 pagesRespirationjtPas encore d'évaluation
- NCP (Baluyot Jason Lee) Group17Document3 pagesNCP (Baluyot Jason Lee) Group17Jasonlee BaluyotPas encore d'évaluation
- 697-Article Text-1372-1-10-20191104Document6 pages697-Article Text-1372-1-10-20191104NuyPas encore d'évaluation