Vous aimerez peut-être aussi
- Polycystic Kidney DiseaseDocument9 pagesPolycystic Kidney DiseaseCésar Aguilar ContrerasPas encore d'évaluation
- Atherosclerosis PresentationDocument90 pagesAtherosclerosis PresentationAbu SaifPas encore d'évaluation
- AtherosclerosisDocument54 pagesAtherosclerosislohit_chauhanPas encore d'évaluation
- Infectious DiseasesDocument144 pagesInfectious DiseasesMd.Mahmudul HasanPas encore d'évaluation
- Alzheimer Disease: Petra Nowotny, Jennifer M Kwon, Alison M GoateDocument6 pagesAlzheimer Disease: Petra Nowotny, Jennifer M Kwon, Alison M GoatedineshhissarPas encore d'évaluation
- Absolute Dermatology Review - Mastering Clinical Conditions On The Dermatology Recertification Exam (PDFDrive)Document461 pagesAbsolute Dermatology Review - Mastering Clinical Conditions On The Dermatology Recertification Exam (PDFDrive)mogoscristina100% (1)
- Complete VaccinationDocument2 pagesComplete VaccinationNgoo NwosuPas encore d'évaluation
- Hirschsprun G'S Disease: Dr. Manish Kumar Gupta Assistant Professor Department of Paediatric Surgery AIIMS, RishikeshDocument48 pagesHirschsprun G'S Disease: Dr. Manish Kumar Gupta Assistant Professor Department of Paediatric Surgery AIIMS, RishikeshArchana Mahata100% (1)
- Neoplastic Diseases of The OvaryDocument61 pagesNeoplastic Diseases of The Ovaryea013Pas encore d'évaluation
- Rabdomyosarcoma Case ReportDocument7 pagesRabdomyosarcoma Case ReportAaslesha Jakkampudi100% (1)
- Chest Tube Drainage of The Pleural SpaceDocument10 pagesChest Tube Drainage of The Pleural SpaceFernandaPas encore d'évaluation
- Hypo Album inDocument11 pagesHypo Album inAndi Agung RiatmojoPas encore d'évaluation
- Oral CandidiasisDocument5 pagesOral CandidiasisJPas encore d'évaluation
- Candidiasis - Causes, Symptoms, Treatment, DiagnosisDocument5 pagesCandidiasis - Causes, Symptoms, Treatment, DiagnosisChaiwa JustinePas encore d'évaluation
- Henoch Schonlein Purpura REVDocument42 pagesHenoch Schonlein Purpura REVBayu Kurniawan100% (1)
- Candidiasis Medical MycologyDocument58 pagesCandidiasis Medical MycologyNoor MemonPas encore d'évaluation
- Cell Structure of Cryptococcus FungiDocument19 pagesCell Structure of Cryptococcus FungiArshjyoti SinghPas encore d'évaluation
- Enterovirus & PoliomyelitisDocument17 pagesEnterovirus & PoliomyelitisAbdulsalam HashiPas encore d'évaluation
- Market Survey On Candida Drugs and ProbioticsDocument27 pagesMarket Survey On Candida Drugs and ProbioticsStephen MoorePas encore d'évaluation
- Biomedical Waste Management DownloadDocument22 pagesBiomedical Waste Management Downloaddr_kumananPas encore d'évaluation
- Myco/CandidaDocument29 pagesMyco/Candidaesraa100% (1)
- Agents of Respiratory DiseaseDocument25 pagesAgents of Respiratory DiseaseAbid AliPas encore d'évaluation
- Candidiasis 1Document5 pagesCandidiasis 1jodericoPas encore d'évaluation
- Necrotizing Pneumonia and Lung AbscessDocument11 pagesNecrotizing Pneumonia and Lung AbscessIman KhanPas encore d'évaluation
- Oral Candidiasis - ReviewDocument9 pagesOral Candidiasis - ReviewAdhelia Galuh PrmtsrPas encore d'évaluation
- Peptic UlcerDocument31 pagesPeptic UlcerHarpal Bajwa0% (1)
- Approach To A Patient With Jaundice: Group A9 Cho, Chua Family, Co Family, CofrerosDocument115 pagesApproach To A Patient With Jaundice: Group A9 Cho, Chua Family, Co Family, CofrerosEunice Co100% (1)
- Mucocutaneus Candidiasis: Dosen Pembimbing: DR - Dr.anni Andriani, SP - KK Pembimbing Residen: Dr. EvelynDocument37 pagesMucocutaneus Candidiasis: Dosen Pembimbing: DR - Dr.anni Andriani, SP - KK Pembimbing Residen: Dr. EvelynHamizah Hasbullah100% (1)
- Candidosis A New ChallengeDocument7 pagesCandidosis A New ChallengeSalvador contreras huertaPas encore d'évaluation
- Candidiasis A Fungal Infection Current Challenges and ProgressDocument11 pagesCandidiasis A Fungal Infection Current Challenges and ProgressLau's WorldPas encore d'évaluation
- Pancreatic AdenocarcinomaDocument6 pagesPancreatic AdenocarcinomafikriafisPas encore d'évaluation
- Hemorrhagic Conditions in Neonates: DR Hodan Ahmed, Department of Pediatrics and Child Health, Amoud Medical School, AUDocument27 pagesHemorrhagic Conditions in Neonates: DR Hodan Ahmed, Department of Pediatrics and Child Health, Amoud Medical School, AUAbdisalan hassanPas encore d'évaluation
- Clinical Management: PGI Eileen Andres PediatricsDocument9 pagesClinical Management: PGI Eileen Andres PediatricsMichael BonillaPas encore d'évaluation
- RCJ Finals - Non Epithelial Ovarian CaDocument4 pagesRCJ Finals - Non Epithelial Ovarian CaJohn Paulo Catacutan100% (1)
- AthetosisDocument2 pagesAthetosisapi-19973386Pas encore d'évaluation
- GROSS - Broncho & Lobar PneumoniaDocument2 pagesGROSS - Broncho & Lobar PneumoniaAra Diocos100% (1)
- Causes of Peptic Ulcers:: Helicobacter Pylori (H. Pylori)Document4 pagesCauses of Peptic Ulcers:: Helicobacter Pylori (H. Pylori)jessie monroePas encore d'évaluation
- Lobar Pneumonia: Deevon M. Cariaga FEU-NRMF Institute of MedicineDocument12 pagesLobar Pneumonia: Deevon M. Cariaga FEU-NRMF Institute of MedicinedeevoncPas encore d'évaluation
- Degeneration and Regenration of Nerve Fibers by Dr. RoomiDocument11 pagesDegeneration and Regenration of Nerve Fibers by Dr. RoomiMudassar RoomiPas encore d'évaluation
- Hereditary Spherocytosis, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsD'EverandHereditary Spherocytosis, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsPas encore d'évaluation
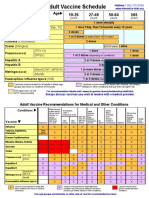
- Adult Vaccine Schedule Eng PDFDocument2 pagesAdult Vaccine Schedule Eng PDFAbdur RehmanPas encore d'évaluation
- Neuro General Neuro: Proptosis/ Exophthalmos ChemosisDocument4 pagesNeuro General Neuro: Proptosis/ Exophthalmos ChemosisShakina FareedPas encore d'évaluation
- HIV Natural HistoryDocument10 pagesHIV Natural HistoryNirav Sharma100% (1)
- Peptic Ulcer DiseaseDocument14 pagesPeptic Ulcer DiseasePernel Jose Alam MicuboPas encore d'évaluation
- Herpes Simplex KeratitisDocument2 pagesHerpes Simplex KeratitisSugam GouliPas encore d'évaluation
- Pathology of Digestive SystemDocument28 pagesPathology of Digestive SystemDianNursyifaRahmahPas encore d'évaluation
- Abdominal TraumaDocument24 pagesAbdominal TraumaSurgeryClassesPas encore d'évaluation
- Fenton Growth Chart CalculationsDocument6 pagesFenton Growth Chart CalculationsNahari ArifinPas encore d'évaluation
- Case Presentation: Prepared By: Erick Rafel Anca, M.DDocument121 pagesCase Presentation: Prepared By: Erick Rafel Anca, M.DErick AncaPas encore d'évaluation
- Blood and Tissue ProtozoaDocument32 pagesBlood and Tissue ProtozoaFort SalvadorPas encore d'évaluation
- Treatment of Infections Associated With Surgical ImplantsDocument8 pagesTreatment of Infections Associated With Surgical ImplantsDiego Bedón AscurraPas encore d'évaluation
- Henoch Scholein PurpuraDocument15 pagesHenoch Scholein PurpurapkpowerhousePas encore d'évaluation
- Gyne - Case 11 Lower Genital UTI PDFDocument2 pagesGyne - Case 11 Lower Genital UTI PDFcbac1990Pas encore d'évaluation
- CryptococcosisDocument25 pagesCryptococcosisinvisibleyetinvinciblePas encore d'évaluation
- Syncope AFPDocument12 pagesSyncope AFP李英誠Pas encore d'évaluation
- Retinoblastoma - EyeWikiDocument11 pagesRetinoblastoma - EyeWikimay171989Pas encore d'évaluation
- CSF AnalysisDocument6 pagesCSF Analysisfrederico_Pas encore d'évaluation
- Reference 1. Satyanarayanajois, S., Stephanie, V., Liu, J., Go, M.L., 2009, Design, Synthesis, and Docking Studies ofDocument1 pageReference 1. Satyanarayanajois, S., Stephanie, V., Liu, J., Go, M.L., 2009, Design, Synthesis, and Docking Studies ofScholastika Palayukan100% (1)
- Neurological Examination of The NewbornDocument21 pagesNeurological Examination of The Newborncristieristiie100% (1)
- Tumours of The Central Nervous System: FM Brett MD., FrcpathDocument57 pagesTumours of The Central Nervous System: FM Brett MD., FrcpathDrGasnasPas encore d'évaluation
- Evaluation of Liver FunctionDocument64 pagesEvaluation of Liver FunctionMustafa KhandgawiPas encore d'évaluation
- Foreign Body AspirationDocument3 pagesForeign Body AspirationAsiya ZaidiPas encore d'évaluation
- Burkitt Lymphoma: Teacher: Daniel Hernández. Student: Diana Rosales DominguezDocument16 pagesBurkitt Lymphoma: Teacher: Daniel Hernández. Student: Diana Rosales DominguezDianita Rosales Dominguez100% (1)
- Abdominal InjuryDocument92 pagesAbdominal InjurympalanethraPas encore d'évaluation
- London School of Hygiene & Tropical Medicine: The Role of Diagnostics in The Antimicrobial Resistance ResponseDocument2 pagesLondon School of Hygiene & Tropical Medicine: The Role of Diagnostics in The Antimicrobial Resistance ResponseIsti RismaPas encore d'évaluation
- Yanzen Bagus Setiawan: Name: Date of Birth: Sex: NationalityDocument1 pageYanzen Bagus Setiawan: Name: Date of Birth: Sex: NationalitylisaPas encore d'évaluation
- Govt. of Himachal Pradesh: DEEPAK (Covid Pass No.: HP-2526572)Document2 pagesGovt. of Himachal Pradesh: DEEPAK (Covid Pass No.: HP-2526572)Vicky LakhanpalPas encore d'évaluation
- Viral Meningitis in Children Clinical Features and DiagnosisDocument25 pagesViral Meningitis in Children Clinical Features and DiagnosisTrúc QuỳnhPas encore d'évaluation
- Cme On TuberclosisDocument12 pagesCme On TuberclosisOdulusi DanielPas encore d'évaluation
- 2010 - 3 Idsp Detail Information BKDocument73 pages2010 - 3 Idsp Detail Information BKPankaj ModhPas encore d'évaluation
- Gastroenteritis: Escherichia ColiDocument4 pagesGastroenteritis: Escherichia ColiFanny BudimanPas encore d'évaluation
- Image Diagnosis: Hemorrhagic Bullae in A Primary Varicella Zoster Virus InfectionDocument2 pagesImage Diagnosis: Hemorrhagic Bullae in A Primary Varicella Zoster Virus InfectionHaniPas encore d'évaluation
- Laboratory Test Report: Sars-Cov-2Document1 pageLaboratory Test Report: Sars-Cov-2sandeep yadavPas encore d'évaluation
- Orange Berry RustDocument2 pagesOrange Berry RustsararmentaPas encore d'évaluation
- 1 InfluenzaDocument7 pages1 InfluenzaElena MoldoveanuPas encore d'évaluation
- WHO - WHO To Publish First Official Guidelines On Leprosy Diagnosis, Treatment and PreventionDocument5 pagesWHO - WHO To Publish First Official Guidelines On Leprosy Diagnosis, Treatment and PreventionSari RiastiningsihPas encore d'évaluation
- Department of Education: Accomplishment Report On Project WinsDocument6 pagesDepartment of Education: Accomplishment Report On Project WinsJuna Corazon PoblacioPas encore d'évaluation
- Isolation and Identification of Brucella SpeciesDocument20 pagesIsolation and Identification of Brucella SpeciesAquiles Baeza VergoñaPas encore d'évaluation
- ProtozoaDocument56 pagesProtozoaSalim JufriPas encore d'évaluation
- Wa0094.Document9 pagesWa0094.lider vigilanciaPas encore d'évaluation
- Kami Export - Pathogens-Stations-ReviewDocument3 pagesKami Export - Pathogens-Stations-ReviewAshley Cervantes VillanuevaPas encore d'évaluation
- Resource Unit 31finalDocument10 pagesResource Unit 31finalHector B. Jr PalacioPas encore d'évaluation
- Genital Tract InfectionsDocument4 pagesGenital Tract Infectionsmed.progressPas encore d'évaluation
- Chapter 20Document81 pagesChapter 20songezo mbutyePas encore d'évaluation
- AntibioticsDocument21 pagesAntibioticsJerry ArockePas encore d'évaluation
- Ciclos 6to Seminario Parasitos de Sangre y Tejidos II. Kine Top Last IdaDocument2 pagesCiclos 6to Seminario Parasitos de Sangre y Tejidos II. Kine Top Last Idaapi-3697245Pas encore d'évaluation
- OnikomikosisDocument19 pagesOnikomikosisMerlyn Chrislia RumthePas encore d'évaluation
- Record Redacte1Document1 pageRecord Redacte1Matt BrownPas encore d'évaluation
- Art and CultureDocument6 pagesArt and CultureParth TiwariPas encore d'évaluation
- Pneumonia and VAP PreventionDocument35 pagesPneumonia and VAP Preventionhendro harahapPas encore d'évaluation