Vous aimerez peut-être aussi
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeD'EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeÉvaluation : 4 sur 5 étoiles4/5 (5794)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreD'EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreÉvaluation : 4 sur 5 étoiles4/5 (1090)
- Never Split the Difference: Negotiating As If Your Life Depended On ItD'EverandNever Split the Difference: Negotiating As If Your Life Depended On ItÉvaluation : 4.5 sur 5 étoiles4.5/5 (838)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceD'EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceÉvaluation : 4 sur 5 étoiles4/5 (895)
- Grit: The Power of Passion and PerseveranceD'EverandGrit: The Power of Passion and PerseveranceÉvaluation : 4 sur 5 étoiles4/5 (588)
- Shoe Dog: A Memoir by the Creator of NikeD'EverandShoe Dog: A Memoir by the Creator of NikeÉvaluation : 4.5 sur 5 étoiles4.5/5 (537)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersD'EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersÉvaluation : 4.5 sur 5 étoiles4.5/5 (345)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureD'EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureÉvaluation : 4.5 sur 5 étoiles4.5/5 (474)
- Her Body and Other Parties: StoriesD'EverandHer Body and Other Parties: StoriesÉvaluation : 4 sur 5 étoiles4/5 (821)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)D'EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Évaluation : 4.5 sur 5 étoiles4.5/5 (121)
- The Emperor of All Maladies: A Biography of CancerD'EverandThe Emperor of All Maladies: A Biography of CancerÉvaluation : 4.5 sur 5 étoiles4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingD'EverandThe Little Book of Hygge: Danish Secrets to Happy LivingÉvaluation : 3.5 sur 5 étoiles3.5/5 (400)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyD'EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyÉvaluation : 3.5 sur 5 étoiles3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)D'EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Évaluation : 4 sur 5 étoiles4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaD'EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaÉvaluation : 4.5 sur 5 étoiles4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryD'EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryÉvaluation : 3.5 sur 5 étoiles3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnD'EverandTeam of Rivals: The Political Genius of Abraham LincolnÉvaluation : 4.5 sur 5 étoiles4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealD'EverandOn Fire: The (Burning) Case for a Green New DealÉvaluation : 4 sur 5 étoiles4/5 (74)
- The Unwinding: An Inner History of the New AmericaD'EverandThe Unwinding: An Inner History of the New AmericaÉvaluation : 4 sur 5 étoiles4/5 (45)
- English For Academic and Professional Purposes (EAPP) : Quarter 1 - Module 3: SummarizingDocument31 pagesEnglish For Academic and Professional Purposes (EAPP) : Quarter 1 - Module 3: SummarizingJay L. Espino85% (85)
- Domiciliary Midwifery RDocument16 pagesDomiciliary Midwifery Rswillymadhu83% (6)
- Inferior Vena Cava and Its TributariesDocument12 pagesInferior Vena Cava and Its TributariesRahaf MajadlyPas encore d'évaluation
- Chronic Renal Failure in North Central Province of Sri Lanka: An Environmentally Induced DiseaseDocument5 pagesChronic Renal Failure in North Central Province of Sri Lanka: An Environmentally Induced Diseasesumanenthiran123Pas encore d'évaluation
- Background: CKD of Uncertain Etiology Sri Lanka A Population Study at Girandurukotte, Uva Province, Preliminary ReportDocument6 pagesBackground: CKD of Uncertain Etiology Sri Lanka A Population Study at Girandurukotte, Uva Province, Preliminary Reportsumanenthiran123Pas encore d'évaluation
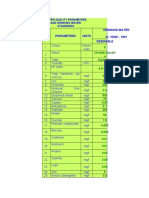
- Water Quality Parameters and Drinking Water StandardsDocument2 pagesWater Quality Parameters and Drinking Water Standardssumanenthiran123Pas encore d'évaluation
- Bala Upasana of Konganava SiddharDocument6 pagesBala Upasana of Konganava Siddharsumanenthiran123Pas encore d'évaluation
- Environmental Pollution in Sri Lanka A ReviewDocument25 pagesEnvironmental Pollution in Sri Lanka A Reviewsumanenthiran123Pas encore d'évaluation
- Siddha Vidya VignanDocument5 pagesSiddha Vidya Vignansumanenthiran123Pas encore d'évaluation
- Information SystemsDocument9 pagesInformation Systemssumanenthiran123Pas encore d'évaluation
- Siththa Vaidhya SikichakramamDocument133 pagesSiththa Vaidhya Sikichakramamsumanenthiran123100% (1)
- Data On Spice PriceDocument3 pagesData On Spice Pricesumanenthiran123Pas encore d'évaluation
- Background Ecotourism Defined AsDocument1 pageBackground Ecotourism Defined Assumanenthiran123Pas encore d'évaluation
- Spritual AlchamyDocument4 pagesSpritual Alchamysumanenthiran123Pas encore d'évaluation
- DiagnosisDocument9 pagesDiagnosissumanenthiran123Pas encore d'évaluation
- Sign, Star and Sub Table - KP AstrologyDocument12 pagesSign, Star and Sub Table - KP Astrologysumanenthiran123100% (2)
- UpasanaDocument10 pagesUpasanasumanenthiran123Pas encore d'évaluation
- Gayathri Siddha SadanaiDocument4 pagesGayathri Siddha Sadanaisumanenthiran123Pas encore d'évaluation
- Medicine BuddhaDocument3 pagesMedicine Buddhasumanenthiran123Pas encore d'évaluation
- Charaka Samhita, Sutrasthanam, Slokas The Section of Introductory, Theoretical and Philosophical Foundation of AyurvedaDocument240 pagesCharaka Samhita, Sutrasthanam, Slokas The Section of Introductory, Theoretical and Philosophical Foundation of AyurvedaAyurvista89% (9)
- Chapter 2 - Fundamental Principles - KP AstrologyDocument12 pagesChapter 2 - Fundamental Principles - KP Astrologysumanenthiran123100% (2)
- Home Composting SystemsDocument8 pagesHome Composting Systemssumanenthiran123Pas encore d'évaluation
- Principles of Fluid Therapy On The Basis ofDocument29 pagesPrinciples of Fluid Therapy On The Basis ofhendrytzPas encore d'évaluation
- Scientific Book Jicccim 2018Document171 pagesScientific Book Jicccim 2018ngwinda90Pas encore d'évaluation
- Impact of COVID-19 On Marketing AmityDocument59 pagesImpact of COVID-19 On Marketing AmitySudha RaniPas encore d'évaluation
- Cells - 1 V2 (Euks, Proks & Viruses)Document9 pagesCells - 1 V2 (Euks, Proks & Viruses)mormerodPas encore d'évaluation
- Feeding A Dairy CowDocument31 pagesFeeding A Dairy CowFrancis Onyango OduorPas encore d'évaluation
- Lucid Dreaming Tips OWDocument9 pagesLucid Dreaming Tips OWarlikPas encore d'évaluation
- Burn NotesDocument4 pagesBurn NotesRiza Angela BarazanPas encore d'évaluation
- About Monkey PoxDocument3 pagesAbout Monkey PoxObakoma Josiah100% (1)
- Nud 241 NoteDocument31 pagesNud 241 Notepdsth7mtsjPas encore d'évaluation
- DarwinDocument118 pagesDarwinmrthumb100% (2)
- For Review OAPDocument144 pagesFor Review OAPKim John Rull NatePas encore d'évaluation
- Hydrogen Sulfide FactDocument2 pagesHydrogen Sulfide FactAgriSafePas encore d'évaluation
- Science Technology and Society Assignment 1Document2 pagesScience Technology and Society Assignment 1VonPas encore d'évaluation
- Key Points: Information About Your Procedure From The British Association of Urological Surgeons (BAUS)Document6 pagesKey Points: Information About Your Procedure From The British Association of Urological Surgeons (BAUS)diva aurelliaPas encore d'évaluation
- CM2-CU10-Modification of Mendelian RatiosDocument17 pagesCM2-CU10-Modification of Mendelian RatiosClaire GonoPas encore d'évaluation
- BangkasDocument5 pagesBangkasJulianne BangkasPas encore d'évaluation
- Case Note 6: Patient DetailsDocument3 pagesCase Note 6: Patient DetailsBINCYPas encore d'évaluation
- A Comprehensive Overview On Osteoporosis and Its Risk FactorsDocument21 pagesA Comprehensive Overview On Osteoporosis and Its Risk Factorsdenta aePas encore d'évaluation
- DR Antonious CV N & AEDocument27 pagesDR Antonious CV N & AEdoctorantoniPas encore d'évaluation
- CASE STUDY PPT Group1 - Revised WithoutvideoDocument34 pagesCASE STUDY PPT Group1 - Revised WithoutvideoSamantha BolantePas encore d'évaluation
- OCTA InflammatoryEyediseaseSrivastavaDocument24 pagesOCTA InflammatoryEyediseaseSrivastavaPriyanka DocPas encore d'évaluation
- 11 Biology Notes ch02 Biological ClassificationDocument8 pages11 Biology Notes ch02 Biological ClassificationDivyaa SreekumarPas encore d'évaluation
- Positive and Negative Filipino ValuesDocument2 pagesPositive and Negative Filipino ValuesBrenty TablatePas encore d'évaluation
- Surgical Drains and TubesDocument3 pagesSurgical Drains and TubesYusra ShaukatPas encore d'évaluation
- Endometriosis: Endometriosis: Symptoms, Treatment, DiagnosisDocument4 pagesEndometriosis: Endometriosis: Symptoms, Treatment, DiagnosisrizkiaautikasariPas encore d'évaluation
- Allergic RhinitisDocument8 pagesAllergic RhinitisJuanPas encore d'évaluation
- Jewish Genetic DiseasesDocument2 pagesJewish Genetic DiseasesReformJudaismPas encore d'évaluation