Vous aimerez peut-être aussi
- The Yellow House: A Memoir (2019 National Book Award Winner)D'EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Évaluation : 4 sur 5 étoiles4/5 (98)
- A Toolkit For Intensive Care UnitsDocument28 pagesA Toolkit For Intensive Care UnitsekramsPas encore d'évaluation
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeD'EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeÉvaluation : 4 sur 5 étoiles4/5 (5795)
- Feeding Tubes Advanced DementiaDocument7 pagesFeeding Tubes Advanced DementiaekramsPas encore d'évaluation
- Shoe Dog: A Memoir by the Creator of NikeD'EverandShoe Dog: A Memoir by the Creator of NikeÉvaluation : 4.5 sur 5 étoiles4.5/5 (537)
- Case-Study-61-Report Urinary Incontinance PDFDocument16 pagesCase-Study-61-Report Urinary Incontinance PDFFayzaRayesPas encore d'évaluation
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureD'EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureÉvaluation : 4.5 sur 5 étoiles4.5/5 (474)
- Bell - S Palsy Aetiology, Classification, Differential Diagnosis and Treatment Consideration A ReviewDocument8 pagesBell - S Palsy Aetiology, Classification, Differential Diagnosis and Treatment Consideration A ReviewekramsPas encore d'évaluation
- Grit: The Power of Passion and PerseveranceD'EverandGrit: The Power of Passion and PerseveranceÉvaluation : 4 sur 5 étoiles4/5 (588)
- Helicobacter Pylori - The Latest in Diagnosis and TreatmentDocument5 pagesHelicobacter Pylori - The Latest in Diagnosis and TreatmentekramsPas encore d'évaluation
- On Fire: The (Burning) Case for a Green New DealD'EverandOn Fire: The (Burning) Case for a Green New DealÉvaluation : 4 sur 5 étoiles4/5 (74)
- Table1 ICU DailyGoalsSheetDocument3 pagesTable1 ICU DailyGoalsSheetekrams100% (1)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryD'EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryÉvaluation : 3.5 sur 5 étoiles3.5/5 (231)
- Why Are My Legs SwollenDocument5 pagesWhy Are My Legs SwollenekramsPas encore d'évaluation
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceD'EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceÉvaluation : 4 sur 5 étoiles4/5 (895)
- Caring For The Patient On A VentilatorDocument10 pagesCaring For The Patient On A Ventilatorekrams100% (1)
- Never Split the Difference: Negotiating As If Your Life Depended On ItD'EverandNever Split the Difference: Negotiating As If Your Life Depended On ItÉvaluation : 4.5 sur 5 étoiles4.5/5 (838)
- West Midlands Regional Training Package For Safe Blood Transfusion PracticeDocument20 pagesWest Midlands Regional Training Package For Safe Blood Transfusion PracticeekramsPas encore d'évaluation
- The Little Book of Hygge: Danish Secrets to Happy LivingD'EverandThe Little Book of Hygge: Danish Secrets to Happy LivingÉvaluation : 3.5 sur 5 étoiles3.5/5 (400)
- Calculating Parenteral FeedingsDocument5 pagesCalculating Parenteral FeedingsekramsPas encore d'évaluation
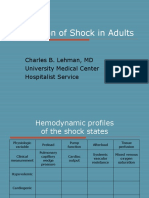
- Evaluation of Shock in AdultsDocument99 pagesEvaluation of Shock in AdultsekramsPas encore d'évaluation
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersD'EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersÉvaluation : 4.5 sur 5 étoiles4.5/5 (345)
- Kaposi's SarcomaDocument6 pagesKaposi's SarcomaveremkovichPas encore d'évaluation
- M5-Y12-OSCE Phase 1 Examiners FeedbackDocument9 pagesM5-Y12-OSCE Phase 1 Examiners FeedbackTanyaNganPas encore d'évaluation
- The Unwinding: An Inner History of the New AmericaD'EverandThe Unwinding: An Inner History of the New AmericaÉvaluation : 4 sur 5 étoiles4/5 (45)
- 6.Intra-Arch DistractionDocument15 pages6.Intra-Arch DistractionMónica C. BadilloPas encore d'évaluation
- Team of Rivals: The Political Genius of Abraham LincolnD'EverandTeam of Rivals: The Political Genius of Abraham LincolnÉvaluation : 4.5 sur 5 étoiles4.5/5 (234)
- Valleylab ForceTriad - User Manual PDFDocument100 pagesValleylab ForceTriad - User Manual PDFPaulina LekszyckaPas encore d'évaluation
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyD'EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyÉvaluation : 3.5 sur 5 étoiles3.5/5 (2259)
- Drug Infusion SystemsDocument13 pagesDrug Infusion Systemsオマル カジサジャPas encore d'évaluation
- United Biotech WorldDocument9 pagesUnited Biotech Worldswtyneha33Pas encore d'évaluation
- A Practical Treatise On Nervous Exhaustion (Neurasthenia) - G.M.BeardDocument232 pagesA Practical Treatise On Nervous Exhaustion (Neurasthenia) - G.M.BeardcableblancoPas encore d'évaluation
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaD'EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaÉvaluation : 4.5 sur 5 étoiles4.5/5 (266)
- Rectal Cancer Talk 1228785749826555 9Document54 pagesRectal Cancer Talk 1228785749826555 9Jantima SirisophonwattanaPas encore d'évaluation
- The Emperor of All Maladies: A Biography of CancerD'EverandThe Emperor of All Maladies: A Biography of CancerÉvaluation : 4.5 sur 5 étoiles4.5/5 (271)
- Launching The Century of PatientsDocument26 pagesLaunching The Century of PatientsshaniaggrandPas encore d'évaluation
- PT Intake FormDocument4 pagesPT Intake FormChifor FlorinPas encore d'évaluation
- PsychopathologyDocument5 pagesPsychopathologyOzzyel CrowleyPas encore d'évaluation
- Pediatric OphthalmologyDocument12 pagesPediatric Ophthalmologyapi-3743483Pas encore d'évaluation
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreD'EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreÉvaluation : 4 sur 5 étoiles4/5 (1090)
- TherablocDocument3 pagesTherablocianecunar100% (2)
- Theorist Task Stage Patient Description 1. Erik Erikson Generativity vs. StagnationDocument8 pagesTheorist Task Stage Patient Description 1. Erik Erikson Generativity vs. StagnationRina CebreroPas encore d'évaluation
- Lesson Plan Personality DisorderDocument7 pagesLesson Plan Personality DisorderRaj MeghwalPas encore d'évaluation
- Siemens Acuson S3000 Ultrasound System BrochureDocument2 pagesSiemens Acuson S3000 Ultrasound System BrochureTanya Reynolds0% (1)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)D'EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Évaluation : 4.5 sur 5 étoiles4.5/5 (121)
- Recommendations For Good Practice in Ultrasound - 062019Document41 pagesRecommendations For Good Practice in Ultrasound - 062019RakhiPas encore d'évaluation
- Practice Nurse Vacancy Oct 2019Document2 pagesPractice Nurse Vacancy Oct 2019M LubisPas encore d'évaluation
- 10 Management of Patient With Hypoglycemic Coma. Management of Patient With Hyperglycemic (Ketoacidotic) ComaDocument59 pages10 Management of Patient With Hypoglycemic Coma. Management of Patient With Hyperglycemic (Ketoacidotic) ComaMimi ChukwuPas encore d'évaluation
- John O. Agwunobi MD Mba MPHDocument1 pageJohn O. Agwunobi MD Mba MPHStalyn DíazPas encore d'évaluation
- Coronary Artery Bypass SurgeryDocument3 pagesCoronary Artery Bypass Surgeryapi-355048975Pas encore d'évaluation
- Nursing Care Plan: Risk For InfectionDocument3 pagesNursing Care Plan: Risk For Infectiongeorgeborja414726100% (3)
- Thomasy & Lassaline EVE 2015 Equine Glaucoma Review ArticleDocument11 pagesThomasy & Lassaline EVE 2015 Equine Glaucoma Review ArticleMariana NunesPas encore d'évaluation
- Physiotherapy For Criticall IllnessDocument13 pagesPhysiotherapy For Criticall IllnessRatee Kumala100% (1)
- American College of Women's Health PhysiciansDocument16 pagesAmerican College of Women's Health PhysiciansSex & Gender Women's Health CollaborativePas encore d'évaluation
- Graduation ProjectDocument16 pagesGraduation Projectapi-357343808Pas encore d'évaluation
- Her Body and Other Parties: StoriesD'EverandHer Body and Other Parties: StoriesÉvaluation : 4 sur 5 étoiles4/5 (821)
- NCP Ineffective Airway ClearanceDocument2 pagesNCP Ineffective Airway ClearanceIsabel Barredo Del MundoPas encore d'évaluation
- FCP (Gorres)Document3 pagesFCP (Gorres)Kaloy KamaoPas encore d'évaluation
- Immunotec Whey To Go!: Immunotec Is Building An Empire On Patented ResultsDocument5 pagesImmunotec Whey To Go!: Immunotec Is Building An Empire On Patented Resultsapi-26034055Pas encore d'évaluation
- Pengembangan Format Pengkajian OremDocument20 pagesPengembangan Format Pengkajian OremMiftakhul KhoeryPas encore d'évaluation